
Abstract
We report a case of successful transcatheter arterial embolization of a pancreaticoduodenal artery pseudoaneurysm (PSA) caused by erosion of the pancreatic pseudocyst content near pancreaticoduodenal arteries. A 55-year-old man was admitted to a local hospital for investigation of severe, stabbing epigastric pain confined to the upper abdomen. He had a history of previous alcohol abuse, chronic pancreatitis, and a duodenal ulcer. Upper gastrointestinal endoscopy revealed narrowing in the pyloric channel along with an ulcer located at the first and second portions of the duodenum with oozing beneath an adherent cloth and duodenal distortion. Computed tomography additionally revealed an enlarged head of the pancreas with numerous spot calcifications and round cystic formation inside, with a diameter of 30 × 25 mm. Following two surgical procedures for duodenal ulcers, selective angiography revealed a PSA located inside the pancreas head and high-grade stenosis > 90% of the celiac trunk and hepatic artery that rose separately from the aorta. Fiber coil embolization was used to occlude the PSA sac successfully. There was no complication after completion of the last embolic procedure. The patient was doing well after 26 months.
Pancreaticoduodenal artery (PDA) pseudoaneurysm (PSA) is a relatively uncommon, potentially lethal vascular structure that may cause life-threatening gastrointestinal bleeding. 1–4 PSA formation could be a disastrous complication of pancreatitis, with an incidence estimated to be as high as 10%. 4 The expected outcome is rupture, with an associated mortality rate between 15 and 50%. 5 We report a case of symptomatic PDA PSA associated with hepatic and celiac trunk origin stenosis that was successfully managed.
Case Report
A 55-year-old man was admitted to a local hospital for investigation of severe, stabbing, epigastric pain confined to the upper abdomen, accompanied by fever and hypotension. The patient complained of vomiting, hematemesis, and melena a week before. He had a history of alcohol abuse, chronic pancreatitis, duodenal ulcer, and significant weight loss.
Six months previously, upper gastrointestinal endoscopy revealed narrowing in the pyloric channel along with an ulcer located at the first portion of the duodenum with oozing beneath an adherent cloth and distortion of the duodenal bulb. The patient underwent emergency surgery; closure of the duodenal perforation and omental patching were done. At discharge 8 days later, the patient was doing well.
Repeated gastroduodenal endoscopy detected new active oozing at the same place. Computed tomography (CT) revealed an enlarged pancreatic head with numerous spot calcifications and round cystic formation inside (30 × 25 mm). The radiologist was not explicit enough in specifying the nature of a cystic formation; otherwise, the PSA would be occluded by an interventional approach, avoiding a new surgical procedure.
The patient's condition was getting worse; therefore, a new surgical procedure was performed the next day (cholecystectomy, Billroth II gastrojejunostomy) for staunching hematemesis and melena. During surgery, pulsatile tumefaction, probably a PSA, located deep within the parenchyma of the pancreas was identified. Considering the difficulties in a surgical approach to the PSA and the lack of experience in vascular surgery, the procedure was completed and the patient was transferred to our vascular unit for further treatment.
Selective angiography revealed that the celiac trunk, hepatic artery, and splenic artery rose separately from the abdominal aorta with stenotic arterial roots, > 90% (Figure 1). Superselective angiography through the superior mesenteric artery showed a PSA inside the pancreatic pseudocyst derived from the inferior posterior PDA (Figure 2). Owing to previous surgery and the patient's condition, catheter-based embolization was chosen for further treatment. The first attempt at aneurysm sac embolization was performed through the superior mesenteric artery with three fiber coils (Figure 3). The PSA sac disappeared after embolization, and we did not notice any PSA feeding collateral branches. Additional surveillance for collateral branches always needs to be performed.

The celiac trunk and common hepatic artery rose separately from the abdominal aorta. A, Stenotic hepatic arterial root > 90%; B, stenotic hepatic and splenic arterial roots; gastroduodenal orifice (dashed arrow); C and D, stenotic splenic arterial root.
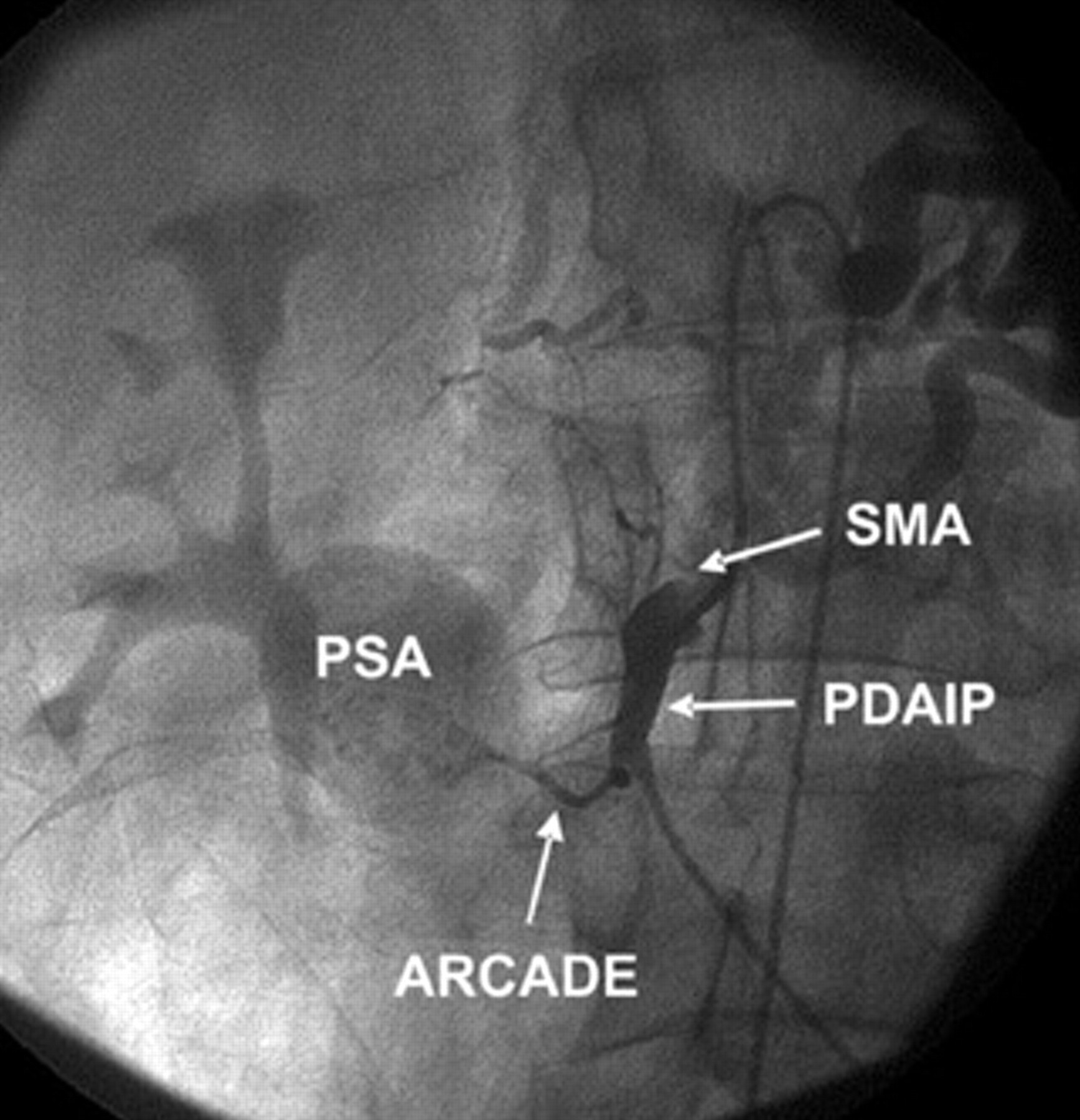
Pancreaticoduodenal inferior posterior artery (PDAIP) selective angiography. Pseudoaneurysm (PSA) at the level of the pancreaticoduodenal inferior posterior and the pancreaticoduodenal superior anterior artery anastomosis (arcade). SMA = superior mesenteric artery.
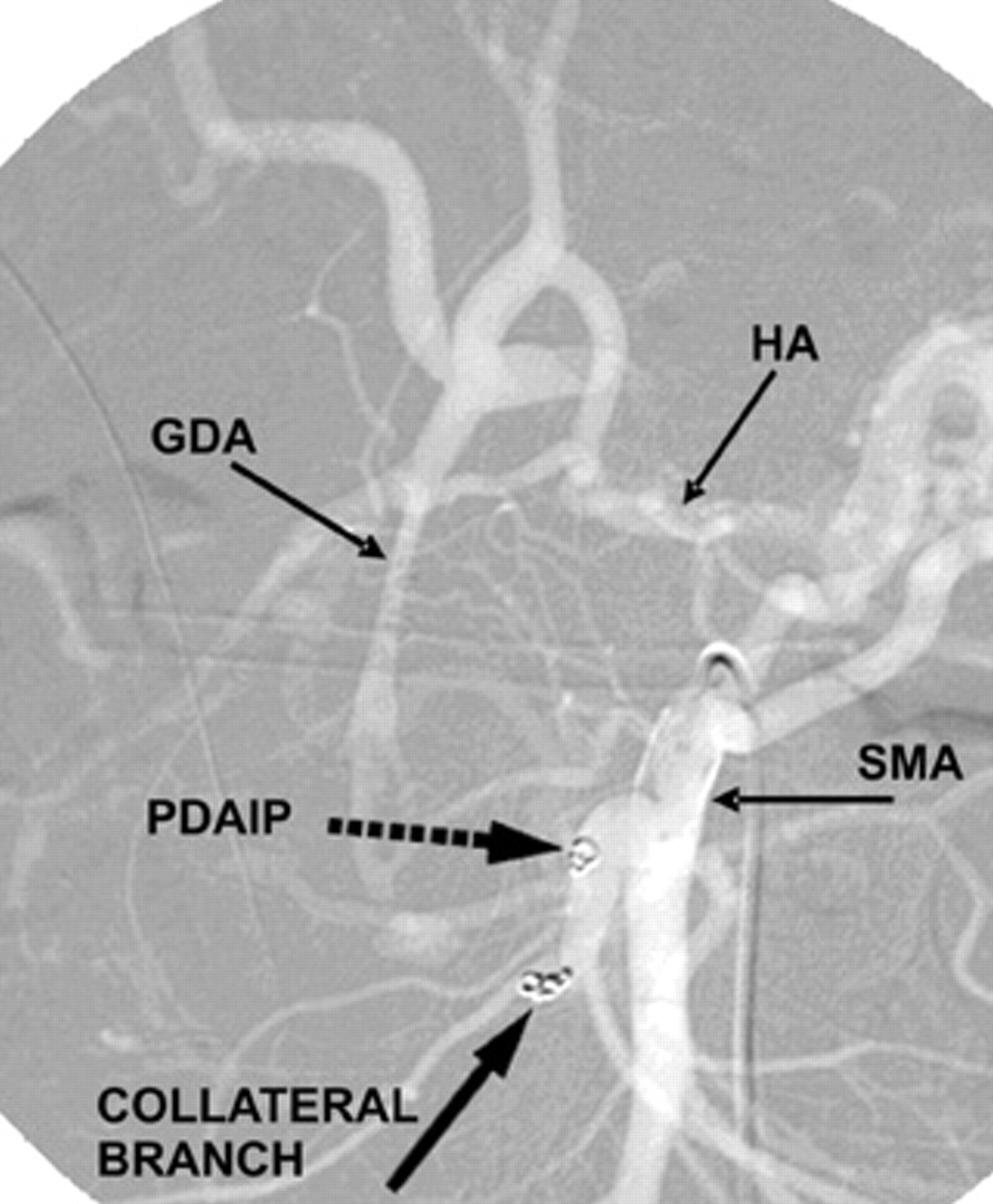
First embolization, performed through the superior mesenteric artery (SMA): three fiber coils embedded into the initial part of the pancreaticoduodenal inferior posterior artery (PDAIP) (discontinuous arrow) and one in the collateral arterial branch. The pseudoaneurysm sac was no longer visible. GDA = gastroduodenal artery; HA = hepatic artery.
Two days later, the patient had melena again. Repeated angiography showed incomplete PSA sac occlusion; therefore another embolization was performed throughout the hepatic and gastroduodenal arteries. During the procedure, hepatic and celiac trunk artery orifice subocclusion was detected. Hepatic artery stenosis was relieved by balloon dilatation and stenting, and the upper aneurysm sac entrance was closed deploying another two fiber coils. This second-time embolization was due to a failure of the first coils to occlude all feeding PSA branches. Control angiography confirmed aneurysm occlusion (Figure 4).

A and B, High-grade hepatic artery (HA) stenosis relieved by balloon dilatation and placing two stents, the Selfx (8.0 × 32 mm) and the WaveMax (Abbott Laboratory, Abbott Park, IL 7.0 × 28 mm). C and D, The upper aneurysm sac entrance was closed using Vortex-18 Diamond Shape fiber platinum coils (Neomedica, Belgrade, Serbia) and a Vortex Diamond fiber coil (Neomedica), 2/4 mm × 4.1 cm. GDA = gastroduodenal artery; PDAIP = pancreaticoduodenal inferior posterior artery; SMA = superior mesenteric artery.
Sixteen days after the procedure, gastrointestinal bleeding recurred. New angiography revealed refeeding of the aneurysm sac alongside the coil placed into the lesser collateral branch during the first embolization procedure. A stent was placed into the collateral branch artery to prevent migration or protrusion of the previously placed coil. Final arteriography illustrated complete PSA sac occlusion (Figure 5). No further complication was seen during the 26 months of follow-up.
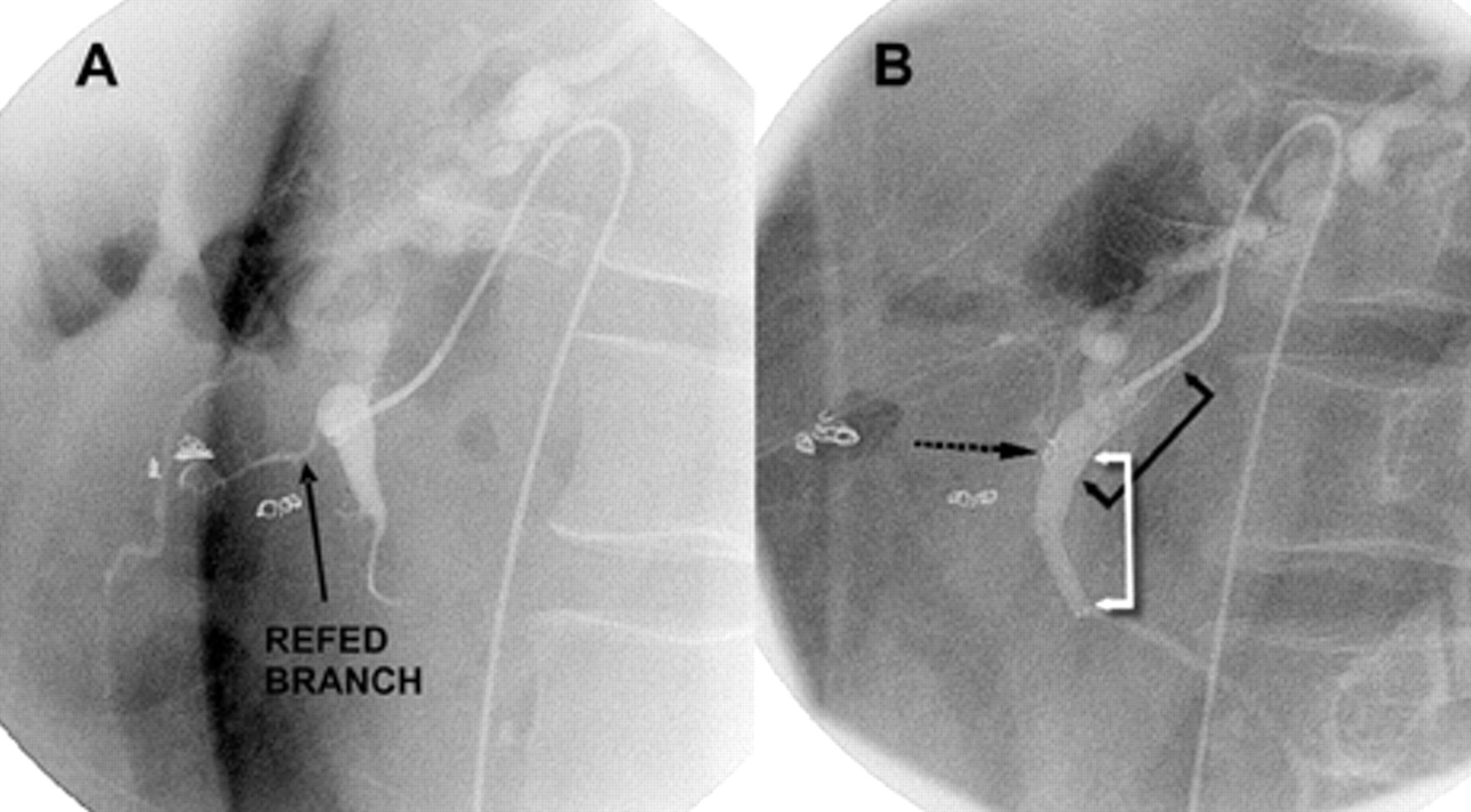
A, The aneurysm sac refeeding alongside the coil placed into the lesser collateral branch during the first embolization. B, A stent was placed into the collateral artery to prevent migration and/or protrusion of the previously placed coil (S.M.A.R.T. control, Cordis [Johnson & Johnson, Belgrade, Serbia], 6 mm × 30 mm). Control arteriography illustrated complete pseudoaneurysm obstruction (black and white arrows point to stent position).
Discussion
A PDA PSA is often seen as a complication of acute or chronic pancreatitis, surgical trauma, and/or infection. Autodigestion caused by leakage of pancreatic, activated proteolytic enzymes may weaken the arterial wall of adjacent visceral arteries (splenic 30–50%, gastroduodenal 10–15%, PDA around 10%) and provoke development of PSA formation. 6 Pancreatitis complicated by a pseudocyst is the major etiologic factor for PSA formation. Rupture of the PSA into the pseudocyst converts the pseudocyst into a PSA. Six to 17% of pancreatic pseudocysts are complicated by hemorrhage. In our case, we could not explicitly define the cause of the developing PSA. 1 Previous surgical trauma or chronic pancreatitis could be the reason. Recognition of such a lesion is essential in preventing a fatal outcome.
On the other hand, our patient had concomitant high-grade hepatic and celiac trunk artery stenosis. As a consequence of the increased flow present within the PDAs caused by hepatic artery and celiac trunk orifice stenosis, true aneurysms can occur. 7,8
To the best of our knowledge, there have been only two reports of a PSA associated with stenosis or occlusion of the common hepatic artery. 8 High-grade stenosis (hemodynamically significant) of the hepatic artery probably additionally raises pressure in the gastroduodenal and PDAs via the pancreaticoduodenal arcade, which could lead to aneurysm formation. 7
Magnetic resonance imaging, ultrasonography, and angiography are reliable in early detection of peripancreatic artery false or true aneurysms, but multislice scanning is the most precise way to visualize aneurysm position, aneurysm size, and anatomic correlation with surrounding organs. Angiography, in itself, has the additional advantage of facilitating embolization of the affected vessel even in emergencies.
The two primary methods of treatment of visceral artery PSAs are either surgery or transcatheter occlusion of the PSA. 1–5,9,10 The standard of care in dealing with PSAs has been surgical intervention. Debate still exists about the best methods of treatment. Surgical treatment of pancreatic PSA should be limited to patients for whom less invasive catheter-based embolization is not technically feasible, for patients who have undergone a failed embolization, or for recurrent PSA after successful embolization.
Otherwise, angiographic embolization has increasingly become the favored therapeutic option in patients who are at increased surgical risk. 2,4,5,9,10 Minimal invasiveness, intra-aneurysmatic thrombosis, aneurysm size regression, and the low rate of complications are the main advantages over surgical treatment. 2,4,5,9–11 Ultimately, the decision as to which treatment should be used was left to the discretion of the surgeon.
Concomitant celiac axis and hepatic artery stenosis additionally requires endovascular management or dilatation to facilitate angiographic access and prevent recurrence of aneurysm formation. A PDA PSA should always be approached from two sides (over the gastroduodenal and superior mesenteric arteries) to avoid retrograde flow. The incidence of recurrent hemorrhage after thrombosis has been reported to be as high as 30% with embolization of a pancreatic PSA. CT and ultrasonography follow-up are mandatory to control the long-term outcome of the procedure. 2
In conclusion, a symptomatic PDA PSA could be successfully treated with coil embolization in a patient who is at high surgical risk. Glue or percutaneous thrombin injection can be either an additional solution to transcatheter fiber coil embolization therapy or the first-line treatment. Our angiographic laboratory did not have previous experience with these materials. Coil embolization of the PSA is technically demanding, especially if we know that the occlusion of all side branches of the PSA by selective embolization is necessary. 2,4,5 Sometimes several attempts may be required for an excellent final result.