
Abstract
Aortitis is an inflammatory condition that can be due to numerous causes. It is a diagnostic quandary because it commonly shows similar clinical, pathologic, and aortographic features independently of the etiology. A case of aortitis, possibly secondary to bacterial endocarditis, initially misdiagnosed as an atherosclerotic aortic ulcer and managed with an endoprosthesis is presented. On the fourth postoperative day, the patient presented with fever and worsening abdominal pain, which was later diagnosed as infectious aortitis. It required débridement and replacement of the infrarenal aorta with a cadaveric cryopreserved allograft. This case emphasizes the need for early diagnosis and aggressive therapy to avoid life-threatening sequelae.
Keywords
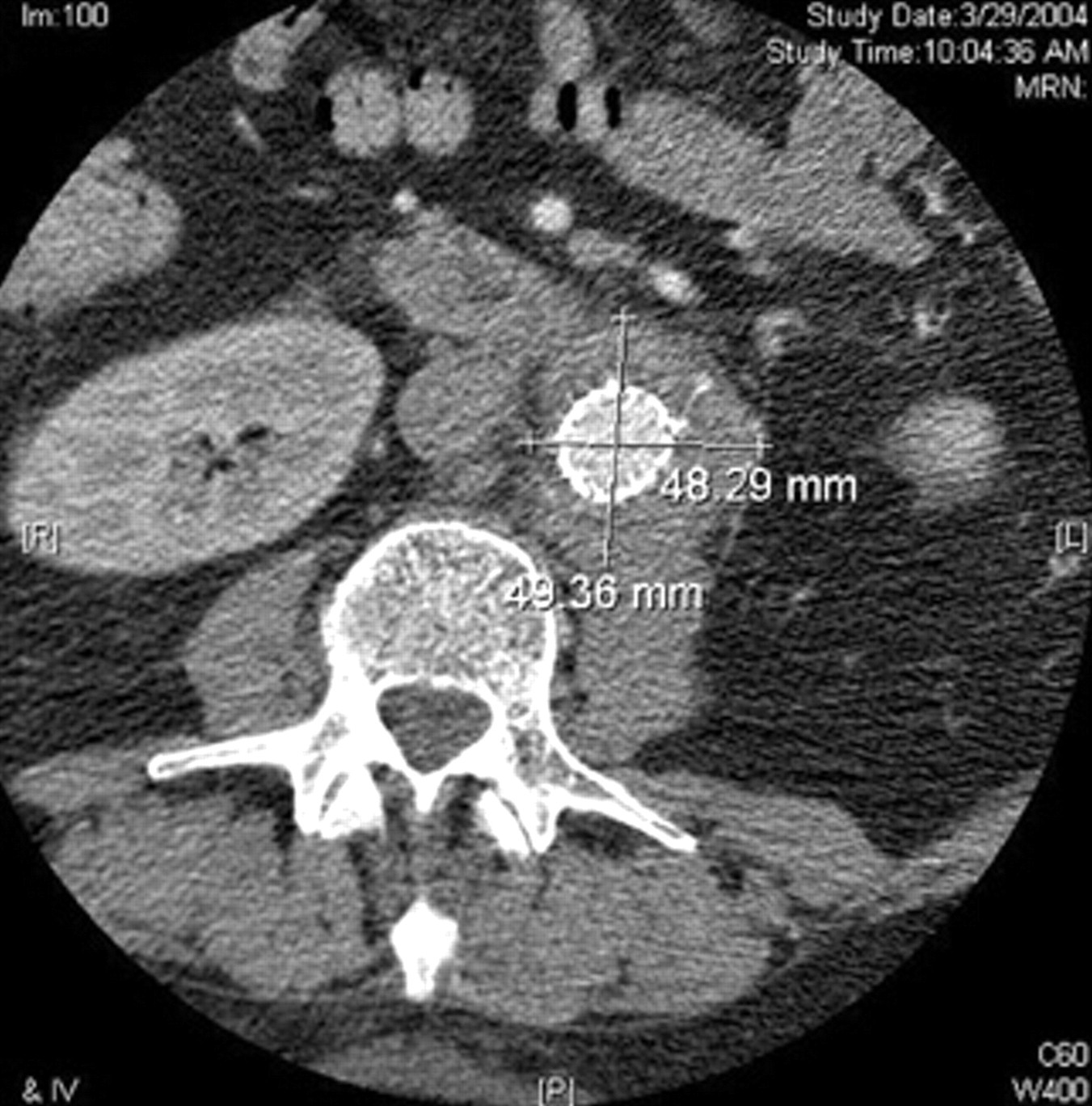
A 57-year-old male presented with acute onset of diffuse abdominal pain but was hemodynamically stable. His history was noncontributory. An abdominal computed tomographic (CT) scan showed aortic atherosclerosis and periaortic inflammation below the renal arteries origin extending into the bifurcation (Figure 1). An area of focal abnormality in the lumen of the aorta was seen below the inferior mesenteric artery origin measuring 4.5 × 5 mm. His blood work was normal except for a white blood cell count (WBC) of 17,500 cells/μL. He was admitted and started on intravenous beta-blockers for blood pressure control and empiric antibiotic therapy. Blood and urine cultures were negative, and 12 hours after admission, his WBC normalized. His antibiotics were stopped since no definite evidence of infection was demonstrated. A CT scan 5 days later showed that the radiographic abnormality increased in size (10 × 6 mm). The working diagnosis was that of a penetrating aortic ulcer with periaortic inflammatory reaction. In addition, although rare, primary aortic tumors were also considered. Given the progression of the radiographic findings, endovascular exclusion of the penetrating aortic ulcer was planned. This was successfully performed using the Gore Excluder endoprosthesis (W. L. Gore & Associates, Inc. Flagstaff, AZ), as shown by intraoperative imaging (Figure 2).

An abdominal computed tomographic scan reveals aortic atherosclerosis and periaortic inflammation, consistent with an infectious versus atherosclerotic etiology.

Intraoperative completion angiography shows successful endovascular exclusion of the penetrating aortic ulcer using the Gore Excluder endoprosthesis.
Postoperatively, the patient developed an intermittent low-grade fever that resolved in 2 days. Blood and urine cultures were negative. Transthoracic echocardiography was performed, with inconclusive results. Consequently, transesophageal echocardiography (TEE) was suggested but was not done owing to the patient's refusal. He was subsequently discharged with plans to repeat a CT scan 2 weeks after intervention. Four days later, he was admitted because of worsening abdominal pain, an elevated WBC, and a fever. Abdominal CT scan revealed increased periaortic inflammation in the infrarenal aorta (Figure 3). CT scan–guided, translumbar aspiration was performed, obtaining purulent material identified on immediate stain as gram-positive staphylococci in clusters. The patient was immediately taken to the operating room. Large amounts of inflammatory tissue with purulence were found. On entering the aorta, the previously placed endograft was found without incorporation. A healthy infrarenal neck was able to be seen after débridement and endograft excision. He underwent radical retroperitoneal débridement and replacement of the infrarenal aorta with cadaveric cryopreserved allograft (Figure 4). Intraoperative aortic tissue cultures revealed pan-sensitive Staphylococcus aureus. Pathology reported atherosclerotic aortic calcification with marked acute and chronic periaortic inflammation. The patient had a postoperative course without complications. Postoperative TEE showed a very small mitral valve vegetation. He was discharged on lifelong oral antibiotics 9 days after the operation. At his first visit at 2 weeks, he was asymptomatic. A CT scan performed 19 days after discharge showed almost total resolution of the aortitis, and another one about 4 months after intervention showed a complete lack of inflammation (Figure 5). He is followed yearly with clinical examinations and imaging surveillance consisting of CT scans for the first 2 years and duplex ultrasonography thereafter.
Repeated abdominal computed tomographic scan, now showing the presence of an aortic stent graft and worsening of the inflammatory process around the aorta. Translumbar aspiration in the same setting revealed the presence of Staphylococcus aureus.

Intraoperative photograph showing the final appearance of a cadaveric cryopreserved allograft used for aortic reconstruction.

Computed tomographic scan of the abdomen performed 4 months after interventioin, showing complete resolution of the infectious aortic process.
Discussion
Aortitis is an inflammatory process that involves one or more layers of the aortic wall caused by several etiologies, 1–5 mainly infectious. 6–9 Aortic aneurysm infections were described initially in 1885. 10 However, nonaneurysmal aortitis, such as in the case of our patient, is exceedingly rare. Its clinical manifestations are nonspecific, and a high suspicion index is required for its diagnosis. Albeit unusual, primary aortic tumors should be considered. Reported tumor cases described an intraoperative appearance indistinguishable from that of inflammatory aortitis. 11
Different imaging modalities are available for the diagnosis of aortitis. Traditionally, aortography has been performed, but echocardiography, magnetic resonance imaging, contrast-enhanced CT scan, and positron emission tomography are being used with increasing frequency. 12–16 Pathologic examinations can assist in the diagnosis when tissue is available. However, the diagnosis of aortitis is difficult because of nonspecific clinical, pathologic, and aortographic findings. Furthermore, the infectious or inflammatory nature of an aortitis is difficult to assert because the microbiologic results are often negative.
Historically, aortitis was uniformly fatal. The association between endocarditis and aortitis is becoming rare, and mortality rates have fallen after the antibiotic era. 17 Beta-lactams are the drugs of choice for staphylococcal endocarditis and aortitis, as shown experimentally. 18 Currently, aortitis usually presents in men between 50 and 70 years old, often immunocompromised, with Staphylococcus or Salmonella superinfection of an atherosclerotic or aneurysmal aorta. 19 It is difficult to ascertain with precision if the aortitis in the case of our patient arose from endocarditis or if the latter was a consequence of the severe arterial infection, especially when the cardiac vegetation was small and was not initially detected by TEE.
Early diagnosis and aggressive therapy are needed to avoid life-threatening complications. The treatment of aortitis is determined by the underlying cause: antibiotics and surgery for infectious causes and immunosuppression and surveillance for autoimmune problems. In this patient, the absence of fever or positive blood cultures during his initial presentation, as well as the delay in obtaining tissue sampling, caused a misdiagnosis for atherosclerotic ulceration. In retrospect, immediate surgical exploration or CT-guided aspiration of the periaortic tissue during the first admission would have made the correct diagnosis in a timely fashion. As stated previously, the diagnostic challenge that faced us with this patient is not unheard of. 8,20 Often infections of the aorta are diagnosed only after an extensive workup under the presumption of noninfectious aortitis, but after clinical deterioration, an infectious origin is found, either before or at the time of surgery.
The management of penetrating ulcers in the abdominal aorta is controversial. Little is known about their natural history, 21 and most of the available information is extrapolated from experience managing thoracic aortic ulcers. Some authors advocate conservative management, 22–24 others recommend surgical repair, 25 and, more recently, endovascular management has become another option and even the first choice at some centers. 26,27
Treatment strategies for infectious aortitis include extra-anatomic grafting followed by staged excision of the infected aortic segment, 28 in situ reconstruction using rifampin-bonded grafts, 29 autogenous tissues, 30 cryopreserved arterial 31 or venous 32 allografts, and endovascular techniques. 33,34
The use of arterial allografts, either fresh or cryopreserved, in the surgical treatment of aortic infections has been extensively documented. Most series include primary aortic graft infections, mycotic aneurysms, aortoenteric erosions, and aortic reconstructions performed concomitantly with bowel repair, making the precise assessment of their efficacy in the sole therapy of primary aortitis difficult. In general, the reported results show acceptable results in terms of 30-day and overall morbidity and mortality (Table 1). 31,35–41 Also, others have shown benefits in terms of duration of intensive care per year of follow-up, hospitalization, duration of postoperative antibiotic therapy, costs, and elimination of infection when directly compared with traditional extra-anatomic reconstruction using prosthetic material. 42 Some authors consider the use of cryopreserved allografts to treat aortic infections as their primary alternative and find this approach to be at least as effective as the other traditional surgical strategies. 43,44
Aortic Allografts Used for Infected Aorta
*Patency assumed equivalent to survival in this article (30 day: 84.6%; overall: 77%).
S. aureus infection of the aorta has been identified as one of the risk factors associated with poor hospital survival after surgical therapy. 45 Six weeks of antibiotics directed by the minimum inhibitory and bactericidal concentration of these agents for the causative organisms has been suggested. 46 Lifelong oral antibiotics for this patient can be seen as an exaggeration. However, there are no available data to support the benefit of shorter courses in cases of endocarditis associated with ruptured aortitis.
Conclusions
The diagnosis of infectious aortitis is not always straightforward. In cases in which no definite evidence of infection is demonstrated, early surgical exploration or CT-guided aspiration prevents misdiagnosis and unnecessary delays in treatment. The use of cryopreserved allografts appears to be an acceptable alternative to traditional in situ or extra-anatomic approaches. Intensive postoperative imaging surveillance is mandatory. Increased awareness of the possibility of aortitis and the importance of early and precise identification of its cause cannot be overemphasized.