
Abstract
Endovascular repair of thoracic aortic aneurysm has become an important treatment modality in patients who are at increased risk for open surgical repair. Since the US Food and Drug Administration (FDA) approved the clinical application of this technology in the thoracic aorta in 2005, there has been a rapid growth in this treatment modality as numerous endovascular devices have been introduced in the application of thoracic aortic pathology. Although thoracic aortic aneurysm is the only FDA-approved treatment indication for endovascular repair, this technology may lead to a broader clinical applicability in other thoracic pathologies. This article reviews the current endovascular devices designed for the treatment of thoracic aortic pathology. These devices are described, and the current clinical results are discussed.
Keywords
Since the US Food and Drug Administration (FDA) approved the commercial use of a thoracic endograft device in the treatment of thoracic aortic aneurysms in 2005, 1 it has broadened the therapeutic strategies in patients with thoracic aortic disease. Endovascular repair of thoracic aortic aneurysm offers many practical benefits and technical advantages compared with the conventional open thoracotomy. Deployment of a thoracic endograft in the descending aortic aneurysm, particularly in patients with adequate proximal and distal aortic neck landing zones, can be accomplished in a straightforward manner. In patients with suitable ileofemoral artery access, this procedure can even be performed under local anesthesia without incurring significant cardiopulmonary stress. Frequently encountered physiologic insults associated with an open repair, such as thoracotomy, aortic cross-clamping, left-heart bypass, and single-lung ventilation, can all be avoided in the setting of an endovascular thoracic aortic endografting procedure. Exclusion of a descending aortic aneurysm with an endograft does not necessitate cross-clamping the thoracic aorta. As a result, the avoidance of aortic cross-clamping minimizes significant blood pressure shifts and coagulopathy. This also reduces operative blood loss and ischemic events involving the spinal cord, viscera, and kidneys. An additional advantage of endovascular repair, which is in sharp contrast to an open operation, includes reduced systemic anticoagulation with heparin during the procedure. This is particularly beneficial in patients with traumatic aortic injuries who have concomitant intracranial or abdominal injuries. Lastly, patients who had endovascular thoracic procedures experienced a significantly shorter convalescent period compared with those who underwent open repair, which is a comparable and well-recognized benefit documented in studies of endovascular abdominal aortic aneurysm (AAA) repair.
These perceived benefits of endovascular thoracic repair have generated enormous interest in developing the ideal device for thoracic aortic pathology. Many endovascular manufacturers have launched their respective endograft and clinical investigation to validate the efficacy of the device. This article provides a brief overview of various endovascular thoracic endografts and available clinical studies supporting their utility. The devices that are discussed herein include the Gore TAG Endoprosthesis (W.L. Gore & Associates, Flagstaff, AZ), the Talent Thoracic Stent Graft (Medtronic, Santa Rosa, CA), the Zenith TX2 Stent-graft (Cook Inc., Bloomington, IN), and the Relay Thoracic Stent-Graft (Bolton Medical, Sunrise, FL).
Gore TAG Endoprosthesis
The initial feasibility trial of the Gore TAG Endoprosthesis was completed in the United States in 1998, followed by the pivotal trial in 1999. 2 Following a voluntary withdrawal by the manufacturer in 2001 owing to the discovery of fractures involving the longitudinal deployment stent, a modified device was reintroduced after a confirmatory trial in late 2003. It became the first commercially approved thoracic device in the United States as the FDA granted its approval for clinical application in 2005. 1
Device Description
The Gore TAG Endoprosthesis is composed of a symmetric expanded polytetrafluoroethylene (ePTFE) tube externally reinforced with a layer of ePTFE and fluorinated ethylene propylene (FEP) (Figure 1). An exoskeleton consisting of nitinol stents is attached to the entire external surface of the graft with ePTFE-FEP bonding tape. Both the proximal and distal segments of the endograft have scalloped flares, which are to facilitate endograft conformity in a tortuous thoracic aorta. Two radiopaque gold bands are attached to the base of the flares, serving as a guide during deployment and in graft surveillance. A polytetrafluoroethylene sealing cuff, which is affixed to the base of the flares, is attached on one end with FEP, whereas the other end is allowed to remain free. This is designed to enhance the device attachment to the aortic wall and potentially reduce type 1 endoleaks.
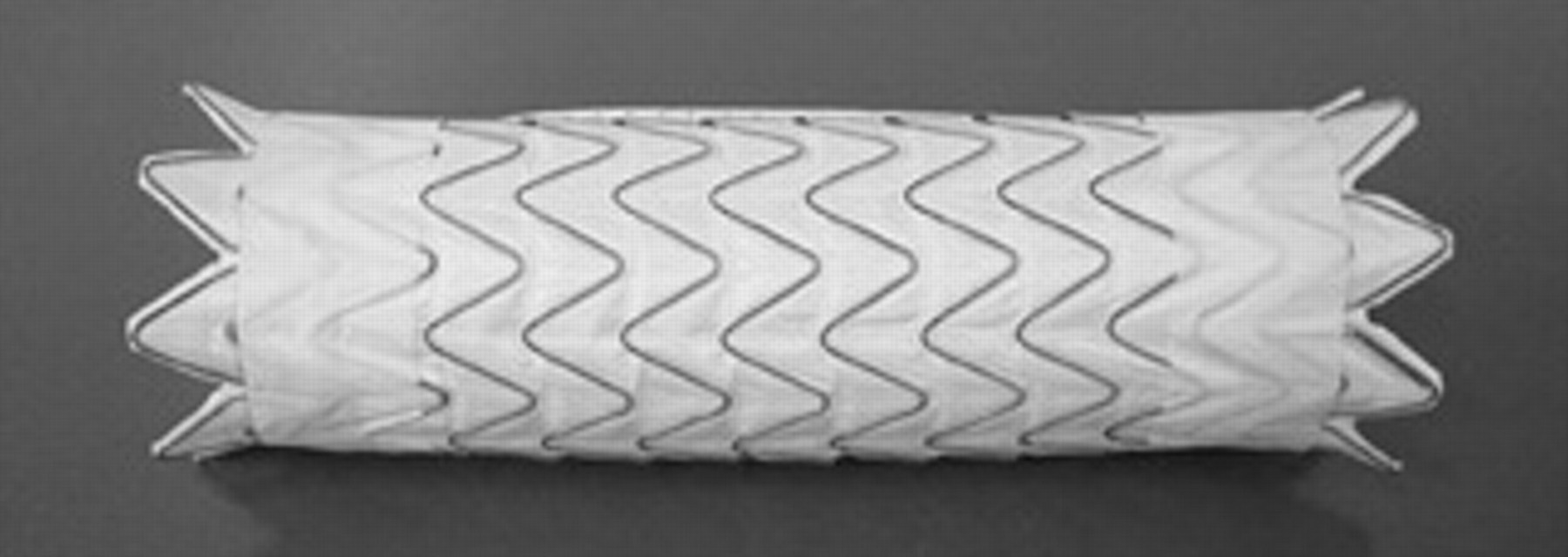
The Gore TAG endoprosthesis.
This device contains a unique deployment mechanism in which the endograft is constrained by an ePTFE-FEP sleeve connected to a deployment knob located at the control end of the delivery catheter (Figure 2). Release of the endograft begins in the midgraft region to reduce distal displacement via a “windsock” effect. Following device deployment, a unique trilobed balloon, which permits continuous antegrade aortic blood flow during balloon inflation, is used to ensure full device attachment to the aortic wall (Figure 3). The flexible catheter delivery system and the rapid deployment mechanism are potentially beneficial, particularly for deployment in curved segments of the aorta within or close to the aortic arch. The delivery system and compatible introducer sheaths vary according to the diameter of the device and scale over a range of 20F to 24F sheath. Grafts are available in diameters ranging between 26 and 40 mm, and lengths are available in 10, 15, or 20 cm.
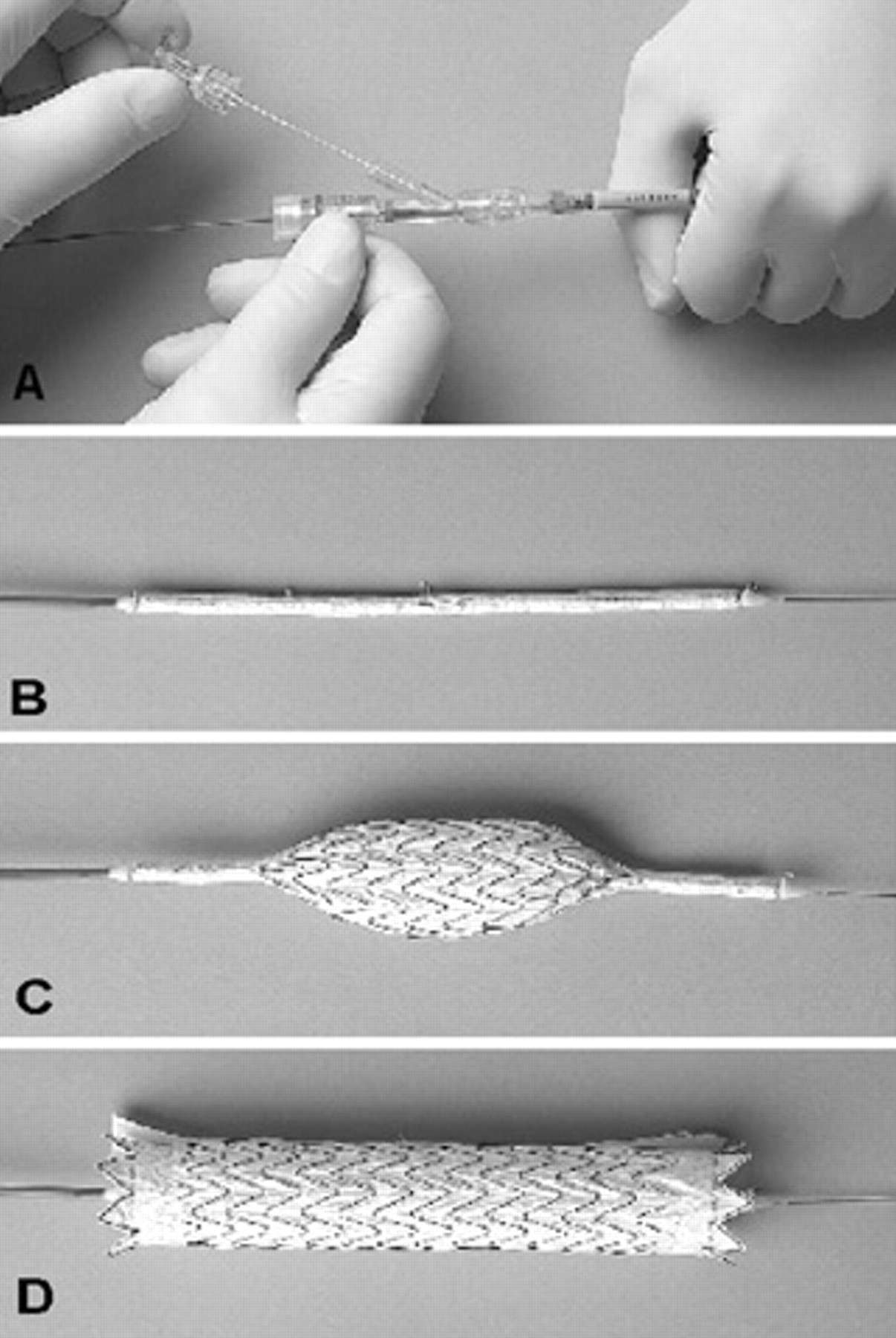
Deployment of the Gore TAG endoprosthesis. A, Initial deployment involves turning and pulling the deployment knob. B, The endoprosthesis is fully constrained on the delivery catheter. C, The stent graft is deployed from the middle segment, expanding outward. D, Fully deployed thoracic device.

A trilobed balloon is used to inflate the aortic stent graft while allowing continuous antegrade blood flow during balloon inflation.
Brief Clinical Results
The feasibility study was conducted between 1998 and 1999 to establish preliminary device safety data and included 28 patients at two clinical sites. At 30 days, there was one mortality and no paraplegia or stroke. At the 1-year follow-up, the all-cause mortality rate was 21%, with no aneurysm-related mortality. There was an 8% rate of sac enlargement with stent fracture in 32%.
A phase II pivotal trial was conducted between September 1999 and May 2001 and was halted when the high rate of longitudinal wire fractures was detected. This study was a prospective, multicenter, nonrandomized study that evaluated the safety and efficacy of the Gore TAG Endoprosthesis in 17 institutions for the treatment of descending thoracic aortic aneurysm in 142 patients compared with an open surgical repair group of 94 patients. 2 The primary safety end point was the percentage of patients with more than one major adverse event (MAE) through 1 year post-treatment. The primary efficacy end point was the percentage of patients free from major device-related events through the 1-year follow-up for the TAG group. One hundred thirty-nine (98%) of 142 patients had successful implantation of the device. Inadequate arterial access was responsible for the three failures. A conduit was placed to facilitate access in 21 patients (15%). Operative mortality, defined as death within 30 days of the procedure or during the same hospitalization, occurred in 3 (2.1%) patients after a TAG repair and was significantly lower than in the surgical control group, with a mortality rate of 11.7%. Within 30 days of the operation, 45 (32%) patients had at least one MAE: 5 (4%) experienced a stroke, 4 (3%) demonstrated temporary or permanent paraplegia, 20 (14%) experienced vascular trauma or thrombosis, and 2 (1.5%) died. The mean follow-up was 24.0 months. The 2-year all-cause mortality rates were comparable between the TAG and open surgical groups, which were 24% and 26%, respectively. The incidence of MAEs at the 1-year follow-up was significantly lower in the TAG group compared with the surgical controls, which were 42% versus 77%, respectively. The majority (70%) of MAEs were noted to have occurred within 30 days of the original procedure. This advantage to the TAG group persisted through the 3-year follow-up. Kaplan-Meier estimates of the probability of freedom from MAEs at 3 years were 48% after TAG repair and 20% after open repair. During the 3-year follow-up, five patients underwent endovascular revisions and one patient underwent open surgical conversion. Twenty fractures were noted in 19 patients, 18 of which were in the longitudinal spine and 2 in the apical nitinol support tings. Clinical sequelae developed only in one patient, who manifested a type 3 endoleak that was successfully treated with an additional endograft. There were no device-related deaths noted through the 3-year follow-up. Based on the findings of this study, the authors concluded that the Gore TAG Endoprosthesis represents a safe alternative for the treatment of descending thoracic aneurysms, with remarkable 2-year freedom from aneurysm-related death. 1–3
The confirmatory trial was performed after the reintroduction of the modified device in 2003 to compare the safety and early results of the modified device with the original device. This was a prospective nonrandomized trial performed on 51 patients at 11 test sites, who were compared with the 94 control subjects used in the pivotal study. 3 At the 30-day follow-up, the incidence of MAEs was noted to be 12% in the TAG group and 70% in the control group. This was a statistically significant difference corresponding to an 83% risk reduction for those with TAG repair, although risk classification according to the American Society of Anesthesiologists (ASA) was very similar between both groups and the Society for Vascular Surgery risk score was slightly higher in the TAG group. There were no deaths. There were no major device-related events noted at the 30-day follow-up. This is in comparison with the 4% major device-related complication rate reported in the pivotal study (4%). 3 Based on the anatomic inclusion criteria with a 2 cm landing zone in the proximal and distal aortic neck, patients with descending thoracic aortic aneurysms enrolled in this confirmatory study and other multicenter trials uniformly had an excellent outcome when treated with the Gore TAG endograft devices. 1–3 The 2 cm landing zone in a normal thoracic aorta proximal and distal to an aneurysm is a critical anatomic consideration when placing a thoracic endograft device, and this serves as an important criterion in the device's instructions for use (IFU).
Since the TAG device was approved by the FDA in March 2005, the device has been increasingly used in practice for the treatment of different thoracic aortic pathologies. Experiences from various institutions using this device within the various clinical scenarios and indications are being continuously added to the literatures. 4–7 From our own institutional experience, 128 patients have undergone successful endovascular thoracic repair using the Gore TAG device since March 2005. Among them, 86 patients had a descending thoracic aortic aneurysm with anatomy suited for the device's IFU. The remaining 42 patients had an unsuitable landing zone, with thoracic aneurysms extending either proximally to the aortic arch (n = 25) or distally to the celiac artery (n = 17). These patients underwent aortic debranching procedures in which either the left carotid bypass was debranched to increase the proximal landing zone or the visceral arteries were relocated to increase the distal landing zone. The clinical outcome of these patients who underwent aortic debranching procedures to accommodate Gore TAG device implantation was previously reported. 8,9 The overall mean aortic aneurysm diameter was 6.7 ± 3.2 cm. Technical success was achieved in all patients. Among the 86 patients whose aortic anatomy was within the recommended IFU, one device was used in 43% of patients, whereas 57% required two or more endografts to cover the thoracic aneurysm. The mean intensive care unit (ICU) stay was 2.5 days, whereas the overall hospital stay was 6.4 days. Within 30 days, 14 (16%) patients had at least one MAE, which included 4 (4.7%) patients with renal insufficiency, 2 (2.3%) patients with transient paraplegia, 5 (5.8%) patients with stroke, and 3 (3.5%) patients with femoral artery trauma that necessitated iliofemoral bypass. Among the 42 patients who required either aortic arch vessel or visceral debranching operation to lengthen the device landing zone, significantly greater MAEs were noted, which occurred in 12 (29%) patients. Among them, four (9.5%) patients developed myocardial infarction, five (11.9%) patients developed renal insufficiency, three (7.1%) patients developed transient or permanent paraplegia, and two (4.8%) patients developed stroke. Based on our experience, an excellent clinical outcome can be achieved when using the Gore TAG Endoprosthesis in patients with a descending thoracic aortic aneurysm when endograft placement is based on the device's IFU, a finding that was confirmed by other series. 3,4,10,11 When treating patients with an inadequate proximal or distal landing zone, however, surgeons must be cautious as efforts to lengthen these landing zones by performing aortic arch or visceral debranching operations can still result in relatively high perioperative complication rates.
Medtronic Talent Thoracic Stent Graft System
The clinical feasibility trial of the Talent stent graft system was initiated in the United States in 1998. 12 This clinical study, also known as the VALOR trial (Vascular Talent Thoracic Stent Graft System for the Treatment of Thoracic Aortic Aneurysms), recently completed the enrollment of three study arms. The Talent endograft system evaluated in the VALOR trial has been used extensively outside the United States for many years. The manufacturer is preparing to introduce the next generation of their thoracic endograft device, which is called the Valiant Stent Graft, into US clinical trials. The evolution of the Talent Thoracic Stent Graft to the Valiant device is based in part on the accumulated clinical experience from device implantation worldwide.
Device Description
The Talent Thoracic Stent Graft system is composed of a self-expanding serpentine-shaped nitinol endoskeleton inlaid in a woven polyester graft. 13,14 The Talent has a longitudinal support bar throughout the length of the endograft, which provides column strength while maintaining device flexibility to accommodate tortuous vessels. Individual stents are secured to the graft with suture (Figure 4). Between individual stents is an unsupported graft to allow for flexibility. The proximal end of this stent graft is made in two configurations, which include either a serrated (open web configuration) or an open bare stent segment (FreeFlo configuration). The bare stent FreeFlo configuration allows device implantation across the orifice of the left subclavian or common carotid artery while maintaining antegrade blood flow. A similar bare wire configuration is also available in the distal stent graft, which permits the uncovered device to anchor across the celiac artery. The delivery systems for the Talent have profiles between 22F and 25F. The Talent system consists of two device components. The proximal device is a straight tube stent graft with proximal FreeFlo configuration. The proximal device is available in diameters of 22 to 46 mm with a 2 mm increment.

The Medtronic Talent thoracic stent graft.
The covered lengths of the proximal device range from 112 mm (largest diameter) to 116 mm (smallest diameter). In contrast, the distal Talent device is a tapered tube endograft system with a 4 mm difference in diameter between the proximal and distal orifices. The proximal orifice of the distal Talent device has an open web configuration, whereas the distal orifice of the same component has a closed web configuration (Figure 5). The distal Talent device is available in diameters ranging from 22 to 44 mm in 2 mm increments. The covered lengths of the distal Talent endograft range from 110 mm (largest diameter) to 114 mm (smallest diameter).
The Medtronic Talent stent graft system consists of two components. The proximal stent graft device is a straight tubular endograft with proximal FreeFlo bare stent configuration. The distal stent graft component is a tapered tubular endograft with an open web proximal configuration and closed web distal configuration.
Precise deployment of the thoracic endograft in the vicinity of the aortic arch is of fundamental importance to prevent device-induced cerebral embolization. In an effort to improve deployment accuracy and technical ease, the long connecting bar of the Talent device has been removed in the Valiant device, whereas columnar support has been optimized through stent spacing and the exoskeleton. The removal of the connecting bar enables the device to become more flexible. Additionally, it has eliminated the need to orient the device in the aorta owing in part to its enhanced flexibility. The Valiant stent graft has a modified proximal FreeFlo configuration with eight bare peak wires compared with the five bare peak wires found in the Talent stent graft (Figure 6). This modification allows for same radial force as the Talent system with less stent flare while distributing similar radial force across more points of contact with less force and stress per point of contact.
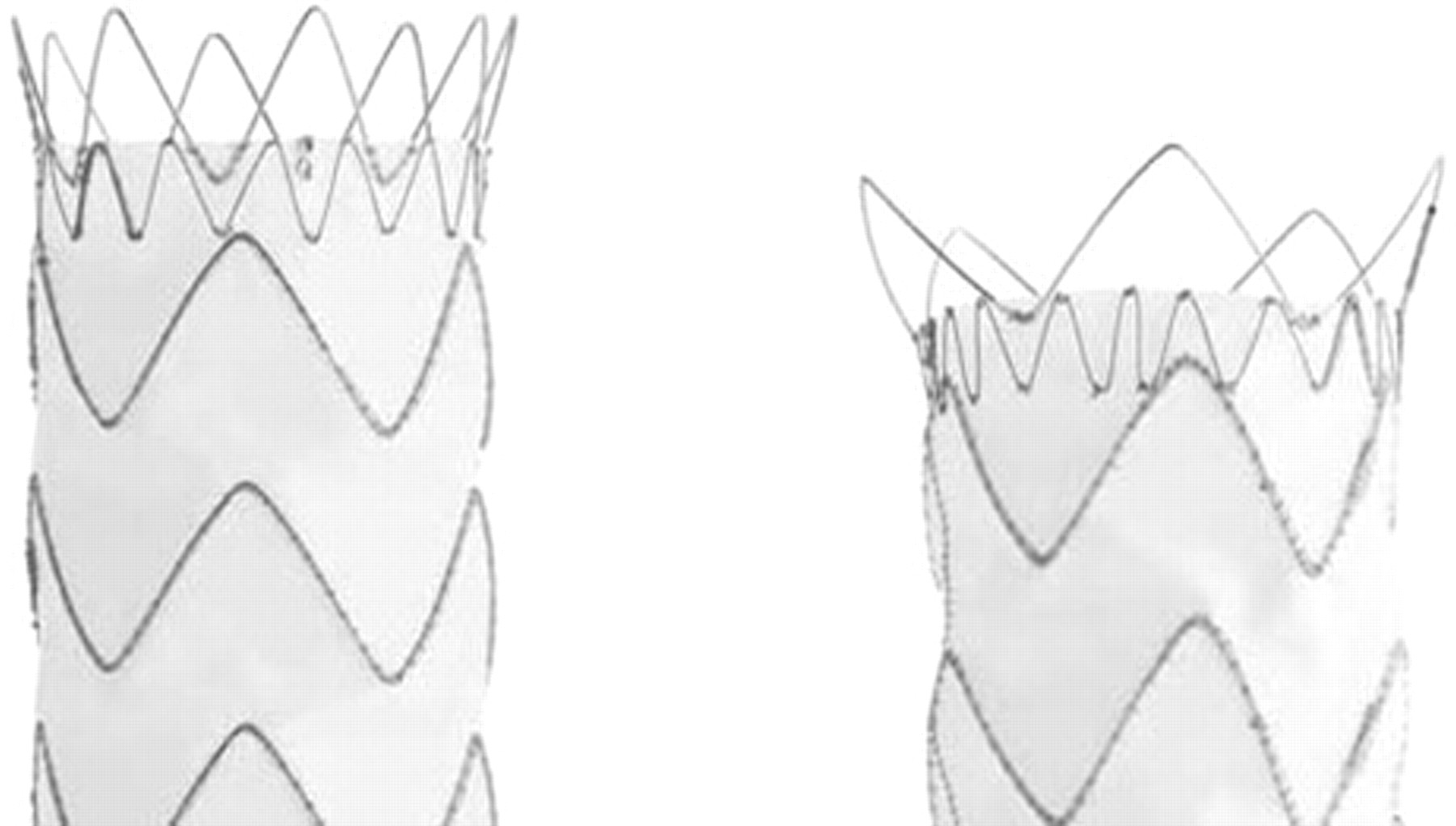
The Valiant stent graft has a modified proximal FreeFlo configuration with eight bare peak wires (left) compared with the five bare peak wires found in the Talent stent graft (right).
The Valiant device is available in lengths ranging from 100 to 227 mm, and its proximal neck diameters range from 24 to 46 mm with a 2 mm increment. Longer thoracic stent grafts are desirable in selected situations when treating thoracic aortic pathologies. The great majority of thoracic aortic conditions require stent graft coverage of up to 200 mm in length. Although shorter thoracic endografts are adequate when excluding focal disease processes such as aortic transection, penetrating ulcers, or saccular aneurysms, longer thoracic coverage is typically necessary when treating atherosclerotic fusiform aortic aneurysm. Longer endografts may result in less modular junctional endoleaks. In addition, fewer passes of large delivery systems through diseased iliofemoral arteries may avoid the risk of device-induced arterial rupture and life-threatening hemorrhage. The Valiant distal device contains closed web configuration in both straight and tapered fashion. Similar to the Talent device, a distal bare spring device available in the Valiant component when implantation is near the celiac artery is required. The delivery system in the Valiant device is 2F size smaller compared with the Talent device and allows for controlled ratcheted precise deployment using the refined Xcelerant delivery system (Figure 7).

The Xcelerent delivery system of the Talent thoracic stent graft device allows stable and accurate deployment.
Brief Clinical Results
The Talent Thoracic Retrospective Registry was designed to collect outcome data from patients who underwent endoluminal treatment with the Medtronic Talent Thoracic Stent Graft in seven European referral centers between November 1996 and March 2004. Data collection was focused on clinical and imaging follow-up, with particular reference to mortality and long-term complications. 15 The entire cohort study consisted of 457 patients (113 emergency and 344 elective cases) who underwent thoracic aortic repair with the Talent Thoracic Stent Graft for different aortic pathologies, including 137 degenerative aneurysms (29.9%), 180 dissections (39.4%), 85 post-traumatic aneurysms (18%), and other pathologies, including penetrating ulcer and intramural hematoma. Fifty-six percent of the patients were classified as ASA class III, IV, or V. Technical success was obtained in 97.8%, with failure in 10 patients owing to the inadequate caliber of the femoral or iliac vessels or to difficult device deployment. In-hospital mortality occurred in 23 patients, with a 7.9% mortality rate for acute cases (9 of 113) and 4% for elective cases (14 of 344). Two of the mortalities occurred intraoperatively (0.4%); both were emergency cases of type B aortic dissection. In-hospital complications included stroke in 17 patients and paraparesis or paraplegia in another 8 patients. In their analysis, stroke was associated with occlusion of the left subclavian artery without revascularization and paraplegia or paraparesis with a covered aorta longer than 20 cm. 15 Follow-up had a mean of 24 months with a late mortality rate of 8.5% (36 patients), and in 11 patients, death was related to the aortic disease.
The VALOR trial is a prospective, multicenter, nonrandomized investigation of the safety and efficacy of the Talent Thoracic Stent Graft system when used in patients with thoracic aortic aneurysms and has three arms. 12 The primary test arm consists of patients diagnosed with thoracic aortic aneurysms who are considered candidates for open surgical repair and who are low to moderate risk. Additionally, two observational treatment group registries were conducted concurrently, serving to record descriptive information that may serve as the basis for future clinical investigations. The registry arm (27 patients) included patients diagnosed with dissections, traumatic injury, and pseudoaneurysms, as well as aneurysms without a distinct proximal or distal aneurysm neck of > 20 mm in length. The high-risk arm (150 patients) included patients diagnosed with the same pathologies who were deemed of operative risk and were not fit for open surgery. The VALOR study includes 40 participating institutions in the United States. The great majority of diseases treated throughout all arms of the study consisted of either fusiform or saccular thoracic aneurysms. The results of the high-risk arm were presented at the Society for Vascular Surgery (SVS) meeting in Chicago in 2005. In this arm, aneurysm comprised 82% of the procedural indications among the patients enrolled. Forty percent of the patients enrolled were females. With a relatively high percentage of female patients compared with AAA disease, challenging issues relating to iliofemoral artery access become critically important. The 30-day mortality rate was 8.4%, with an 8% stroke rate and paraplegia or paraparesis in 5.5% of patients. In the VALOR trial, surgically placed conduits were necessary in upwards of 14% of patients, demonstrating the need for delivery systems smaller than 22F to 24 F. The bare spring or FreeFlo proximal design, as well as the availability of stent graft devices with diameters as large as 46 mm, allowed for greater suitability of endovascular treatment options for a broader range of patients in the VALOR trial compared with any other thoracic device trials currently in clinical investigations. 12 Owing to rapid enrolment in the registry and high-risk groups, enrollment was closed quickly, whereas the test group recently completed enrollment of 195 patients and is awaiting accrual of the 1-year follow-up before being presented to the FDA. Various single-institution series of thoracic aortic stent graft repair using the Talent thoracic device have also been reported. 16–20
Zenith TX2 Stent-Graft System
The Zenith TX2 TAA Endovascular stent graft is designed as a two-piece modular endograft system for thoracic aneurysm repair application. Both the proximal and distal endograft components are a tubular stent graft in design. However, an additional uncovered bare stent configuration is incorporated in the lower segment of the distal endograft device (Figure 8). The product line of the Zenith TX2 stent has recently introduced a novel extension of the original endograft design to be used in conjunction with the proximal TX2 component that is specially designed for the treatment of dissections and is composed of stacked bare Z-stents (Figure 9). This is an investigational device and available only under an investigational device exemption (IDE) in the United States.
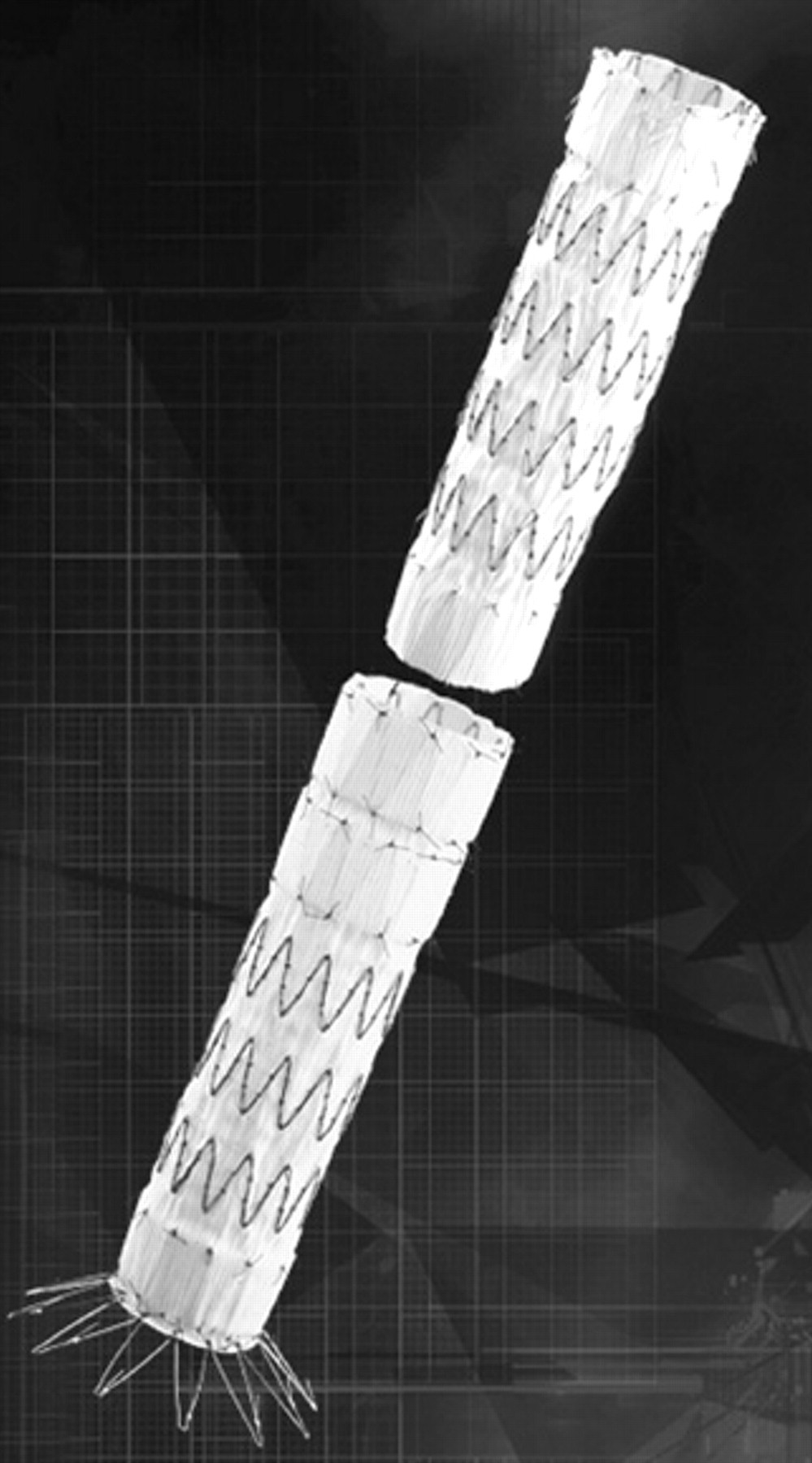
The Zenith TX2 endograft system is designed as a two-piece modular endograft system for thoracic aneurysm treatment.

The Zenith TX2 distal bare stent component is designed for the treatment of aortic dissections, which is used as a distal extension with the main Zenith TX2 component.
Device Description
The Zenith TX2 TAA Endovascular stent graft is designed as a two-piece modular system, although implantation of a single device may be sufficient for focal thoracic aortic lesions (see Figure 8). The Zenith TX2 endograft is constructed of Dacron fabric covered by stainless steel Z-stents. In this device, the proximal end is covered and has stainless steel barbs protruding through the graft fabric (Figure 10), which anchor the graft directly to the aortic wall. This also protects against distal stent graft migration during high-velocity systolic blood flow. The device uses an active fixation mechanism with external barbs oriented in opposing directions and designed to engage the aortic wall to decrease the risk of proximal and distal migration. Full deployment of the proximal stent is released by pulling a trigger wire once the optimal graft position is confirmed. The stents are modified Gianturco Z-stents, with small gaps left between each stent to allow some flexibility. Each end of the graft is held within a cap; inadvertent release during positioning within the aorta is prevented by a safety catch. The full length of the graft material is stent supported to prevent graft torsion or compression. The placement of the stents relative to the fabric is varied along the length of the device. At the ends of the endograft, the stents are sewn inside the fabric, whereas in its midportion, they are outside the fabric. The intent of this design was to optimize fabric apposition to the aortic lumen and fabric-fabric interstent junctions. The Zenith TX2 Proximal Component is available in diameters ranging from 28 to 42 mm and lengths from 12.0 to 21.6 cm. The Z-Trak delivery systems for the Zenith TX2 device have profiles between 20F and 22F. Device deployment is achieved by withdrawing an external sheath.
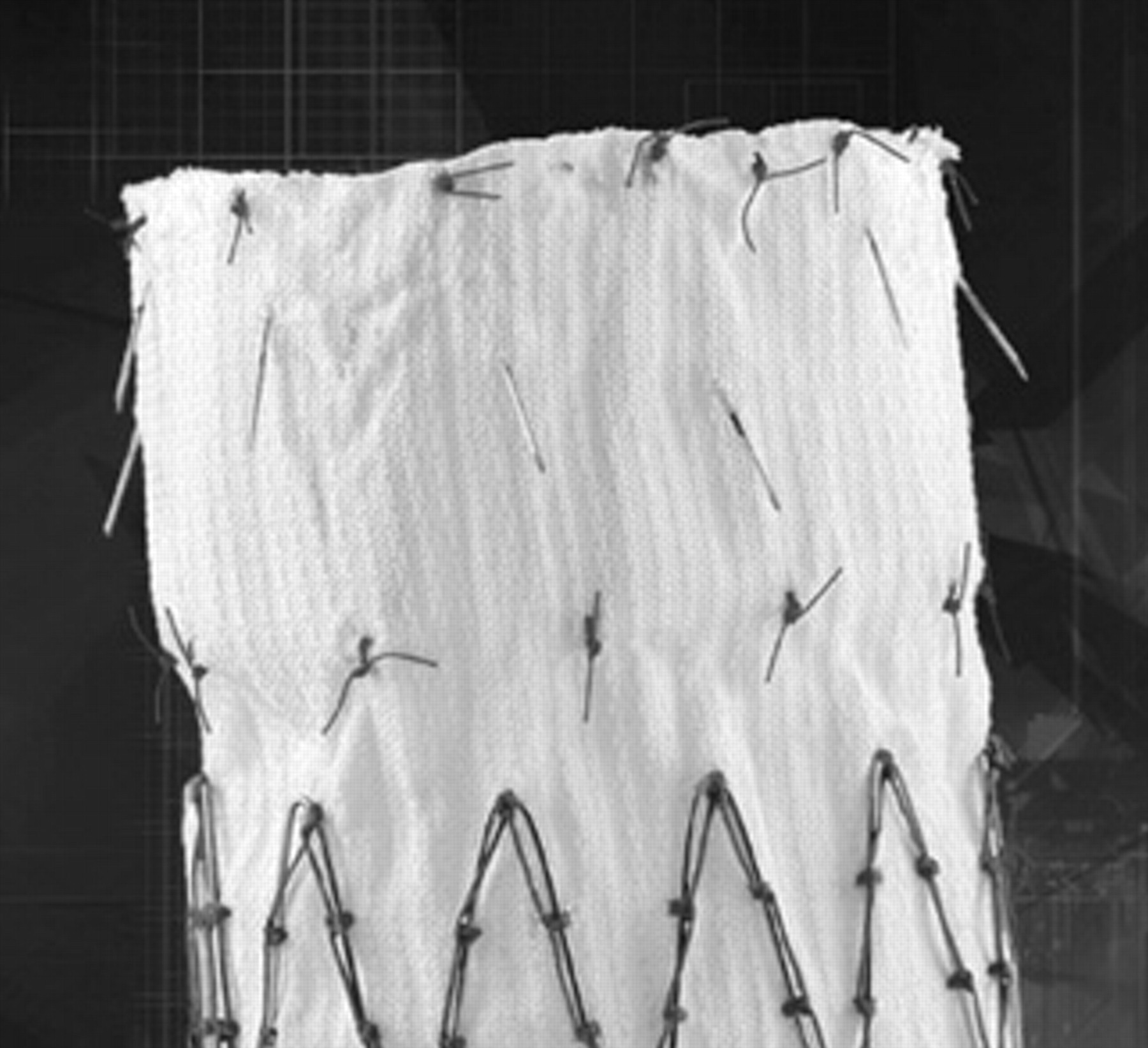
Close-up view of the proximal end of the TX2 proximal component. Note the hooks protruding from the fabric.
The Zenith TX2 Distal Component differs slightly in design configuration compared with the proximal component. The distal end of the device has an uncovered bare metal stent similar to the proximal end of the Zenith Abdominal Aortic Endovascular Graft for AAA. The barbs are on this bare stent and are oriented in a retrograde manner opposite the direction of the proximal hooks (Figure 11). This bare stent configuration allows fixation of the device over the origins of the visceral vessels, where it may be relatively less diseased, and the covered portion to extend right to the origin of the celiac artery. Similar to the proximal component, the TX2 Proximal Component device diameters range from 28 to 42 mm and lengths from 12.7 to 20.7 cm. The deployment method similarly involves first unsheathing the stent graft and, after precisely positioning the distal end, releasing trigger wires to deploy the distal bare metal stents.

Close-up view of the distal end of the TX2 distal component. Note the bare stent with the retrograde-oriented hooks.
The recently introduced Zenith Dissection Endovascular Stent component is designed to be used in conjunction with the Zenith TX2 covered stent in the setting of aortic dissection (see Figure 9). This bare stent component is constructed of stacked Z-stents joined by polypropylene sutures, which can be deployed through a 16F sheath and inserted through the existing Zenith TX2 Proximal Component sheath. A single stent diameter accommodates aortic luminal diameters ranging from 24 to 38 mm and is available in 82, 123, and 164 mm lengths. The Z-stents exert minimal radial force, which allows gradual opposition of the dissection septum and reexpansion of the true lumen. The large open strut architecture allows maintenance of branch vessel perfusion so that the stent can be safely deployed across the origins of the intercostal, visceral, and renal arteries. In the scenario of persistent malperfusion owing to a dissection flap into or a reentry tear near a vessel origin, the bare Z-stent component provides structural scaffolding for placement of a bare or covered peripheral stent from the true lumen into the branch vessel bridging across the false lumen (Figure 12).
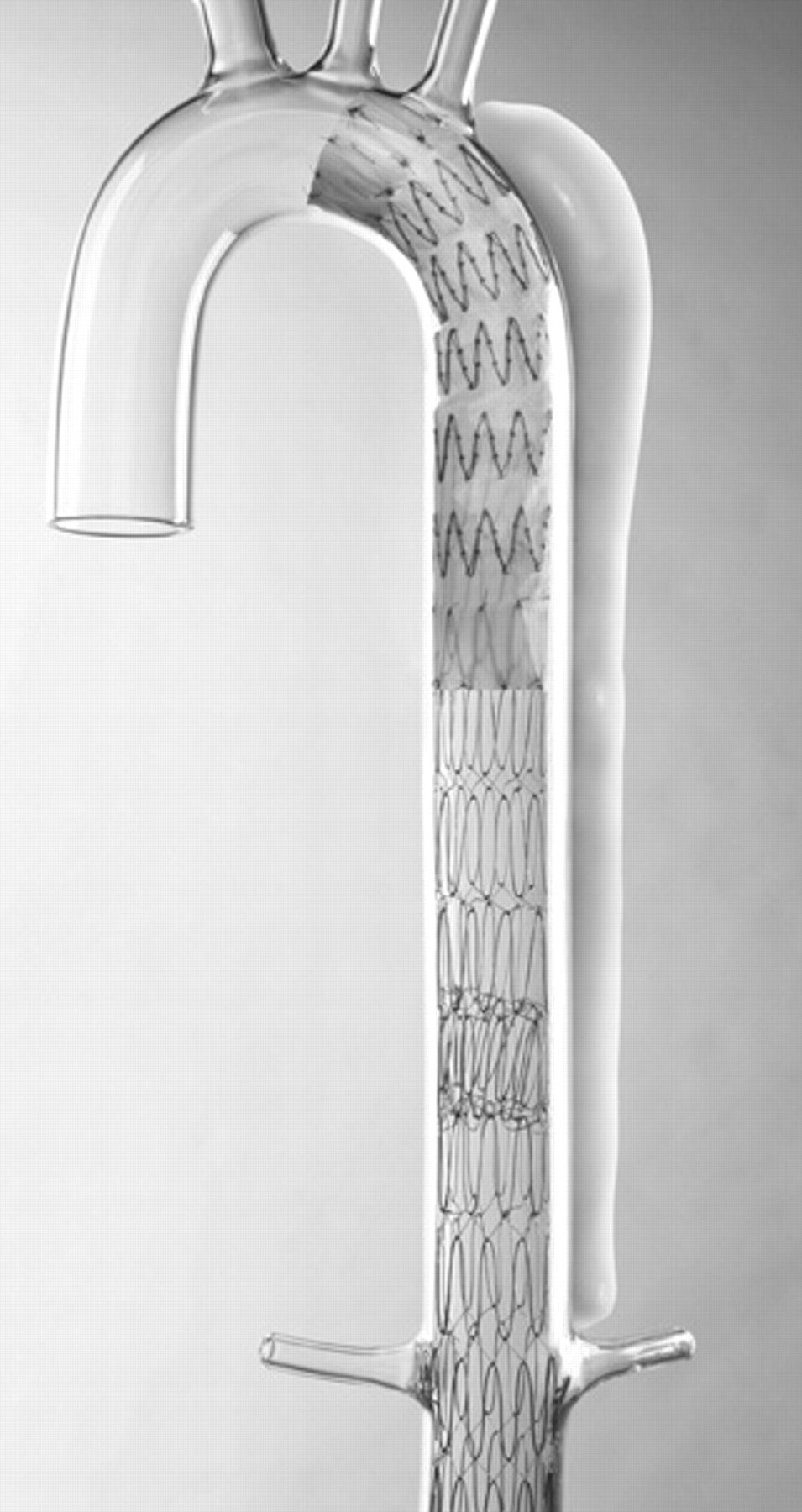
A glass model depicting the treatment strategy using the TX2 proximal component with the distal bare stent component. Note how the bare stent can be deployed over the abdominal visceral vessels in the setting of aortic dissection or malperfusion syndrome.
Brief Clinical Results
The Zenith TX2 stent graft is an investigational endovascular device designed to treat aneurysms and other degenerative pathologies of the thoracic aorta. At the time of this writing, it is nearing completion of its pivotal trial. Clinical experience with this device is limited to outside the United States and to sites participating in the clinical trials. 21 In 2005, Greenberg and colleagues reported the midterm results of their first 100 consecutive thoracic aortic repairs using the Zenith TX1 (first generation) and TX2 stent graft systems. 22 This study was performed under a sponsored IDE between February 2001 and April 2004. The authors noted that the majority of the experience comprised aneurysms (81%) and chronic dissections with aneurysm degeneration (15%). The follow-up of the patients lasted for 24 months. At 1 year, the overall mortality rate was 17%, with an aneurysm-related mortality rate of 14%. At 2 years, the all-cause mortality rate was 23%, of which the majority were also aneurysm related (20%). It is to be emphasized that many of these patients were clearly high risk or compassionate use equivalent. 23 Spinal cord ischemia occurred in 6% and strokes in 3% of patients. Other pertinent outcomes at 1 year included a 6% rate of endoleak, 15% secondary interventions, and 6% migrations. The authors noted that 55% of these enrolled patients had a previous aortic aneurysm repair and 19% required iliac conduits. Another single-center experience from Italy using the Zenith TX1 version of the device for the treatment of a variety of thoracic pathologies in 45 consecutive patients has also been published. 24 The technical success of stent deployment was 98%, with no in-hospital mortality or stroke. There was one case of transient paraplegia. At a mean follow-up of 7.3 months, there were no aneurysm-related deaths, no graft migrations, or structural failure related to the graft. Taken together, these two single-center experiences provide preliminary indications of the potential safety and effectiveness of this modular aortic endograft for the treatment of thoracic aortic aneurysms.
The Zenith TX2 pivotal trial has recently completed the enrollment of the test or endovascular arm. 25 This is a prospective, nonrandomized, multinational, investigational device exemption clinical trial involving 35 centers with the aim of studying the safety and efficacy of the TX2 stent graft system in the treatment of thoracic aortic aneurysms. Patient allocation to the endovascular treatment group or the surgical control group is based on the anatomy of their aneurysm. Anatomic inclusion criteria into the endovascular arm included descending thoracic aortic aneurysms and penetrating ulcers with at least 3 cm of healthy, uninvolved aorta proximal and distal to the lesion. No patients may be enrolled in either arm of the study if any of the general exclusion or medical exclusion criteria are true. Patients may not be enrolled in the endovascular treatment arm if any of the endovascular anatomic exclusion criteria are true, and patients may not be enrolled as surgical controls if any of the surgical anatomic exclusion criteria are true. The study design involves 135 endovascular repairs and 70 contemporary (repairs performed within 12 months of enrollment) and prospective open surgical controls. The primary safety end point was 30-day all-cause mortality compared with the surgical controls, and the primary efficacy end point was 30-day rupture-free survival. Secondary end points include procedural and treatment successes, adverse events, mortality, clinical utility measures (eg, mean ICU time, mean length of hospital stay, mean return to daily activity), and quality of life assessment at 12 months. The study started enrolling patients in March 2004 and is nearing its enrollment targets. 23 No results are yet available from this study.
Relay Thoracic Stent-Graft System
Device Description
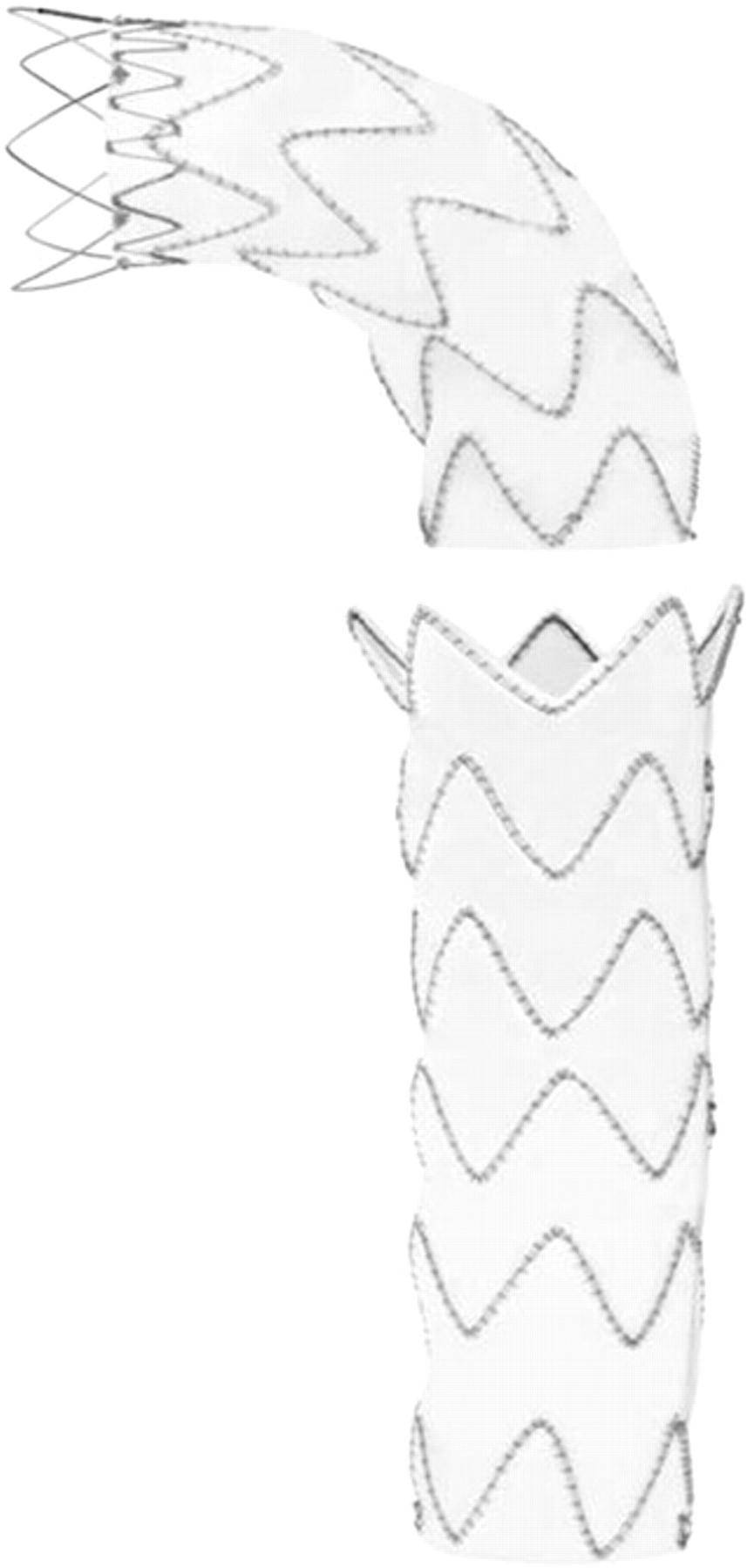
The Relay Thoracic Stent-Graft is a new endovascular device for the treatment of thoracic aortic pathologies (Figure 13). Clinical investigation is currently under way to assess its efficacy in the treatment of descending thoracic aneurysms. This device is composed of self-expanding nitinol stents that are sutured to a polyester fabric graft. The skeleton of the device is made up of a series of sinusoidal stents placed along the length of the graft fabric. To provide longitudinal support for this device, a curved nitinol wire is attached to the outer curve of the endograft fabric by a series of sutures. This design provides moderate column strength while maintaining desirable flexibility and torque response. A series of radiopaque markers, composed of platinum and iridium, are attached to the endograft in various locations to enhance fluoroscopic visualization. The Relay device is available in various sizes and configurations, both tapered and nontapered. Graft lengths up to 200 mm are available, with diameters from 22 to 46 mm. The profile of the primary introducer sheath ranges from 22F to 26F in size depending on graft diameter and length.

The Bolton Relay Thoracic Stent-Graft system.
Brief Clinical Results
The feasibility or phase I study for the Relay Thoracic Stent-Graft in the treatment of descending thoracic aortic aneurysms and penetrating ulcers was approved by the FDA in December 2004. This study was initially limited to 30 patients and 5 clinical sites. Regulatory approval to include two additional sites was granted in April 2005. Available information showed that more than 20 patients have been enrolled in the phase I study as of November 2005. Eighteen (90%) had thoracic aortic aneurysms and two (10%) had penetrating ulcers. Delivery and deployment of the device were deemed satisfactory in all instances except in three cases (15%), all involving a tendency toward distal device migration. This phenomenon occurred when the deployment sequence involved a “stop-and-go” maneuver with initial expansion of the first two to three stent segments before proceeding to full uncovering and expansion along its full length. These observations were similarly reproduced on bench testing, which led to a modification of the IFU involving the deployment technique. Since a modified deployment technique was instituted, no further occurrences relating to device migration were noted during the deployment process. Among all procedures that could be completed, there was a 100% technical success rate, with delivery and deployment of the device as intended and complete angiographic exclusion of the target lesion. There have been no 30-day mortalities. Two endoleaks have been reported on 6-month follow-up scans, although the precise cause remains undetermined. There have been no unanticipated device-related adverse events to date. Completion of the phase I study was achieved in 2006. It is anticipated that the results of this trial will be published at a later date.
Conclusion
Endovascular treatment of descending thoracic aortic diseases is an exciting treatment modality that can potentially be used in a variety of thoracic aortic pathologies. This minimally invasive treatment strategy may provide the greatest benefit in high-risk patients who are unfit for open surgery. It is anticipated that endovascular thoracic technology would provide a greater impact in treatment benefit than endovascular AAA repair because of the higher morbidity of the open thoracic aortic procedures. The perceived benefits of endovascular repair have generated enormous interest for device manufacturers to create an ideal device in the treatment of descending thoracic aortic diseases. Experience with endovascular treatment in a wide spectrum of thoracic aortic diseases demonstrates the feasibility of this approach even in unstable patients as early and midterm results have been promising. 2,4,26 A longer follow-up study will undoubtedly be necessary to validate the durability of this technology.