
Abstract
Patients diagnosed with steal syndrome after hemodialysis access surgery have a few options for symptom relief while maintaining vascular access. These include fistula lengthening, banding, distal revascularization with interval ligation (DRIL), revision using distal inflow (RUDI) or proximalization of the arterial inflow (PAI). Two cases are described in which a modified DRIL procedure without interval ligation was used to relieve steal syndrome, leaving the arterial supply of an ischemic hand not entirely dependent upon a bypass. Furthermore, a review of the literature is presented in order to elucidate this relatively new treatment option as a viable means to improve hand perfusion while maintaining a functional fistula.
Keywords
Steal syndrome after creation of an arteriovenous fistula for dialysis purposes is a major complication. It has been reported to develop in 1.6 to 8.0% of constructed fistulae. 1 Symptoms range from coldness of the extremity, numbness, and intrinsic muscle weakness to ischemic rest pain and ulceration. 2 When initial signs, such as minor sensory loss, worsen, one should be cautious, and surgical intervention will be inevitable to prevent irreversible damage. Reversed flow in the artery distal to the fistula (the steal phenomenon) is not always associated with hand ischemia. Reversed flow has been documented in up to 73% of radiocephalic fistulae and in up to 91% of brachial artery to axillary vein grafts. 2 Steal syndrome associated with hand ischemia develops only when the collateral circulation is insufficient to produce enough flow antegrade to maintain adequate perfusion of the hand. This can be the case when the patient suffers from peripheral arterial disease or vasculitis in the lower arm. 2
The restoration of adequate hand perfusion with preservation of the fistula would obviously be the preferred treatment. Procedures currently available for the relief of steal syndrome are fistula lengthening, banding, distal revascularization with interval ligation (DRIL), revision using distal inflow (RUDI), 3 or proximalization of the arterial inflow. 4 DRIL has been shown to be the superior treatment so far, with RUDI gaining more popularity because of the reluctance to ligate a brachial artery and leave the arterial supply of an ischemic hand entirely dependent on a bypass. 3 We describe two cases of a modified DRIL procedure to relieve steal syndrome and present a review of the literature to elucidate these relatively new treatment options as a viable means to improve hand perfusion while maintaining a functional fistula.
Case Reports
Case A
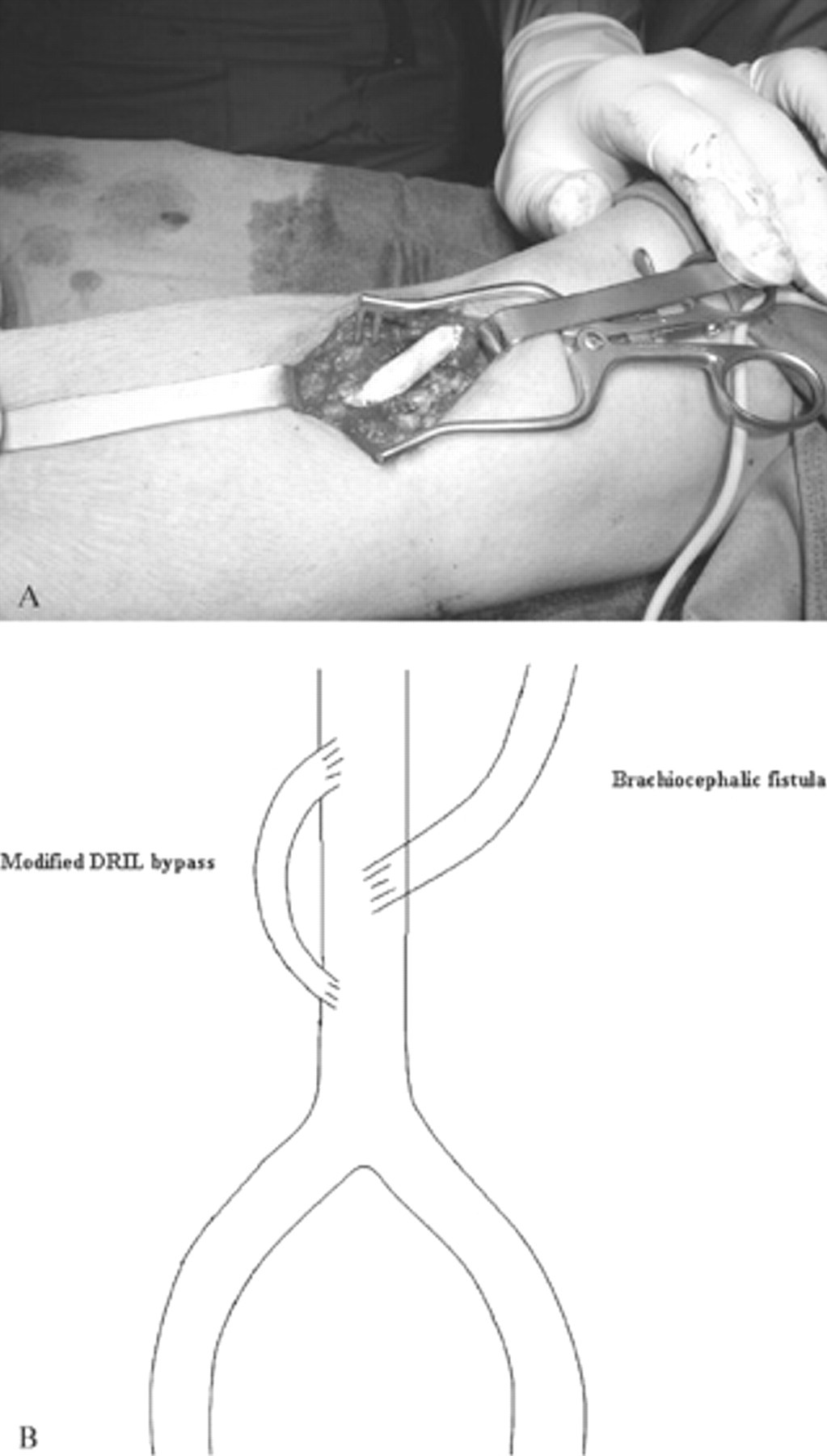
A 60-year-old woman started hemodialysis in July 2005 through a jugular catheter because of end-stage renal disease with an unknown cause. She was evaluated for autogenous fistula creation but was found to have unsuitable veins. A polytetrafluoroethylene (PTFE) loop graft was constructed from the brachial artery onto the median cubital vein of her right arm. Three hours after surgery, she complained of pain and sensorimotor loss in her right hand. The hand was colder and paler compared with the left hand, with a palpable radial pulse, but with retrograde flow in the radial and ulnar arteries at the level of the wrist, as demonstrated on duplex ultrasound scanning. The following day, her symptoms were not improving and revision of the fistula seemed inevitable. The midportion of a 7 to 4 mm tapered vascular graft was placed end to side on the brachial artery proximal to the fistula entrance with the distal end of the new bypass placed end to side onto the distal brachial artery (Figure 1). In contrast to the DRIL procedure, in this case, ligation of the brachial artery between the fistula and the graft was not performed. Intraoperatively, an improvement in flow through the radial and ulnar arteries was seen using handheld Doppler ultrasonography. Directly after the procedure, the hand became warm and pink, with good capillary refill, a palpable radial pulse, and restoration of antegrade flow in the distal brachial artery, as shown on duplex ultrasound scanning. The day after revision, edema of the hand had developed, probably owing to reperfusion. The pain had disappeared, the hand felt markedly warmer, and the patient had more control over her finger movements. However, sensory loss remained in the first three fingers for about 2 weeks. One year after the revision, the PTFE loop is functioning well and is currently used three times a week for two-needle dialysis. In addition, no signs of steal syndrome are currently present.

Modified DRIL procedure as described in case A. A, Intraoperative aspect; B, diagram of midsection of a tapered 7 to 4 mm polytetrafluoroethylene (PTFE) graft.
Case B
An 80-year-old lady started hemodialysis for end-stage renal disease owing to primary oxaluria with persisting urinary tract infections. Six weeks after creation of a brachiocephalic fistula in her left upper arm, a stenosis of the cephalic vein had to be dilated because of a suboptimal developing fistula. Thereafter, she developed critical ischemia in the left hand with severe pain, numbness, retrograde flow on duplex ultrasound scanning, and no palpable radial pulse. Eleven days after this dilation, she underwent a modified DRIL procedure (Figure 2). A 7 to 4 mm midportion tapered PTFE bypass was constructed without ligation of the brachial artery distal to the anastomosis of the fistula. Intraoperatively, after completion of the tapered bypass, the radial pulse was palpable again. Postoperatively, the hand was warm, with a normal color and an improved neurologic status. After 1 month, the fistula and bypass were still patent, but because of chronic back pain owing to an osteoporotic vertebral fracture and with low quality of life remaining, she stopped dialysis and died soon after.
Modified DRIL procedure as described in case B. A, Intraoperative aspect; B, diagram of midsection of a tapered 7 to 4 mm polytetrafluoroethylene (PTFE) graft.
Discussion
The DRIL procedure was first described by Schanzer and colleagues in 1988. 5 They treated three patients who all showed instant relief of steal syndrome symptoms with a patent fistula and bypass for a period of 1 month to 8 years. A number of reports using the original DRIL procedure or a modification appeared thereafter (Table 1).
The modification of the DRIL procedure, which we used to treat symptoms of steal syndrome, included omitting the ligation of the brachial artery between the fistula and the graft. The proximal anastomosis of the new bypass was inserted 3 cm proximal from the fistula as this decreases retrograde flow through the bypass to the fistula. 5 The distal revascularization was done using the midportion of a tapered 7 to 4 mm graft. PTFE was used instead of the great saphenous vein because of its tapered character, and there is some evidence that a thin-walled vein twists and kinks earlier than thick-walled PTFE, especially when it concerns short bypasses. 6 To comprehend why the modified DRIL procedure should work, one can compare flow in the extremity with a Wheatstone bridge, as Wixon and colleagues did. 7 One can imagine that the DRIL bypass functions as a low-resistance collateral; as the total resistance of a parallel circuit is always lower than that of each resistor, the DRIL bypass decreases peripheral resistance and augments blood flow to the extremity. Ligation of the artery distal to the fistula in the DRIL procedure is done to prevent retrograde flow in this artery. 7 However, we did not find any retrograde flow in the distal artery after performing the modified DRIL procedure. The reason for this might be the presence of peripheral arterial occlusive disease, which prevents augmentation of retrograde flow to the fistula after applying the modified DRIL procedure. Given that arterial occlusive disease is associated with end-stage renal failure, some of the patients treated for steal syndrome might be overtreated with the original DRIL procedure as interval ligation is not necessary in all of these cases. Furthermore, ligation has a major disadvantage as it leaves the hand entirely dependent on a manufactured bypass. The use of some kind of intraoperative monitoring of the distal perfusion may be helpful to decide whether ligation is necessary. Monitoring techniques that have been used before include pressure measurements, palpating the radial pulse intraoperatively, and/or Doppler ultrasonography. 1,5 In one of our cases, handheld Doppler ultrasonography was used, and in the other, return of a palpable radial pulse was observed. In future operations, we also decided to use pulse oximetry to be able to define intraoperative improvement in flow more accurately.
This modified DRIL procedure was also described by Gradman and Pozrikidis. 8 They also found that it increased distal flow to the hand. However, they used an extended 6 mm axillobrachial bypass, inserted through a large incisional wound. In our case, only the small incision from the previously created PTFE loop at the level of the brachial artery was reused. In addition, the advantage of this modified DRIL procedure for treatment of steal syndrome is that the native circulation is not ligated and the limb will not be dependent on a manufactured bypass. Furthermore, the procedure is relatively simple, and with the aforementioned, this makes it a promising alternative for the treatment of steal syndrome.
Review of the Literature on the DRIL Procedure
DRIL = distal revascularization with interval ligation; PAI = proximalization of the arterial inflow; PTFE = polytetrafluoroethylene; RUDI = revision using distal inflow.