
Abstract
Carotid percutaneous transluminal angioplasty/stenting has become an accepted treatment modality for carotid artery stenosis in high-risk patients. There has been an ongoing debate regarding which duplex ultrasound (DUS) criteria to use to determine the rate of in-stent restenosis. This prospective study revisits DUS criteria for determining the rate of in-stent restenosis. In analyzing a subset of 12 patients (pilot study) who had both completion carotid angiography and DUS within 30 days, 10 patients with normal post-stenting carotid angiography (< 30% residual stenosis) had peak systolic velocities (PSVs) of the stented internal carotid artery (ICA) of ≤ 155 cm/s and two patients with ≥ 30% residual stenosis had internal carotid artery (ICA) PSVs of > 155 cm/s. Eighty-three patients who underwent carotid stenting as part of clinical trials were analyzed. All patients underwent post-stenting carotid DUS that was done at 1 month and every 6 months thereafter. PSVs and end-diastolic velocities of the ICA and common carotid artery were recorded. Patients with PSVs of the ICA of > 140 cm/s underwent carotid computed tomographic (CT) angiography. The perioperative stroke rate was 1.2%. When the old DUS velocity criteria for nonstented carotid arteries were applied, 54% of patients had ≥ 30% restenosis (PSV of > 120 cm/s), but when our new proposed DUS velocity criteria for stented arteries were applied (PSV of > 155 cm/s), 33% had ≥ 30% restenosis at a mean follow-up of 18 months (p = .007). The mean PSVs for patients with normal stented carotid arteries based on CT angiography, were 122 cm/s versus 243 cm/s for ≥ 30% restenosis and 113 cm/s versus 230 cm/s for ≥ 30% restenosis based on our new criteria. The mean PSVs of in-stent restenosis of 30 to < 50%, 50 to < 70%, and 70 to 99%, based on CT angiography, were 205 cm/s, 264 cm/s, and 435 cm/s, respectively. Receiver operating curve analysis demonstrated that an ICA PSV of > 155 cm/s was optimal for detecting ≥ 30% in-stent restenosis, with a sensitivity of 100%, a specificity of 90%, a positive predictive value of 74%, and a negative predictive value of 100%. The currently used carotid DUS velocity criteria overestimated the incidence of in-stent restenosis. We propose new velocity criteria for the ICA PSV of > 155 cm/s to define ≥ 30% in-stent restenosis.
Keywords
In the past decade, carotid percutaneous transluminal angioplasty/stenting has become a widely accepted treatment modality for significant carotid artery stenosis in high-risk patients. 1–7 Early studies have reported the incidence of carotid in-stent restenosis to range between 1 and 50%. 8 These reported rates varied depending on the definition of restenosis, the method of stenosis calculations, and the duration of follow-up. We previously reported a high incidence rate of 32% for ≥ 50% carotid in-stent restenosis 9 when applying the standard carotid duplex ultrasound velocity criteria for nonstented carotid arteries (peak systolic velocity [PSV] of ≥ 140 cm/s). 10
There has been an ongoing debate regarding which duplex ultrasound criteria to use to determine the rate of restenosis after carotid stenting. 10–14
These few published studies reported on the potential source for errors when using the standard ultrasound criteria after carotid stenting since the reduced compliance of stented carotid arteries may produce falsely elevated velocities relative to the native nonstented carotid artery. Presently, standard duplex ultrasound velocity criteria have not been established for patients after carotid stenting. Therefore, we conducted the present study to revisit duplex ultrasound criteria for determining normal (0–< 30% stenosis) versus abnormal (≥ 30%) in-stent carotid restenosis.
Patient Population and Methods
In analyzing a subset of 12 patients (pilot study) who had both completion carotid angiography and carotid duplex ultrasonography within 7 days after stenting, 10 patients with normal post-stenting carotid angiograms (< 30% residual stenosis) had PSVs of the stented internal carotid artery (ICA) of ≤ 155 cm/s and 2 patients with ≥ 30% residual stenosis had ICA PSVs of > 155 cm/s. This study was conducted to develop new modified duplex velocity criteria to better define normal carotid (0–< 30%) versus abnormal (≥ 30%) carotid in-stent restenosis.
Eighty-three patients who underwent carotid stenting as a part of clinical trials (Maverick 1 and 2, Shelter, Parodi, CREST, and Capture trials) were analyzed. Patients underwent post-stenting carotid duplex ultrasonography at 1 month and then every 6 months thereafter. PSVs and end-diastolic velocities (EDVs) of the internal and common carotid arteries and the ICA to common carotid artery (CCA) PSV ratios were recorded. The velocities for the PSV ratio were taken as close as possible to the lesion.
The velocity criteria that are used in our vascular laboratory for differentiating normal to < 30% stenosis from abnormal (≥ 30% stenosis) for native nonstented carotid arteries were published previously. 15 PSVs of ≥ 140 cm/s of nonstented carotid arteries were compatible with ≥ 50% stenoses.
Patients with PSVs of the stented artery of > 140 cm/s underwent carotid computed tomographic (CT) angiography and/or conventional carotid arteriograms to verify the presence of in-stent restenosis.
For practical purposes, and to comply with the standard classification of carotid stenosis, we used the cutoff of < 30% stenosis to be normal (or minimal disease). Accordingly, carotid arteriography that was done at completion of the carotid stenting and/or carotid arteriography and/or CT angiography that was done at a later date were reviewed for the presence of < 30% stenosis versus ≥ 30% stenosis. Measurement of stenoses was calculated according to the North American Symptomatic Carotid Endarterectomy Trial, 16 basically by comparing the narrowest segment of the carotid stent to the diameter of the distal normal ICA where the wall becomes parallel. This study analyzed only patients with concurrent duplex sonograms that were done within 7 days of the post-stenting completion carotid arteriography and patients who had carotid duplex ultrasonography and CT angiography and/or carotid arteriography in the late follow-up, which were done within 30 days.
Statistical Analysis
The velocity data were expressed as mean ± standard deviation. Comparison of the duplex ultrasound velocity data with the angiographic stenoses was done using Fisher's exact method.
Receiver operating characteristic (ROC) curves were used to compare angiographic data with velocity measurements to determine the optimum velocity criteria for in-stent restenosis of ≥ 30%. Sensitivity, specificity, positive predictive value, negative predictive value, and overall accuracy were determined for the PSVs, EDVs, and the ICA to CCA ratio.
Results
Sixty-nine patients had ICA stenting and 14 had CCA stents (these were CCA bifurcated stents). Sixty-three percent were done for ≥ 70% asymptomatic carotid stenosis and 37% for strokes/transient ischemic attacks. Table 1 summarizes the clinical and demographic characteristics. The perioperative complication rate was 3.6%, with a perioperative stroke rate of 1.2% (Table 2). The mean follow-up was 18 months (range 1–54 months).
Demographics and Clinical Characteristics
CEA = carotid endarterectomy; TIA = transient ischemic attack.
30-Day Perioperative Complications
TIA = transient ischemic attack.
As noted in Table 3, when applying the original duplex criteria for nonstented carotid arteries (normal to < 30% has a PSV of < 120 cm/s), 15 46% were normal and 54% had ≥ 30% stenosis (45% had ≥ 50–< 70% stenosis, and 9% had ≥ 70 to 99% stenosis). However, when the new proposed duplex velocity criteria for stented arteries were applied (a PSV of ≤ 155 cm/s to define < 30%), 67% were normal and 33% had ≥ 30% in-stent restenosis. As noted in Table 3, 77% were normal (< 30%) and 23% were ≥ 30% on CT angiography. When the old nonstented velocity criteria were compared with CT angiography, the differences were statistically significant (p < .0001). However, when the new proposed stented duplex criteria were compared with CT angiography findings, there were no statistically significant differences (p = .19).
Comparison of Duplex Ultrasound Criteria for Restenosis
CT = computed tomography; PSV = peak systolic velocity.
Nonstented vs new stented criteria: p = .007.
New stented vs CT-angiography: p = .19.
Nonstented vs CT-angiography: p < .0001.
*Seven patients had > 50 to 99% based on angiography; four of these had midstent restenosis and three others at the end of the stent; all were identified by duplex ultrasonography.
The mean PSV for patients with normal stented carotid arteries, based on CT angiography, was 122 cm/s versus 243 cm/s for ≥ 30% restenosis (p < .0001). The mean PSV of a normal stented carotid artery based on our new proposed duplex criteria was 113 cm/s versus 230 cm/s for ≥ 30% restenosis (p < .0001; Table 4).
Mean Velocities and Internal Carotid Artery to Common Carotid Artery Ratios
CCA = common carotid artery; CT = computed tomography; EDV = end-diastolic velocity; ICA = internal carotid artery; PSV = peak systolic velocity.
*Abnormal vs normal PSV: p < .0001.
†Mean ± standard error of mean.
Comparison of abnormal PSVs (CT angiography vs duplex ultrasonography): p = .61.
Comparison of normal PSVs (CT angiography vs duplex ultrasonography): p = .13.
Table 5 summarizes the mean velocities and ICA to CCA ratios for ≥ 30 to < 50%, ≥ 50 to < 70%, and ≥ 70 to 99% in-stent restenosis, based on CT angiography.
Computed Tomography Angiography Stenosis versus Velocities and Ratio
CT = computed tomography; EDV = end-diastolic velocity; PSV = peak systolic velocity.
ROC Curves: Sensitivity and Specificity of Various Velocity Criteria
Peak Systolic Velocity
As noted in Table 6, a PSV of ≥ 155 cm/s was optimal in detecting ≥ 30% in-stent restenosis, with a sensitivity of 100%, a specificity of 90%, a positive predictive value of 74%, and a negative predictive value of 100%, with an overall accuracy of 92%. Figure 1 shows the ROC curve for the sensitivity and specificity of the PSV values. As noted, using a cutoff of 155 cm/s, the area under the curve was equal to 0.96, with a standard error of 0.03 (95% confidence interval 0.895–0.99). A larger area under the ROC curve is a measure of improved discrimination.

Receiver operating characteristic curve for peak systolic velocity (PSV). AUC = area under the curve; C.I. = confidence interval; SE = standard error.
Peak Systolic Velocity Sensitivity and Specificity
ICA = internal carotid artery; PSV = peak systolic velocity.
Numbers in bold indicate that a peak systolic velocity ≥ 155 cm/s was optimal in detecting in-stent restenosis ≥ 30%.
End-Diastolic Velocities
Table 7 illustrates the sensitivity and specificity for the EDVs. As noted, an EDV of ≥ 42 has a sensitivity of 70%, a specificity of 82%, a positive predictive value of 54%, and a negative predictive value of 90%, with an overall accuracy of 79%. Figure 2 shows the ROC curve for the sensitivity and specificity of the EDVs. Using a cutoff value of 42 cm/s, the area under the curve was equal to 0.8, with a standard error of 0.7 (95% confidence interval 0.668–0.854).

Receiver operating characteristic curve for end-diastolic velocity (EDV). AUC = area under the curve; C.I. = confidence interval; SE = standard error.
End-Diastolic Velocity Sensitivity and Specificity
EDV = end-diastolic velocity; ICA = internal carotid artery.
Numbers in bold indicate that a peak systolic velocity ≥ 42 cm/s was optimal in detecting in-stent restenosis ≥ 30%.
Peak Systolic Velocity ICA to CCA Ratio
Table 8 summarizes the sensitivity and specificity of the PSV ICA to CCA ratio, and, as noted, a value of ≥ 1.49 had a sensitivity of 75%, a specificity of 73%, a positive predictive value of 46%, and a negative predictive value of 91%, with an overall accuracy of 74%. Using a cutoff of ≥ 1.49 ±, the area under the curve equals 0.76, a standard error of 0.7 (95% confidence interval 0.657–0.845; Figure 3). Figure 4 compares the ROC curves for the PSVs, EDVs, and the ICA to CCA ratio. As noted, the PSV values were statistically significantly superior to both the EDV values and the ICA to CCA ratios.
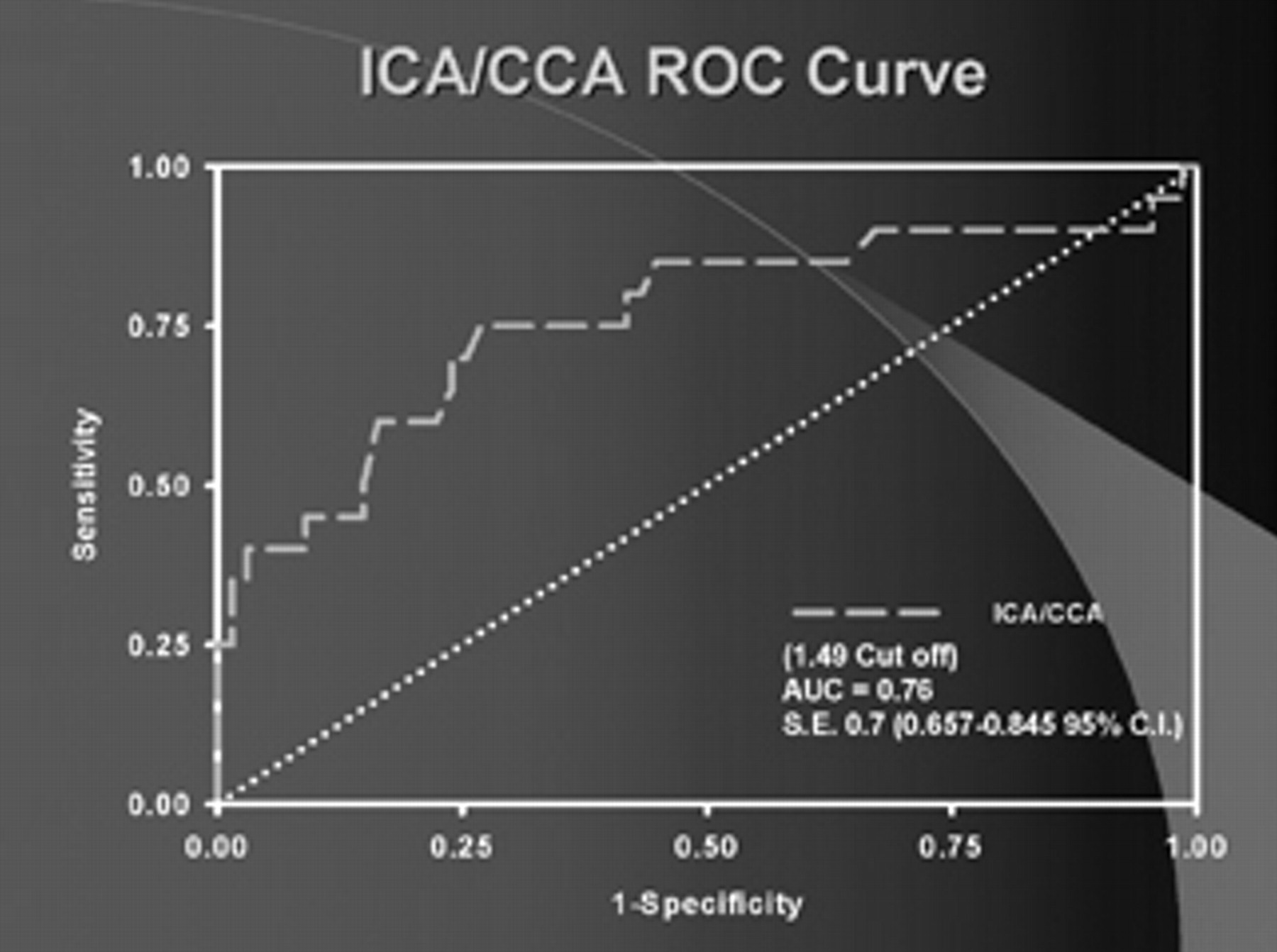
Receiver operating characteristic curve for the internal carotid artery to common carotid artery ratio (ICA/CCA). AUC = area under the curve; C.I. = confidence interval; SE = standard error.

Receiver operating characteristic curve comparison. EDV = end-diastolic velocity; ICA/CCA = internal carotid artery to common carotid artery ratio; PSV = peak systolic velocity.
Peak Systolic Velocity Internal Carotid Artery to Common Carotid Artery Ratio Sensitivity and Specificity
CCA = common carotid artery; ICA = internal carotid artery; PSV = peak systolic velocity.
Numbers in bold indicate that a peak systolic velocity ≥ 1.49 cm/s was optimal in detecting in-stent restinosis ≥ 30%.
Discussion
Although carotid angiography can be used for follow-up in patients with carotid artery stenting, most physicians prefer noninvasive evaluation using duplex ultrasonography. The duplex ultrasound technique is noninvasive, safe, readily available in all vascular laboratories, and free of complications. It has been used for the diagnosis of extracranial carotid artery disease for over 25 years. The appropriate threshold velocities defining various degrees of stenoses have been analyzed, leading to the use of specific PSVs, EDVs, and/or PSV to EDV ratios to define various categories of carotid artery stenosis.
Presently, duplex ultrasonography can be used to examine stented carotid arteries. In spite of the stent material being highly reflective, it does not produce any significant artifact to limit visualization. Duplex ultrasonography can noninvasively provide imaging details of the stent and vessel wall characteristics, as well as any abnormalities. Although the cause of elevated ICA PSVs in the absence of disease is uncertain, it has been speculated that the stent may decrease the compliance of the carotid artery. In addition, because the plaque is not removed with angioplasty and stenting, this may also add to a decreased compliance and elevation of velocities. Although B-mode imaging data are useful, the primary ultrasound parameters used in most vascular laboratories to diagnose the severity of carotid artery disease have been the hemodynamic parameters, that is, the PSV, EDV, and ICA to CCA ratio, alone or in combination.
In spite of the use of several carotid stents worldwide and in the United States, duplex ultrasound velocity criteria have not been well established or standardized for patients undergoing carotid artery stenting. In an earlier study by Robbin and colleagues, they concluded that the use of duplex ultrasonography in the follow-up of stented carotid arteries was unreliable in defining in-stent restenosis based on variable velocity measurements. 11 Ringer and colleagues also reviewed their experience after carotid stent placement and concluded that strict velocity criteria for restenosis were unreliable. 13
When we initially applied our Intersocietal Commission for the Accreditation of Vascular Laboratories–accredited vascular laboratory duplex velocity cutoff PSV of ≥ 140 cm/s criterion, which was developed for native nonstented carotid arteries to distinguish between < 50% versus ≥ 50%, 15 32% of our patients were felt to have ≥ 50% in-stent restenosis (PSV of ≥ 140 cm/s). When the same old duplex velocity criteria for nonstented carotid arteries were applied in the present study, 54% of patients had ≥ 30% restenosis. With the proposed new duplex velocity criteria for stented arteries (PSV of > 155 cm/s, to define ≥ 30% restenosis), 33% were felt to have ≥ 30% in-stent restenosis at a mean follow-up of 18 months. The accuracy of these newly defined PSVs of stented carotid arteries was very comparable to carotid arteriography and/or CT angiography. These proposed criteria can form the basis for additional prospective validation studies to further classify the degree of stenosis beyond 30%. In spite of the limited number of the abnormal studies (≥ 30%) in our patients, there was a tendency for higher PSV of the ICA with the higher degree of stenoses as noticed in Table 5.
Although we did not specifically analyze the differences between the baseline velocities and the late follow-up velocities, there was a tendency for the PSVs to increase over time in patients with a documented higher degree of stenosis.
The present study has several limitations, including the relatively small sample size and the use of CT angiography instead of conventional arteriography in some of our patients; however, several studies have compared the accuracy of CT angiography with conventional arteriography and found them comparable. 17,18 Another limitation of this study is the limited number of patients with high-grade stenosis, which did not enable us to further classify stenoses into higher categories, that is, 50 to < 70% stenosis and 70 to 99% stenosis.
Until new proposed revised criteria for carotid stenting are standardized, it is mandatory for follow-up duplex ultrasound velocities to be compared with earlier post-stenting studies. Persistent elevation of PSVs may be the clue for progressive in-stent carotid restenosis and should be clinically managed accordingly.
Conclusions
Our data demonstrated that a significant portion of stented carotid arteries will display elevated PSVs that are greater than the accepted normal value for a native carotid artery. Raising the velocity threshold for PSVs in stented ICAs is warranted. Our present study indicates that a PSV of > 155 cm/s was highly suggestive of carotid in-stent restenosis of ≥ 30%. Early registration of baseline velocities to compare subsequent follow-up velocities of the stented carotid artery is ideal. Elevation in PSVs and/or ICA to CCA ratios may be indicative of developing in-stent restenosis, which may then undergo angiographic evaluation and management, if clinically indicated.
Footnotes
Presented in part at the 20th Annual Meeting of the Eastern Vascular Society, Washington, DC, September 28–30, 2006.