
Abstract
A 75-year-old man was referred to our hospital because of sudden thoracic pain. A saccular aneurysm of the aortic arch extending on the anterior surface of the aortic arch was found on computed tomographic arteriography. The patient was hemodynamically stable and he was programmed for a staged surgical and endovascular approach (hybrid approach). As a first stage and in order to prevent major cardiac complications due to the overstenting of the left subclavian artery (LSA) with the occlusion of the aortocoronary bypass, the patient underwent a polytetrafluoroethylene bypass graft (GORE-TEX, W.L. Gore & Associates, Flagstaff, AZ) between the LSA and the left carotid artery. Intraoperative arteriography revealed a good patency of the left carotid-subclavian bypass and of the left internal mammary bypass on the left anterior descending artery. As a second stage the endovascular procedure was accomplished 5 days later in the operating room. A Gore TAG stent graft (W.L. Gore & Associates) was deployed in the aortic arch 20 mm proximally to the aneurysmatic segment covering the ostium of the LSA. The postoperative course was uneventful and the patient was discharged on the fifth postoperative day in good general conditions. Hybrid procedures for treatment of aneurysms of the aortic arch or of the descending thoracic aorta are a promising alternative to open surgery especially in high-risk patients, with lower early morbidity and mortality rates. Long-term effectiveness remains to be fully elucidated.
Keywords
Endovascular treatment of aneurysms of the aortic arch and distal thoracic aorta represents an important conquest in vascular surgical practice. Aortic resection and replacement with graft interposition have been the treatment of choice for many years. 1–3 However, after 1991, when Parodi and colleagues performed the first endovascular repair of an abdominal aortic aneurysm 4 and Volodos and colleagues achieved the endoluminal exclusion of a thoracic aortic aneurysm, 5 this technique is presently considered a valid alternative to open surgical repair in selected patients. 6–8 In fact, when compared with conventional repair, thoracic endograft positioning has lower morbidity and mortality rates as it avoids thoracotomy, aortic clamping, and hypothermic circulatory arrest. 8 For safe anchorage of the endograft, we always need a sufficiently extended proximal neck of the aneurysm (proximal landing zone), which should be at least 20 mm long. 9–11 When managing endoluminal repair of aortic arch aneurysms, it may be necessary to cover the ostium of the supra-aortic trunks (SATs). In such cases, debranching of the SAT before endograft positioning should be considered. 9–13 We describe here the case of a patient with a left internal mammary artery (IMA) bypass to the left anterior descending artery (LADA) presenting with sudden thoracic pain and a saccular aneurysm of the aortic arch. To avoid major cardiac complications owing to overstenting of the left subclavian artery (LSA), the patient underwent a polytetrafluoroethylene (PTFE) left carotid-subclavian bypass graft before endovascular exclusion of the aortic arch aneurysm.
Case Report
A 75-year-old man with sudden thoracic pain was referred to our hospital on an emergency basis with the suspected diagnosis of thoracic aortic dissection following computed tomography (CT) of the chest done in another hospital. The patient was hemodynamically stable. Bidimensional angio-CT with three-dimensional reconstruction revealed a saccular aneurysm of the aortic arch measuring 35 mm in diameter, without any sign of dissection, fissuration, or rupture (Figure 1). Digital subtraction angiography further delineated the anatomic features of the aneurysm extending on the anterior surface of the aortic arch (Figure 2). The aortocoronary bypass with the left IMA was patent. In addition, this heavy-smoking patient presented with arterial hypertension, an old inferior myocardial infarction (MI), a previous aortocoronary bypass with the left IMA, and subsequent percutaneous transluminal coronary angioplasty performed 2 months earlier. Preoperative electrocardiography confirmed the presence of the old MI. Serum cardiac markers were normal. A preoperative echocardiogram showed mild cardiac insufficiency with an ejection fraction of 55%. Ultrasound duplex scanning revealed no significant stenosis of both internal carotid arteries. In consideration of advanced age, coronary and pulmonary insufficiency, and previous heart surgery, a high risk for conventional open repair was anticipated (American Society of Anesthesiologists classification III–IV). Antihypertensive therapy was started soon after admission, and a staged surgical and endovascular approach was planned (Figure 3). As a first stage and to prevent the occlusion of the aortocoronary bypass, the patient underwent a PTFE bypass graft (GORE-TEX, W.L. Gore & Associates, Flagstaff, AZ) between the LSA and the left carotid artery via a 5 cm left supra-clavicular transverse incision. The PTFE graft was tunnelized retrojugularly. The LSA was ligated close to its ostium. Intraoperative arteriography revealed good patency of the left carotid-subclavian bypass and of the left IMA bypass on the LADA. As a second stage, the endovascular procedure was accomplished 5 days later. The implantation of a stent graft endoprosthesis was performed in the operating room under epidural anesthesia after full heparinization. A left common femoral percutaneous access with a 6F introducer was prepared for intraoperative angiographic controls with a “pigtail” catheter. The right femoral artery was exposed via an oblique incision. With the support of an extra-stiff 0.035-inch guidewire, a Gore TAG Thoracic Endoprosthesis (W.L. Gore & Associates) was deployed in the aortic arch 20 mm proximally to the aneurysmatic segment covering the ostium of the LSA. The total blood loss did not exceed 250 mL, and the duration of the endograft implantation was approximately 75 minutes. The postoperative course was uneventful. The thoracic pain disappeared after the endovascular procedure. Postoperative angio-CT showed the complete exclusion of the aneurysm, and the patient was discharged on the fifth postoperative day in good general condition (Figure 4). Control angio-CT performed 1 year later showed no increase in the diameter of the aneurysm without any sign of refilling of the sac, endoleak, or graft migration.
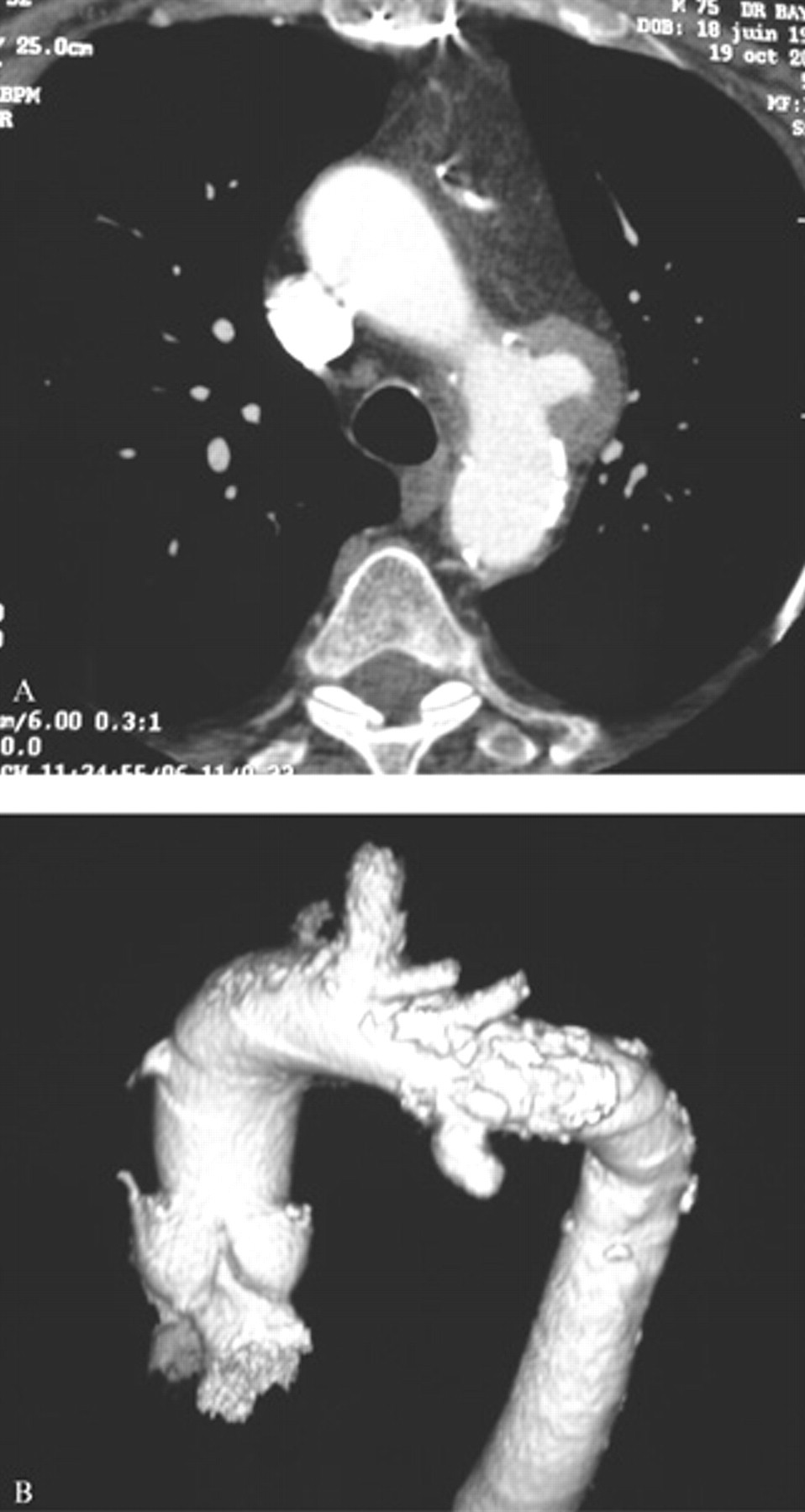
A, Bidimensional angio–computed tomography (angio-CT) revealed a saccular aneurysm of the aortic arch measuring 34.5 mm in diameter, without any sign of dissection, fissuration, or rupture. B, Angio-CT with three-dimensional reconstructions revealed a saccular aneurysm of the aortic arch at the level of the ostium of the left subclavian artery, suitable for endografting on landing zone 2.

Digital subtraction angiography further delineates the anatomic features of the saccular aneurysm of the aortic arch, extending on the anterior surface of the aorta. The aortocoronary bypass with the left internal mammary artery (IMA) is patent.

Hybrid approach: a polytetrafluoroethylene bypass graft between the left subclavian artery and the left carotid artery was performed to prevent occlusion of the aortocoronary bypass. The subclavian artery was ligated close to its ostium to prevent an endoleak. A Gore TAG Thoracic Endoprosthesis (W.L. Gore & Associates) was deployed in the aortic arch on proximal landing zone 2, 20 mm proximal to the aneurysmatic segment, covering the ostium of the left subclavian artery. aaa = aortic arch aneurysm; csb = carotid subclavian bypass; lca = left carotid artery; lma = left mammary artery; lsa = left subclavian artery; rca = right carotid artery; rsa = right subclavian artery.

Control angio–computed tomographic scan showing the correct positioning of the endograft deployed on proximal landing zone 2 and the complete excision of the saccular aneurysm of the aortic arch with no signs of endoleak. The left carotid artery and the innominate trunk are patent.
Discussion
Thoracic aortic aneurysms reportedly affect about 6 persons per 100,000 population each year, 1–3 and this number is increasing because of increased access to diagnostic procedures and of population aging. Risk factors are typically hypertension, coronary artery disease, obstructive pulmonary disease, and heavy smoking. Endoluminal repair of thoracic aortic aneurysms has emerged as a new therapeutic strategy, with encouraging early and midterm results. Reportedly, it reduces the need for open repair. 6–8 The lower perioperative morbidity of endovascular treatment compared with open surgery is especially important when managing high-risk patients. Neck diameters, adequacy of the landing zone, and iliofemoral tortuosity or stenosis represent the limits of feasibility of endoluminal exclusion of thoracic aortic aneurysms. Procedures of debranching of the supra-aortic vessels may be necessary to manage aortic arch aneurysms. 9–13 These procedures will allow safe covering of the SAT by the endograft and will increase the length of the landing zone, which must be at least 2 cm long, preventing migration or type 1 endoleaks. Recent reports have underlined the importance of classification of the endograft landing zones in the thoracic aorta. 9–11 We prefer to use the retrograde landing zone classification (Figure 5) suggested by Bergeron and colleagues. 10 Four proximal landing zones are identified, the severity of the anatomic involvement ranging from zone 1, the ideal situation in which no additional operation is required, to zone 4, which represents the most complex condition in which it is necessary to overstent the whole aortic arch. In our patient, landing zone 2 was present, as shown on three-dimensional angio-CT (see Figure 1B). In this situation, the intentional overstenting of the LSA is indicated. In selected cases, prophylactic revascularization of the LSA should also be considered. In keeping with other authors, we recommend the latter procedure whenever an aortocoronary bypass is present or foreseen. 14 Moreover, revascularization of the LSA will be necessary, always as a first stage, whenever an arteria lusoria or a bypass to another vascular district is present (ie, axillofemoral bypass graft). Arteriovenous hemodialysis access to the left arm, when present, may represent an additional indication. Alternatively, revascularization of the LSA may be needed later if the patient develops subclavian steal syndrome or signs of hypoperfusion of the left upper limb. When the landing zone of the endograft is at the level of the origin of the innominate artery or of the left common carotid artery (zones 3 and 4), prophylactic revascularization of these main aortic vessels is mandatory. Alternatively, to avoid open surgery of the SAT, fenestrated and branched endoprostheses were recently developed. However, these grafts are still under clinical evaluation to prove their safeness and effectiveness, not only at the level of the aortic arch 15 but also of the thoracoabdominal aorta. 16,17
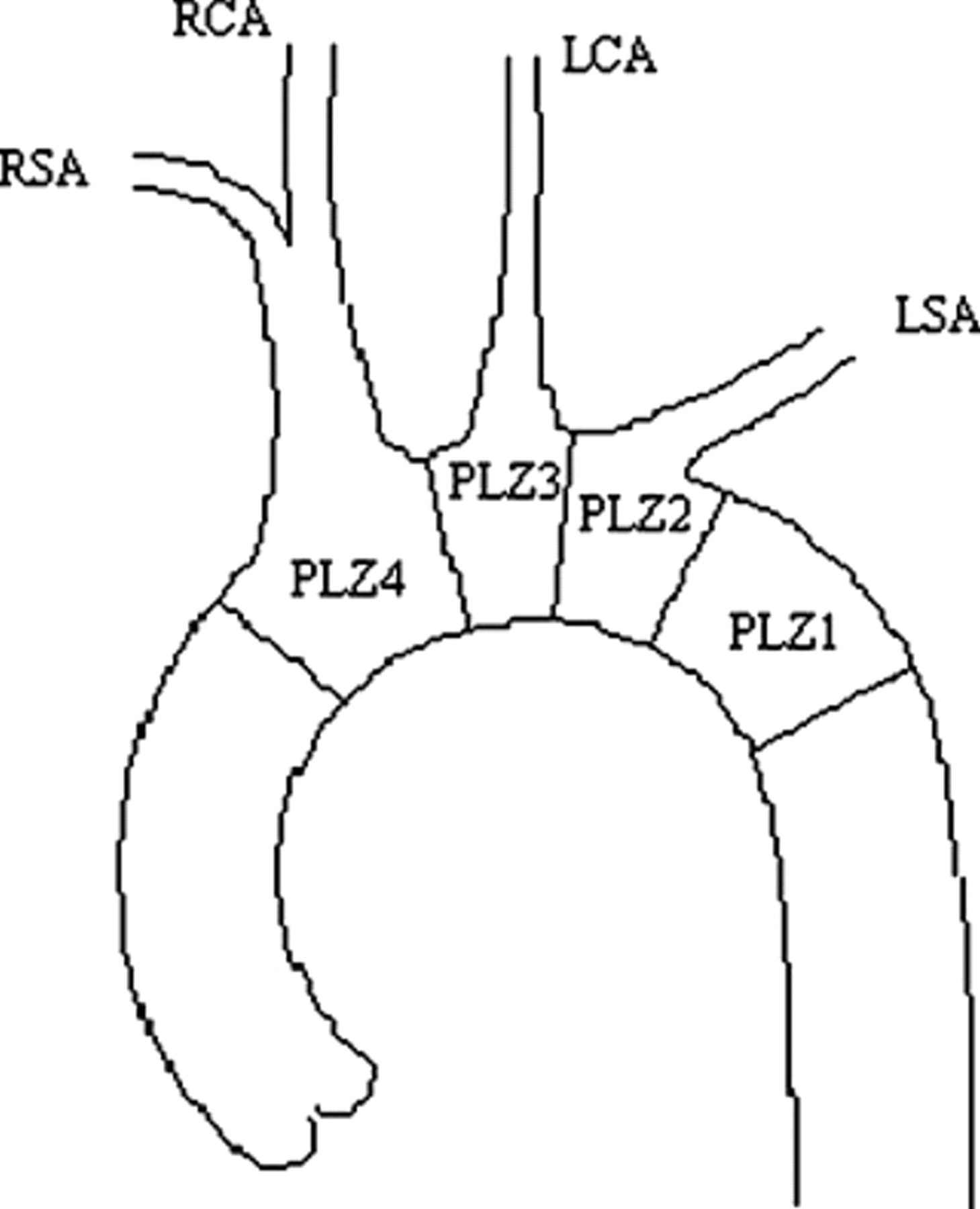
Retrograde proximal landing zone (PLZ) classification: it considers four PLZ, the severity of the anatomical involvement ranging from PLZ1 to PLZ4: zone 1 is located on the descending thoracic aorta distally to the left subclavian artery (LSA). Zone 2 is situated at the level of the origin of the LSA. Here the intentional overstenting of the LSA can be alone or associated to the revascularization of this artery. Zone 3 and 4 are respectively at the level of the left common carotid artery and of the innominate artery. Here the prophylactic revascularization of these main aortic vessels is mandatory. RSA=right subclavian artery; RCA=right carotid artery; LCA=left carotid artery.
In conclusion, hybrid procedures are a promising alternative to open surgery for the treatment of aneurysms of the aortic arch or of the descending thoracic aorta, especially in high-risk patients, with lower early morbidity and mortality rates. The long-term effectiveness remains to be fully elucidated.