
Abstract
Mycotic aneurysms of the extracranial carotid artery are uncommon and always warrant surgical treatment to prevent eventual rupture and death. Septic embolization to the brain is an even rarer complication of these aneurysms. We present a case of a 79-year-old male with an extracranial internal carotid artery mycotic aneurysm during Staphylococcus aureus bacteremia. He presented with hemiparesis owing to brain embolism from multiple septic emboli originating from the aneurysm. Multidetector computed tomographic angiography contributed to the diagnosis. Resection of the aneurysm and restoration of arterial supply to the brain by vein graft interpositioning was the therapeutic procedure along with long-term antibiotic treatment. A high index of suspicion is required for the diagnosis of a mycotic carotid aneurysm and aggressive treatment is always needed to prevent lethal complications.
Mycotic aneurysms of the extracranial carotid artery are relatively rare entities associated with increased mortality. 1 Their initial clinical manifestations are subtle and sometimes nonspecific; therefore, they can be difficult to diagnose in the early stages, especially if the aneurysm is small. 2 We present a patient with an infected pseudoaneurysm of the extracranial right internal carotid artery (ICA) owing to Staphylococcus infection who presented with a neurologic deficit owing to multiple cerebral septic emboli and was diagnosed by multidetector computed tomographic angiography (MDCTA). We discuss aspects of pathogenesis, diagnosis, and treatment, as well as the role of MDCTA in the management of ICA mycotic aneurysms.
Case Report
A 79-year-old man was admitted to our hospital owing to a transient hemiparesis of his left arm, 4 days prior to admission. A plain brain computed tomographic (CT) scan at that time was reported as normal. He complained of a fever of 102°F (39°C) during the last couple of days.
From his recent history, he had suffered from a herpes zoster infection 2 months previously. During the last 20 days, he had felt the presence of a right-sided tender mass, which was attributed to lymphadenitis. Fifteen years ago, he had undergone left nephrectomy owing to cancer.
On admission, his body temperature was 101°F (38.5°C). Tenderness at the site of the right carotid bifurcation was confirmed during palpation. Laboratory testing revealed a white blood cell count of 10,900/mm 3 with 90% neutrophils, a hemoglobin of 9.5 mg/L, an elevated erythrocyte sedimentation rate of 110 mm/h, and a C-reactive protein level of 4.5 mg/dL. A new brain CT scan revealed multiple high-attenuation areas, most likely hemorrhagic, within the right parietal lobe. Further investigation with magnetic resonance imaging (MRI) of the brain depicted four areas of abnormal signal intensity on the right hemisphere (parietal lobe and posterior frontal lobe) (Figure 1). The lesions' characteristics and alterations over time compared with the first CT scan suggested the presence of multiple hemorrhagic septic emboli.
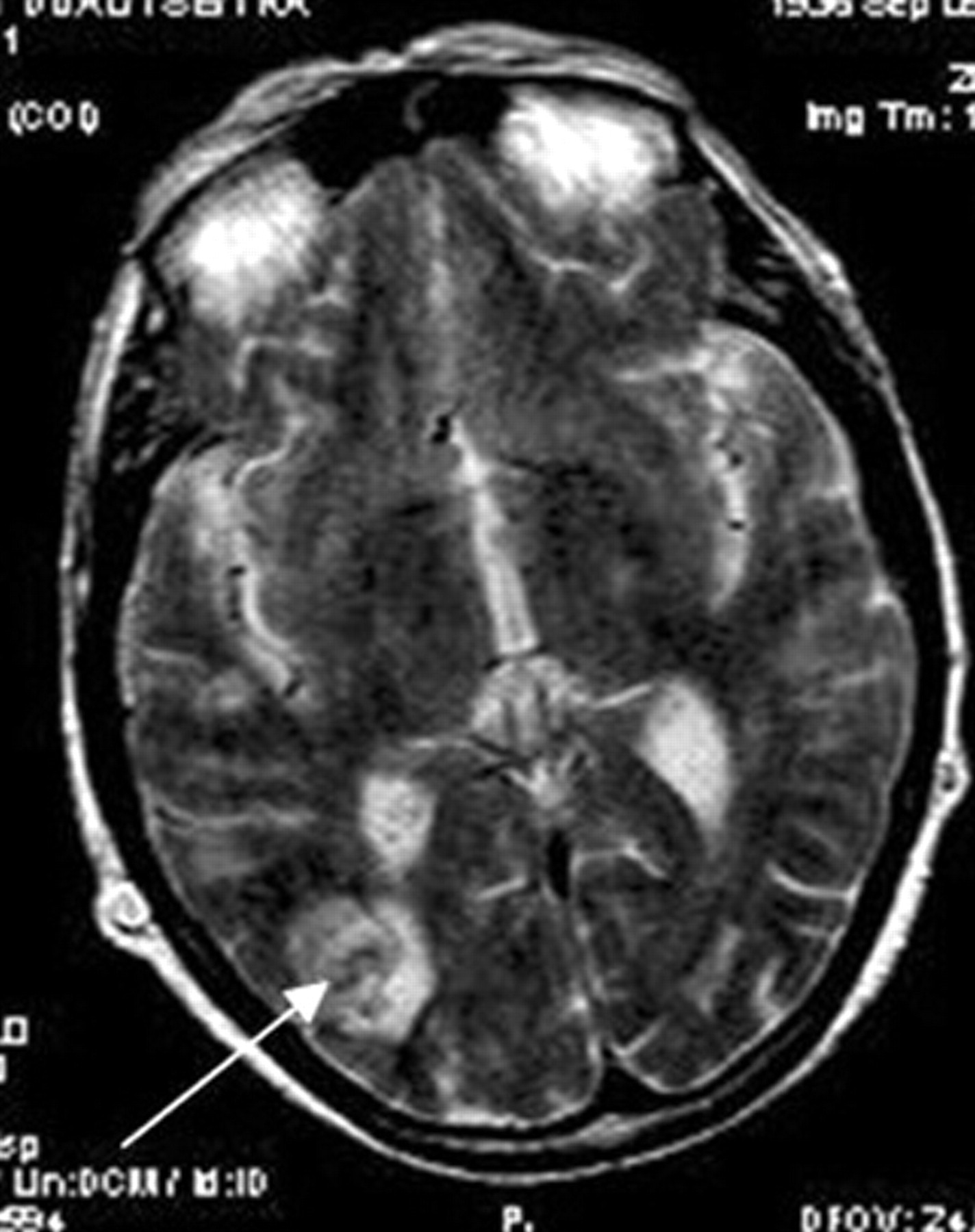
Brain T2-weighted magnetic resonance image: the white arrow indicates the mixed signal of the parietal lobe lesion.
The following day, a color Doppler ultrasound examination revealed thickening of the right carotid bifurcation, suggesting arteritis. A contrast-enhanced CT scan of the neck showed a soft tissue density mass surrounding the right carotid lumen mainly at the bifurcation, with no clear aneurysmal dilatation. A low-attenuation component was present within the mass, whereas the jugular vein was severely compressed (Figure 2). Blood cultures obtained at the time of admission yielded methicillin-resistant Staphylococcus aureus (MRSA). Administration of intravenous antibiotics consisting of imipenem and vancomycin was started immediately to fight a suspected microbial arteritis.

Contrast-enhanced computed tomographic scan of the neck showed a soft tissue density mass surrounding the right carotid bifurcation (black arrow). A low-attenuation component was also present within the mass (black arrowhead). The jugular vein (white arrowhead) was severely compressed.
Two days later, a 3 cm–long pulsatile mass, without overlying erythema, was palpated at the level of the right carotid bifurcation. MDCTA was performed (GE Lightspeed 500, General Electric Medical System, Milwaukee, WI) in order to follow up the abnormal tissue in the neck but also to evaluate the entire carotid lumen, including the intracranial segment and the aortic arch region. MDCTA revealed thickening of the wall of the right carotid artery, starting from the level of the mid–common carotid artery and up to the level of the mid-ICA (C2 level) (Figure 3A). At the carotid bifurcation, a soft tissue mass arising mainly from the lateral wall surrounded the lumen. Other, more hypodense areas were observed within the mass, and an aneurysmal dilatation (maximum diameter 14 mm) of the lateral aspect of the vessel lumen was now detected at the same level (Figure 3, B and C). The appearance suggested a rapidly growing pseudoaneurysm of the ICA. Consequently, urgent exploration under general anesthesia was decided.

A, A computed tomographic angiogram (CTA) (coronal multi-planar reconstruction) shows thickening of the wall of the right carotid artery from the level of the mid–common carotid artery up to the level of the mid–internal carotid artery (C2 level) (white curved line). B, CTA revealed aneurysmal dilatation of the lateral aspect of the carotid artery at the level of carotid bifurcation (black arrow), surrounded by a mass suggesting an infected pseudoaneurysm of the carotid artery. The more hypodense area seen within the mass depicts pus evacuated during surgery. C, Three-dimensional CTA (volume rendering technique algorithm) depicts the pseudoaneurysm of the right carotid bifurcation (white arrow).
After harvesting a 10 cm-long right great saphenous vein conduit from the groin, the common carotid artery was controlled low in the neck, via the standard approach for carotid endarterectomy. Infectious tissue was closely adherent to the carotid bifurcation, creating a dense mass that was impossible to dissect (Figure 4A). The ICA was dissected and looped at the level of the digastric muscle and the external carotid artery at the level of the lingual branch. The hypoglossal nerve was identified and preserved. After systemic anticoagulation and clamping, the mass was opened and pus was discharged. The culture of the pus was positive for MRSA. Afterward, a longitudinal arteriotomy was performed and a 5 mm–long defect was identified at the lateral aspect of the carotid bifurcation. The carotid bifurcation was excised, and most of the infected soft tissue was débrided. The surgical field was irrigated with povidone-iodine and antibiotic solution. The external carotid artery was ligated, and a 6 cm–long saphenous vein graft was interposed between the common carotid artery and the ICA (Figure 4B). No shunt or method of intraoperative brain monitoring was used. The total clamping time was 40 minutes. A closed suction drain was used, which was removed 24 hours later. Postoperatively, the patient was given antibiotics consisting of imipenem and vancomycin intravenously for 7 days, based on the sensitivity studies, and then ciprofloxacin and clindamycin orally for an additional 10 days. He had an uneventful recovery and was discharged on the seventh postoperative day. Histologic examination of the pseudoaneurysm revealed severe chronic inflammation (Figure 5). A month later, on a follow-up MRI, a brain abscess was shown, and the patient restarted the previous antibiotic scheme (ciprofloxacin and clindamycin). This led to an almost complete resolution of the abscess after a 3-month period of antibiotic therapy.
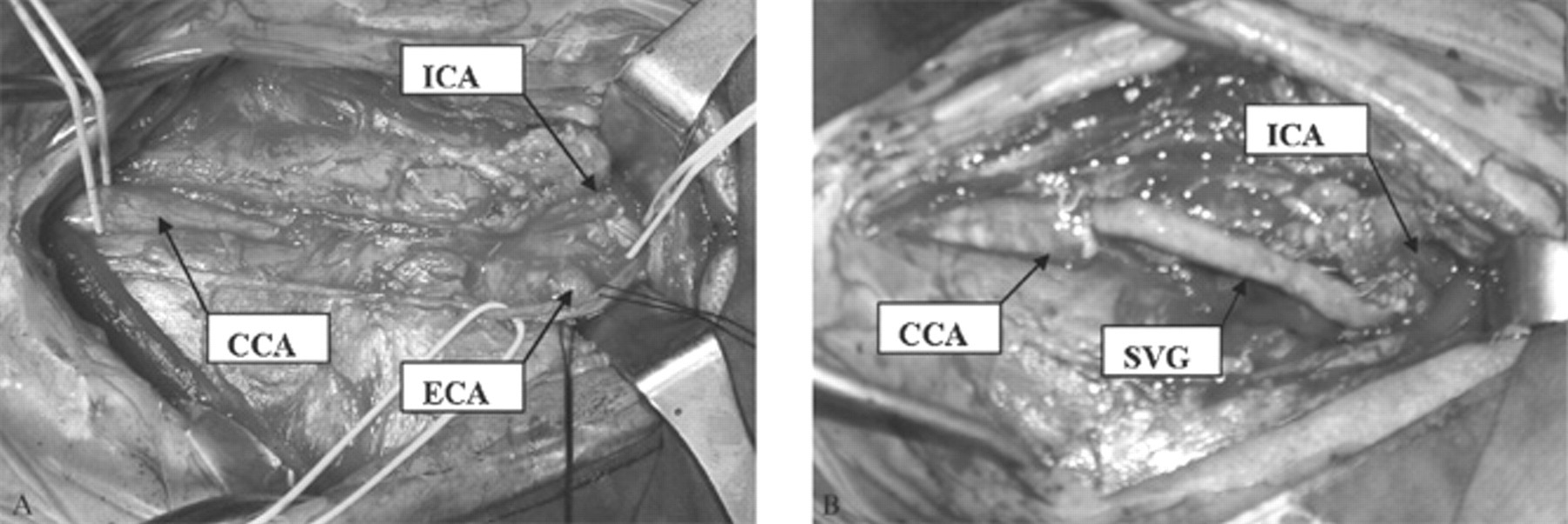
A, Infectious tissue was closely adherent to the carotid bifurcation, creating a dense mass. B, The external carotid artery (ECA) was ligated and a saphenous vein graft (SVG) was interposed between the common carotid artery (CCA) and the internal carotid artery (ICA).

Photomicrograph (hematoxylin-eosin stain; ×100 original magnification) shows severe fibrosis and hyalinization of the intima (arrow) with fibrin deposition, as well as disperse, subtle, chronic inflammatory infiltrates (arrowhead).
Discussion
Mycotic extracranial carotid aneurysms are exceptionally rare, with 74 cases being reported in a 2002 review by Knouse and colleagues. 1 We uncovered at least 13 additional cases reported in the English literature to date using the PubMed database. 2–14 These aneurysms usually occur in the setting of systemic sepsis and seeding of the vascular system from a distant infectious source (eg, endocarditis). Other common mechanisms include direct spread throughout the course of head and neck infections and carotid surgery and trauma. Before the introduction of antibiotics, syphilis, tuberculosis, and untreated endocarditis were the most common causes. 15 Nowdays, intravenous drug abuse, dental extractions, and angiographic procedures supplement the modern list of predisposing conditions. Mycotic aneurysms occur with increased frequency in patients with immunodeficiency. 16 Mycotic extracranial carotid aneurysms usually present as a growing, pulsatile cervical mass associated with pain, tenderness, fever, dysphonia, or dysphagia.
S. aureus has been reported as the most common culprit. 1 The pathologic process most likely responsible for the pseudoaneurysm formation in our case was transient bacteremia originating from skin scratching. S. aureus inoculated the atheromatous plaque of the carotid bifurcation, leading to inflammation and perforation.
Prompt diagnosis and treatment are of paramount importance because if mycotic aneurysms are left untreated, they carry high percentages of morbidity and mortality owing to lethal complications such as rapid enlargement with rupture, hemorrhage, and septic embolization with neurologic sequelae and arterial occlusion. 2 Our case highlights the fact that clinical deterioration and alterations in radiologic features can happen in a short period of time. During the first 4 days after the initial onset of neurologic symptoms, the patient developed multiple cerebral septic emboli, whereas the pseudoaneurysm was formed within 48 hours from the diagnosis of the inflamed vascular wall on the initial CT scan of the neck. The aforementioned fact is of extreme importance as early recognition of the disease and knowledge of its dynamics highly contribute to preventing lethal complications.
With recent advances in technology, efficient diagnosis of the disease is easy and accurate. Color Doppler ultrasonography is usually the first imaging modality for the differential diagnosis of a neck mass, which includes a carotid body tumor, carotid artery kinking and redundancy, cervical lymphadenitis, and deep neck abscesses. 17 It has some limitations to characterize an aneurysm as a mycotic one since it cannot evaluate the perianeurysmal space in detail. 18 Contrast-enhanced CT is the method of choice for that purpose since it offers great advantages, evaluating not only the arterial lumen but also the perivascular space in search of gas, hematoma, fluid, or calcifications. Additionally, it depicts the mural thrombus, the rim enhancement of abscesses, and the possible involvement of other structures (eg, veins). 19 In our case, it offered invaluable information and guided the diagnosis. Digital angiography has largely been used preoperatively to guide surgical planning, offering adequate mapping and evaluation of the entire arterial tree. 20
Ever since the introduction of multidetector scanners, computed-tomography angiography (CTA) is increasingly used for imaging of the carotid arteries and intracranial vessels, tending in many cases to replace conventional angiography. 21,22 In addition to the previously described advantages of a standard CT scan, MDCTA has further benefits over conventional angiography. This method evaluates not only the entire carotid arterial lumen, from the aortic arch up to the intracranial segment, but also the surrounding tissues and their relationship with the arterial lumen. Additionally, MDCTA offers a lack of invasiveness, especially in inflamed vessel walls, rapid examination and interpretation time, and capability for reconstruction in any axis, even three-dimensional. Visualization of the integrity of the circle of Willis, as well as detection of any possible anatomic variations that would be useful for surgical planning, can be easily achieved.
Classic surgical management of infected aneurysms includes excision of the aneurysm, débridement of all infected tissue, and restoration of the arterial continuity. Synthetic grafts should best be avoided for fear of graft infection. Potential alternatives include vein graft interpositioning, venous patch angioplasty, primary suturing, primary end-to-end anastomosis, and use of the transected external carotid artery for inflow. 10,23 Ligation of the ICA was a procedure of choice in the past, carrying an incidence of major stroke of 30 to 50% and a mortality rate of 17 to 40%. 23,24 However, it should now be reserved only for aneurysms extending high in the base of the skull and in gross purulence of the operative field. 18 Ligation is reported to be well tolerated when the ICA stump pressure is up to 70 mm Hg, conveying adequate collateral circulation. 25 Stump pressure measurement can also be accomplished preoperatively during angiography using a special transducer catheter distal to an occlusion balloon. In this setting, any gross inadequacy of the collateral circulation may be uncovered, producing an obvious neurologic impairment. 18,23 With proper patient selection, the incidence of stroke after ligation may be reduced to 10%. These patients, despite adequate stump hemodynamics, experience a stroke attributed to thrombus development into the intracranial carotid artery that either progresses into the middle cerebral artery or embolizes its tail into the latter. Therefore, many suggest postligation anticoagulation for 6 weeks. 23 The use of an intraoperative shunt is normally recommended in cases of low stump pressures (< 25 mm Hg). 26 Nonoperative treatment in the past led to the death of 70 to 90% of patients. Operative management, in contrast, carries a mortality rate of 20%, which has decreased to 10% since 1975, when interposition venous grafting was introduced. 1 Postoperatively, antibiotic therapy is generally recommended for at least 6 weeks. 27,28
Endovascular repair with covered stents is very attractive as it limits the risks for operative damage to the surrounding structures and the potential for substantial blood loss. They are generally not recommended because the addition of a prosthetic material in an infected field may incite disastrous sequelae. However, the use of a covered stent, in combination with long-term antibiotic therapy, for exclusion of an infected postendarterectomy pseudoaneurysm has been reported in the literature, with satisfactory 1-year results. 29 Endovascular technology has also been used to substitute surgical ICA ligation. This has been achieved by deployment of coils in the adjacent distal and proximal ICA, leading to thrombosis of the pseudoaneurysm. 3–5,30,31 However, coils represent a potential cause of persistent infection. 30,32 The exact role of endovascular repair in the management of mycotic carotid aneurysms is yet to be determined. 29
In our case, we unexpectedly palpated pulses in the ICA stump, although they were extremely weak. This was, of course, a convincing rationale for carotid ligation. In contrast, we decided to restore the circulation for fear of a possible late neurologic event. Prior to carotid clamping, we raised the patient's systemic blood pressure (about 160 mm Hg), aiming to augment blood flow through collaterals. This may have been responsible for the weak palpable pulses, which may later be compromised, considering the fact that the patient used to be normotensive (100–120 mm Hg). Late neurologic events of up to 6 weeks following carotid ligation have been reported in the literature. 7,23 Indubitably, the presence of adequate collaterals made the shunt use unnecessary; moreover, it is not the standard practice in carotid endarterectomy at our institution.
In conclusion, we underline the high index of suspicion required for the early diagnosis of an infected carotid aneurysm to stop the rapid progression of the disease. MDCTA highly contributes not only to the diagnosis but also to the planning of the surgical management. Interposition of the long saphenous vein is the procedure of choice, with ligation and endovascular repair being used in certain cases. Long-term antibiotic therapy is always needed.