
Abstract
Atherosclerosis in the form of peripheral arterial disease results in significant morbidity and mortality. Surgical treatment options for peripheral arterial disease include angioplasty with and without stenting, endarterectomy, and bypass grafting. Unfortunately, all of these procedures injure the vascular endothelium, which impairs its ability to produce nitric oxide (NO) and ultimately leads to neointimal hyperplasia and restenosis. To improve on current patency rates after vascular procedures, investigators are engaged in research to improve the bioavailability of NO at the site of vascular injury in an attempt to reduce the risk of thrombosis and restenosis after successful revascularization. This article reviews some of the previous research that has aimed to improve NO bioavailability after vascular procedures whether through systemic or local delivery, as well as to describe some of the NO-releasing products that are currently undergoing study for use in clinical practice.
Atherosclerosis in the form of peripheral arterial disease (PAD) affects approximately eight million Americans, which includes 12 to 20% of individuals over the age of 65. 1 Approximately 20% of patients with PAD have typical symptoms of lower extremity claudication, rest pain, ulceration, or gangrene, and one-third have atypical exertional symptoms. 2 Persons with PAD have impaired function and quality of life even if they do not report symptoms and experience a decline in lower extremity function over time. Cardiovascular disease is the major cause of death in patients with intermittent claudication; the annual rate of cardiovascular events (myocardial infarction, stroke, or death from cardiovascular causes) is 5 to 7%. 3 Thus, PAD represents a significant source of morbidity and mortality.
Several options exist for treating atherosclerotic lesions, including percutaneous transluminal angioplasty with and without stenting, endarterectomy, and bypass grafting. Unfortunately, patency rates for each of these procedures continue to be suboptimal secondary to the development of neointimal hyperplasia. A universal feature of all vascular surgical procedures is the removal of or damage to the endothelial cell monolayer that occurs whether the procedure performed is endovascular or open. This endothelial damage leads to a decreased or absent production of nitric oxide (NO) at the site of injury (Figure 1).
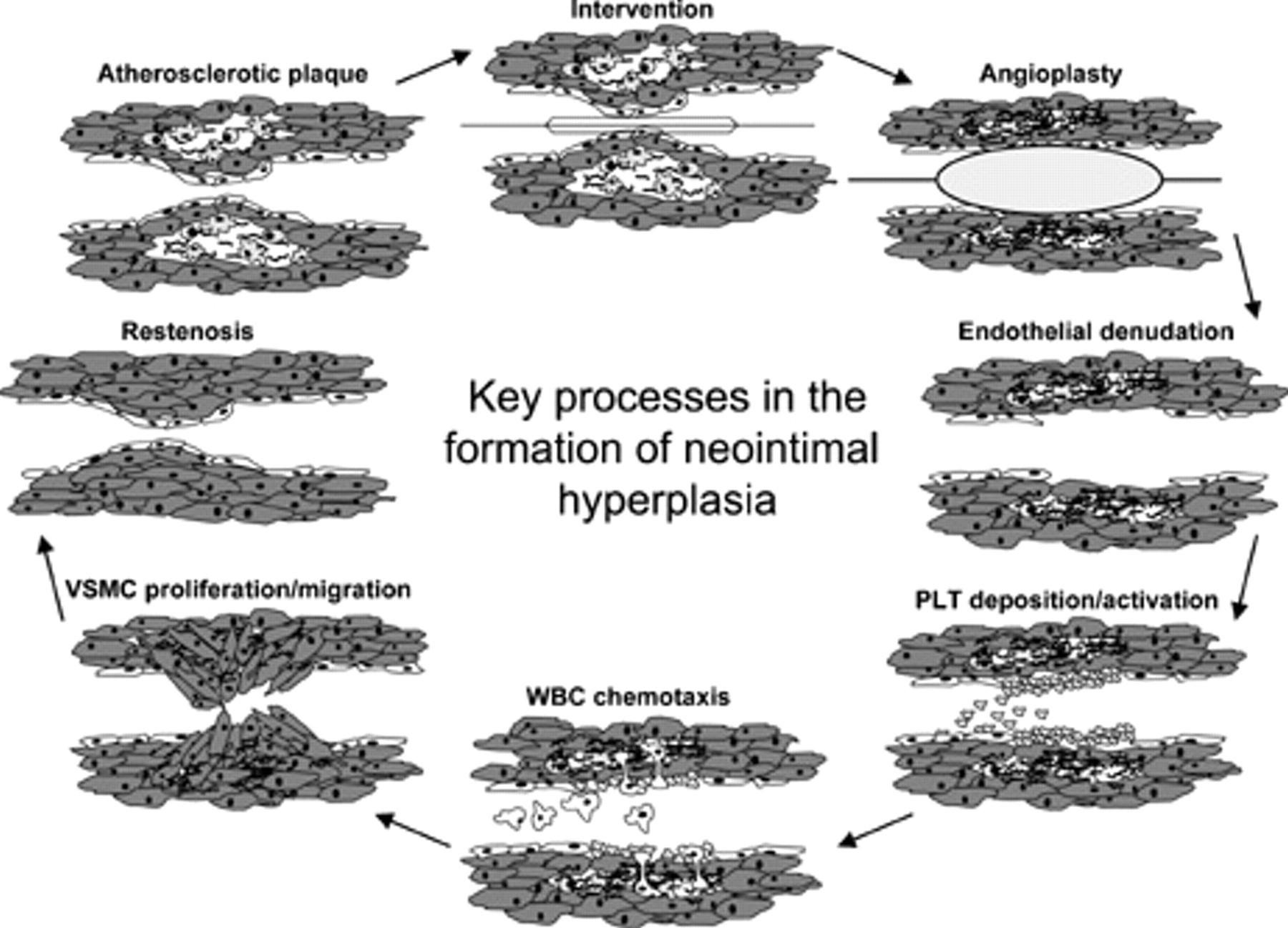
Schematic of neointimal hyperplasia. After vascular interventions, such as balloon angioplasty, the endothelial cell monolayer is removed and/or damaged. This leads to platelet adhesion and activation, which is followed by leukocyte chemotaxis. Vascular smooth muscle cells begin to proliferate and migrate from the media to the intima, forming the neointima, which leads to restenosis. PLT = platelet; VSMC = vascular smooth muscle cell; WBC = white blood cell.
In 1980, Furchgott and Zawadski discovered that intact endothelial cells produced a substance in response to acetylcholine stimulation. 4 This substance, termed endothelium-derived relaxing factor (EDRF), was produced only when endothelial cells were present and acted on vascular smooth muscle cells (VSMCs) to produce relaxation. Several years later, simultaneous work by two different scientists proved that EDRF is NO. 5,6 The relationship between NO and the cardiovascular system has proven to be a landmark discovery, and the scientists credited for its discovery were awarded the Nobel Prize in Medicine in 1998. Since its discovery, NO has proven to be one of the most important molecules in vascular homeostasis. In fact, the term endothelial dysfunction has now become synonymous with the reduced biologic activity of NO. 7
NO produced by endothelial cells has been shown to have many beneficial effects on the vasculature. As described above, NO stimulates VSMC relaxation, which leads to vessel vasodilatation. 8 NO has opposite beneficial affects on endothelial cells compared with VSMCs. Whereas NO stimulates endothelial cell proliferation 9 and prevents endothelial cell apoptosis, 10 it inhibits VSMC growth and migration 11,12 and stimulates VSMC apoptosis. 13 NO also has many thromboresistant properties, such as inhibition of platelet aggregation, adhesion, and activation 14 ; inhibition of leukocyte adhesion and migration 15 ; and inhibition of matrix formation (Figure 2). 16 Because these properties are governed by NO, the endothelial cell monolayer is one of the most thromboresistant substances known. 17 As stated before, the endothelial cell monolayer is often removed or damaged during the time of vascular procedures, which leads to a local decrease in the production of NO. It is now understood that this loss of local NO synthesis by endothelial cells at the site of vascular injury is one of the inciting events that allows platelet aggregation, inflammatory cell infiltration, and VSMC proliferation and migration to occur in excess, which, taken together, leads to neointimal hyperplasia.
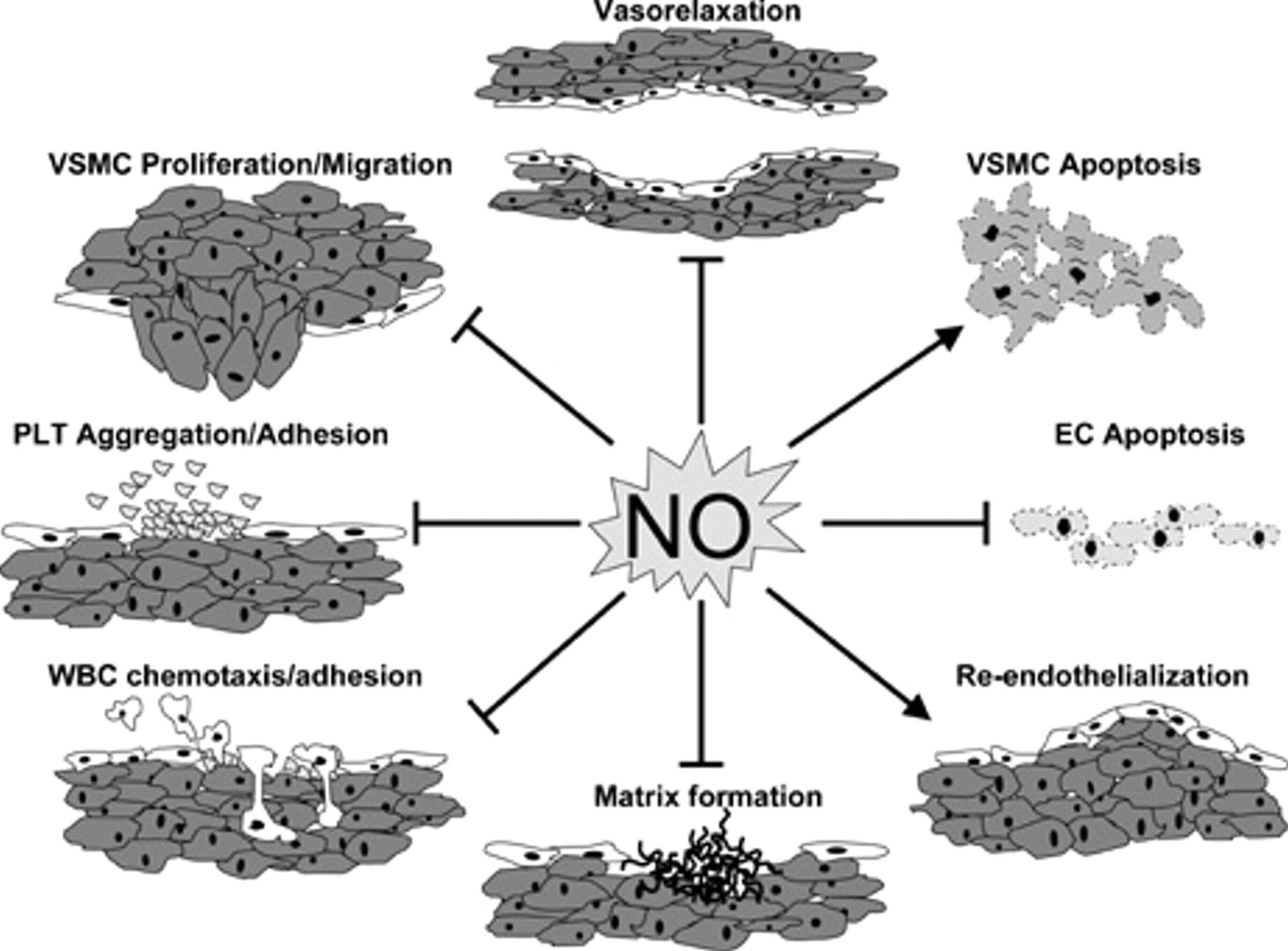
Beneficial properties of nitric oxide (NO) in the vasculature. EC = endothelial cell; PLT = platelet; VSMC = vascular smooth muscle cell; WBC = white blood cell.
Reendothelialization of the injured artery can restore proper function to the artery and potentially halt the restenotic process. 18 Many studies have attempted to improve the patency of bypass grafts and stents by coating them with endothelial cells in the hope that this would restore the thromboresistant nature of native blood vessels. 19–21 Unfortunately, although it has been possible to coat these devices with endothelial cells, these cells do not behave like normal endothelial cells and their NO production is often diminished or absent. Because the vasoprotective properties of endothelial cells are largely carried out by NO alone, investigators are engaged in research to improve the bioavailability of NO at the site of vascular injury in an attempt to reduce the risk of thrombosis and restenosis after successful revascularization. The overall goal of using a NO-based approach is to reproduce the same thromboresistive moiety observed with normal NO production.
Systemic Delivery
One simple mechanism by which to deliver NO to the body is via inhalational therapy. Inhaled NO has been used clinically in the past to selectively reduce pulmonary vascular resistance in patients with pulmonary hypertension, as well as a potential therapy for patients with acute respiratory distress syndrome. Because the gas is delivered only to the pulmonary system and has a very short half-life, it was thought that there would be no systemic effects of the drug. Subsequently, studies in the mid- to late 1990s suggested that inhaled NO had beneficial antiplatelet and antileukocyte properties without adverse systemic side effects. 22,23
To test if inhaled NO had any beneficial systemic properties specifically on the vasculature, Lee and colleagues evaluated the effect of inhaled NO on neointimal hyperplasia in rats undergoing carotid balloon injury. 24 Beginning 60 minutes before carotid injury, rats were exposed to air with 0 or 80 ppm of NO for 14 days. Although neointimal hyperplasia was evident in control and treatment groups, a 43% reduction was observed in the NO-treated group. It was also observed that NO did not cause any adverse effects on bleeding time or blood pressure, and the authors speculated that this modality of treatment could represent an adjunct to preventing restenosis after percutaneous transluminal coronary angioplasty (PTCA). Unfortunately, the treatment was required for the full 2 weeks to see any difference between the treatment and the control group, thereby limiting its clinical utility.
Despite some of the early animal studies, investigations with healthy human volunteers failed to reproduce these findings. 25 It was speculated that despite the obvious effects of inhaled NO on the pulmonary vasculature, systemic bioavailability could not be reliably achieved because of the immediate binding and depletion of NO by hemoglobin as soon as it entered the systemic circulation.
Hamon and colleagues tested the ability of orally supplementing
To test the ability of this supplemented diet to reduce neointimal hyperplasia in a vein bypass graft model, Davies and colleagues fed rabbits
Landis and colleagues performed a similar study in dogs. They placed saphenous veins as interposition grafts into the bilateral femoral arteries of 24 mongrel dogs.
28
A clamp was then placed on one side to reduce the flow in that vein graft by 50%. Twelve dogs were fed a normal diet, and 12 dogs were fed a diet supplemented with
Despite some of the positive findings in animals, similar studies in humans have failed to show any benefit with
Dudek and colleagues examined the long-term effects of
Another example of a NO-donating drug is the hybrid drug NO-releasing aspirin. It was originally developed to help combat the ulcerogenic properties of aspirin despite its excellent cardioprotective effects. Furthermore, NO was found to have added protective effects on the vasculature over aspirin alone. Napoli and colleagues examined the effects of a NO-releasing aspirin called NCX-4016 (55 mg/kg) on adult and aging rats using a balloon carotid artery injury model. 32 The drug was shown to reduce the neointimal area in adult (18.2 ± 1.8 vs 31.8 ± 2.9, p < .01) and aging rats (24.1± 1.6 vs 44.9± 3.6, p < .01) compared with untreated controls. The drug was also found to have less ulcerogenic activity compared with aspirin alone (30 mg/kg). The authors proposed that this drug could be used as an adjunct to bypass surgery in older patients and those with gastrointestinal damage.
Shukla and colleagues examined the effect of three different NO-releasing aspirin drugs on human saphenous vein grafts and human VSMCs in vitro. 33 They found that these drugs elicited relaxation of isolated human saphenous vein, promoted cGMP formation, and inhibited VSMC proliferation, whereas aspirin alone had no effect on any of these variables. The authors speculated that these drugs could be used to prevent early and late thrombosis secondary to vein spasm and neointimal hyperplasia.
Two other examples of NO-donating drugs that can be delivered systemically are linsidomine and molsidomine. They are members of the sydnonimine antianginal class of drugs (Table 1). Both drugs have been used as NO donors for the treatment of hypertension and angina. A benefit of their use over the more conventional use of organic nitrates is that there is no demonstrated tolerance to their effectiveness. One of the first studies that examined molsidomine's ability to reduce neointimal hyperplasia after vascular procedures was performed by Groves and colleagues. 34 Carotid angioplasties were performed on pigs to induce vascular injury. The pigs were given either oral molsidomine (0.3 mg/kg every 8 hours) or placebo for 48 hours before the procedure and continued administration until the time of vessel harvesting (7 or 21 days). A significant reduction in VSMC proliferation was seen in the treatment group compared with placebo. Although NO inhibited VSMC proliferation following angioplasty, it had no significant influence on VSMC migration or extracellular matrix production within the intima. Furthermore, this reduction in VSMC proliferation was present only if the internal elastic lamina had not been ruptured by balloon dilation.
Comparison of Different Nitric Oxide Donor Drugs Currently Used for Clinical or Research Purposes
NO = nitric oxide; NOS = nitric oxide synthase.
One of the only studies that examined the use of these drugs systemically to reduce neointimal hyperplasia in humans was the ACCORD Study. 35 This was a prospective randomized multicenter trial in which 700 patients with stable angina underwent PTCA. It compared the effect of intravenous infusion (1 mg/h) of linsidomine at the time of PTCA and subsequent oral administration of molsidomine (12 mg/day) orally for 6 months with that of oral diltiazem (180 mg/day) alone. All patients received aspirin postoperatively. The study revealed only a moderate improvement in restenosis in the treatment group on long-term angiographic follow-up, but this did not correlate with improved clinical outcome or late lumen loss.
Several years later, Wohrle and colleagues performed a randomized, placebo-controlled, double-blinded trial that compared oral molsidomine with placebo and their ability to inhibit neointimal hyperplasia after PTCA. 36 No statistically significant differences were found between the two groups, although the molsidomine treatment group did have significantly improved angina compared with the placebo group.
Despite the ease of administration, the reliability of drug delivery, and the relative safety of these NO-donating drugs, there are limitations associated with systemic administration. One such limitation is that NO is rapidly inactivated by hemoglobin in the circulating blood, resulting in limited bioavailability. Furthermore, in attempts to increase the amount of drug delivered to obtain the desired clinical effect, unwanted systemic circulatory effects (eg, vasodilation) and unwanted hemostatic effects (eg, bleeding) often preclude administration of biologically effective doses of NO. 37 Because NO produces systemic side effects, lower doses of NO have been used in many of the human studies. One of the reasons for the differences observed between the animal studies and the human studies was the 10- to 50-fold lower doses of drugs used in the human studies compared with the animal studies. Thus, local delivery of NO may achieve improved results. 38
Local Delivery
The local delivery of drugs allows for the administration of the maximally effective dose of a drug without the unwanted systemic side effects. Because the target vessels are easily accessible during most vascular procedures, a local pharmacologic approach to administer a drug during the intervention can be easily performed.
Because of the mixed results seen in the use of systemic
Later studies sought to find out if the local administration of
Because it was not known if the addition of
A study by Kalinowski and colleagues examined the ability of three locally delivered drugs to the area of arterial injury to decrease neointimal hyperplasia compared with untreated controls.
38
The three drugs used were
Although there are promising findings in these studies, the process by which the vessels were exposed to
Diazeniumdiolates are NO donors, which are formed by the reaction of secondary amine structures with two moles of NO under high pressure (see Table 1). 42–44 They generate bioactive NO in physiologic fluids (37°C, pH 7.4) spontaneously (ie, without metabolism or redox activation), with reliable half-lives ranging from 2 seconds to many weeks depending on the ionic structure. 45 The major advantage of using diazeniumdiolates as NO donors is that they are stable as solids but can be triggered to release NO at controlled rates on hydrolysis or other chemical reactions. Given that most of these compounds generate two moles of NO on activation, the exact amount of NO delivered can be calculated by knowing the amount of diazeniumdiolate that was administered. 46 This quality has made them very useful research tools as reliable and stable sources of NO to probe into its protective or toxicologic roles. At present, diazeniumdiolates have not been used clinically, although they have been evaluated in experimental animal models of cardiovascular disease.
The second class of NO-donating drugs that are currently being widely studied is S-nitrosothiols (see Table 1). S-Nitrosothiols are thought to serve as a reservoir and transporter of NO within biologic systems. 47 S-Nitrosothiols are formed by the S-nitrosation of thiols or cysteine residues. Examples of endogenous S-nitrosothiols are S-nitrosoalbumin, S-nitrosoglutathione, and S-nitrosocysteine. 48 These S-nitrosothiols are present in the circulating blood and also found within cells. 49 They release NO by three known mechanisms 50 : copper ion-mediated decomposition, 51 direct reaction with ascorbate, 52 and homeolytic cleavage of the S-NO bond by light. 53 Like diazeniumdiolates, S-nitrosothiols are not clinically used at present, but they are being extensively studied for use in vascular pathology owing to the different mechanisms by which they release NO.
One mechanism to deliver NO locally to the area of vascular injury at the time of surgery is to use hydrogels. Hydrogels allow for uniform diffusion of drugs into the arterial wall while minimizing drug losses in the bloodstream and side branches. 54 One of the first studies to create NO-releasing hydrogels for the intended use as tissue coatings to provide local and sustained NO therapy following vascular injury was done by Fulton and colleagues. 55 The effect of a single dose of locally applied S-nitroso-N-acetylpenicillamine (SNAP) in a pluronic gel on the formation of neointimal hyperplasia was examined. The jugular veins of rabbits were harvested, and their outer surface was coated with this NO-containing gel before being reimplanted as carotid bypass grafts on the contralateral side. The animals were sacrificed at 28 days, and the authors found that the SNAP-treated groups exhibited a 36% decrease in mean intimal thickness compared with controls.
Further improvements in creating NO-releasing gels and making their delivery more simple were performed by Bohl and West. 56 They created hydrogels using different NO-releasing compounds (diazeniumdiolates and S-nitrosothiols). In vitro testing showed that all of their NO-hydrogel preparations were able to inhibit VSMC proliferation and exhibited significantly less platelet adhesion compared with controls. The authors speculated that the ease of creating these hydrogels and the ease of handling them would be well suited for their application to injured arteries in the operating room to prevent thrombosis and restenosis.
One of the first in vivo animal studies that used NO-releasing hydrogels was performed by Kaul and colleagues. A polymer of polylactic-polyglycolic acid matrix (Atrigel) containing the diazeniumdiolate 1-{N-[3-Aminopropyl]-N-[4-(3-aminopropylammoniobutyl)]}diazen-1-ium-1,2-diolate (SPER)/NO was applied to the outside of balloon-injured rat ileofemoral arteries. 37 Atrigel has the unique ability to exist as a liquid below body temperature but solidifies into a viscous mass when it comes into contact with tissue at body temperature. The polymer gel enables a depot drug delivery in which the NO donor is released over several days as it biodegrades, with complete resorption in about 14 days. There were no bleeding complications in any of the rats studied. The authors found that the NO donor reduced neointimal hyperplasia by about 75% compared with controls.
To examine if it was possible to use NO-releasing hydrogels via the endovascular route, Rolland and colleagues coated an angioplasty balloon with a hydrogel containing the NO donor molsidomine. 54 Angioplasties were then performed on the iliac arteries of pigs that were fed atherogenic diets. The arteries were examined at 3 hours, 24 hours, and 3 months after treatment. Although there were no observed effects at 3 hours, at 24 hours, the treated arteries exhibited better thromboresistance and vascular cell homeostasis. At 3 months, the treated groups exhibited fewer stenotic lesions.
Masters and colleagues developed a polyethylene glycol hydrogel that was covalently modified with the NO donor S-nitrosocysteine that could release NO for approximately 24 hours. 57 After performing in vitro studies to identify the optimal concentration of the NO donor to enhance endothelial cell growth while at the same time inhibiting VSMC proliferation, they examined its effect on reducing neointimal hyperplasia formation when applied directly to the external surface of the artery in a rat carotid artery injury model. The treatment groups were found to have 75% less neointimal formation at 14 days.
The results from these initial studies with NO-releasing hydrogels appear promising for their potential use in vascular surgical procedures. One drawback of their use is that they all have to be made at the time of the surgery, which could prove to be inconvenient. Another way to deliver NO to the arterial wall is by using biopolymers that can be stably stored and, when used, release various reliable amounts of NO over extended periods of time. Frost and colleagues noted that polymeric materials that can release or generate NO locally at fluxes that are equal to or greater than the normal endothelial cell layer for extended periods of time may provide the ultimate route to solve the issues of both thrombosis and stenosis that occur after biomedical implants and/or vascular procedures. 58
Smith and colleagues were the first to use diazeniumdiolates as NO donors in polymers and then incorporate those polymers into vascular grafts. 59 They dipped 4 mm expanded polytetrafluoroethylene (ePTFE) grafts (GORE-TEX, W.L. Gore & Associates, Elkton, MD) into a freshly prepared solution of poly-(ethylenimine) (PEI) and a cross-linking agent such that the cross-linked PEI chains became intimately interwoven with the graft. The grafts were then exposed to gaseous NO to create diazeniumdiolate groups on the PEI. These grafts were shown to produce NO for several weeks in vitro, and they exhibited decreased platelet deposition and VSMC proliferation compared with untreated grafts. These grafts were then inserted as arteriovenous shunts into baboons for 1 hour, and analysis showed that there was significantly less platelet deposition on the NO-releasing vascular grafts compared with untreated grafts. Although this technique initially looked promising, the coating process changed the architecture of the graft, which the authors speculated might create long-term biocompatibility complications secondary to compliance mismatch.
In an attempt to preserve the graft architecture, Pulfer and colleagues incorporated polymeric diazeniumdiolate PEI/NO microspheres into the pores of an ePTFE graft (GORE-TEX). 60 These grafts retained the same physical properties as control grafts even after the addition of the microspheres, with the added benefit that they released NO in vitro for greater than 150 hours. Another method of incorporating NO donors into vascular grafts without altering their mechanical properties is to coat the inside lining with a NO-eluting polymer, which would not alter the architecture of the graft material. Zhang and colleagues created diazeniumdiolated silica nanoparticles and embedded them into hydrophobic matrixes, which were used to coat the inside of tubing used for extracorporeal venovenous circuits in a rabbit model. 61 NO release was substantial, and there was much less platelet consumption and activation when compared with controls when in contact with blood for 4 hours.
Fleser and colleagues coated 5 mm polyurethane grafts (Vectra, Thoratec Corporation, Pleasanton, CA) with multiple layers of a polyvinyl chloride film containing a diazeniumdiolate. 62 In vitro studies showed that NO release was linear up to 7 days and that NO release generated after 25 days was still above that which is produced by functional endothelial cells in vivo. Twelve grafts (three uncoated grafts, four sham-coated grafts, and five NO-releasing grafts) were implanted as arteriovenous grafts into sheep connecting the common carotid artery to the ipsilateral jugular vein. The results showed that all three uncoated grafts had occluded, two of the sham-coated grafts had occluded by 3 weeks, and only one of the NO-releasing grafts had occluded. Although there was a significant reduction in surface thrombus accumulation in the NO-releasing grafts compared with sham-coated and uncoated grafts, a statistically significant improvement in patency was not observed.
Another mechanism by which to use NO-releasing polymers is to incorporate them into currently used vascular prosthetics such as stents and bypass grafts. Yoon and colleagues incorporated sodium nitroprusside (SNP) into a polyurethane polymer and coated this onto metallic coiled stents. 63 Despite showing that there was a biologic effect of NO up to 14 days after implantation via increased cGMP levels, no reduction in neointimal hyperplasia in porcine carotid arteries was observed at 28 days.
Hou and colleagues examined the effects of a NO-eluting covered stent on neointimal formation in a porcine carotid balloon injury model. 64 The interior of a self-expanding ePTFE-covered aSpire stent was coated with silicone, which contained two different concentrations of SNP. When angiograms were performed at 28 days, a 24% reduction of vessel narrowing in the NO-treated groups was observed.
Jun and colleagues incorporated a diazeniumdiolate into a biocompatible polyurethane graft (PUBD-NO) to assess the ability of this material to promote graft endothelialization while preventing thrombus formation and neoinitimal hyperplasia. 65 The mechanical properties of this modified graft were comparable to unmodified polyurethane grafts and to native tissue. The grafts released a measurable amount of NO for up to 2 months. In vitro studies showed that the grafts were able to inhibit VSMC proliferation and stimulate endothelial cell growth while at the same time inhibit platelet adhesion. The authors speculated that the properties of this graft would be ideally suited for bypass grafting and exhibit less neointimal hyperplasia than conventional bypass grafts. 66 To date, there have been no clinical studies evaluating these types of grafts for the purpose of decreasing neointimal hyperplasia after vascular procedures.
Gene therapy represents another method by which to locally increase the level of NO at the site of vascular injury. Like other local therapies, one of the novel characteristics of gene therapy–based approaches is the ability to manipulate only the bypass graft or the target vessels with little or no systemic effects. 67 Unlike the local delivery of NO-releasing drugs, which would eventually be depleted and washed away, the local delivery of NOS genes provides the ability to release NO for longer periods of time at the site of vascular injury.
The first published study using nitric oxide synthase (NOS) gene transfer for the inhibition of neointimal hyperplasia was by von der Leyen and colleagues in 1995. 68 An endothelial NOS–expressing plasmid was used to increase NO production in injured rat carotid arteries via a modified liposome. It was found that not only was endothelium-dependent relaxation restored in the treatment group, but a 70% reduction in neointimal hyperplasia was also observed at 14 days (Figure 3). This study proved that it was possible to provide sustained levels of NO production following transfection of a NOS gene, and this NO had beneficial therapeutic effects on the vasculature after injury. 69

Effect of endothelial nitric oxide synthase infection on neointima formation in balloon injured rat carotid arteries. A, Uninjured; B, injured and untreated; C, injured and infected with the control vector; D, injured and infected with endothelial nitric oxide synthase. M = media; N = neointima (×25 original magnification, hematoxylin-eosin stains). Reproduced with permission from von der Leyen HE et al. 68 Copyright (1995) National Academy of Sciences, U.S.A.
Subsequently, Shears and colleagues described the preclinical evaluation of NOS gene transfer using inducible nitric oxide synthase (iNOS). 70 iNOS was chosen because it had been shown to produce much larger quantities of NO in a calcium- and agonist-independent fashion. 71 An adenoviral vector carrying the human inducible nitric oxide synthase complementary deoxyribonucleic acid (DNA) (AdiNOS) was constructed. Transfection of balloon-injured rat carotid arteries with AdiNOS resulted in a > 95% reduction in neointimal hyperplasia 2 weeks postinjury. Next, AdiNOS was evaluated in a preclinical model, namely, the porcine iliac artery balloon injury model. AdiNOS-transfected arteries were found to have 51.8% less neointimal hyperplasia 3 weeks after injury. Kibbe and colleagues investigated the ability of this same AdiNOS construct to inhibit neointimal hyperplasia in the setting of a vein bypass graft. 72 Interposition jugular vein grafts transfected with AdiNOS anastomosed to the carotid arteries of pigs were found to have less vein graft neointimal hyperplasia at 21 days compared with controls.
Further demonstrating the ability to site-specifically overexpress the NOS gene, Pfeiffer and colleagues used a balloon catheter delivery system, the Infiltrator Drug Delivery Balloon System (Infiltrator, InterVentional Technologies Europe Ltd, Lisnenan, Letterkenny, Co Donegal, Ireland), to inject iNOS into the carotid arterial walls of foxhound dogs at the proximal and distal anastomosis of ePTFE bypass grafts. 73 At 6 months, less neointimal hyperplasia was found at both the proximal and distal anastomoses. This included the prosthetic wall, suture region, and arterial wall. At the proximal anastomosis, the reduction in neointimal hyperplasia was 43%, 52%, and 81%, and at the distal anastomosis, the reduction was 40%, 47%, and 52%, respectively, for the three defined locations. The authors pointed out that this study demonstrates the ability of a single local transfection to decrease neointimal hyperplasia even at 6 months.
Using another NOS gene, West and colleauges performed jugular-carotid interposition grafts in rabbits transfected with neuronal nitric oxide synthase (nNOS) via an adenoviral vector. 74 At 3 days, NOS activity was significantly increased, and this caused a substantial reduction in adhesion molecule expression and inflammatory cell infiltrate. At 28 days, although nNOS expression was no longer present, there was a reduction in neointimal hyperplasia by almost 50% and reduced vascular superoxide production.
Because of the promising in vitro and in vivo studies, several researchers attempted to start a randomized clinical trial in humans using gene therapy to reduce neointimal hyperplasia. In December 2000, the Recombinant DNA Advisory Committee at the National Institutes of Health voted unanimously to proceed with the first phase of clinical evaluation of iNOS lipoplex-mediated gene transfer, called REGENT-1: Restenosis Gene Therapy Trial. 69 The primary objective of this multicenter, prospective, single-blind, dose escalation study was to obtain safety and tolerability information of iNOS-lipoplex gene therapy for reducing restenosis following coronary angioplasty. As of 2002, 27 patients had been enrolled overseas and the process had been determined to be safe. To date, no results have been published as it appears that this trial lost its funding and closed. On April 5, 2002, a notification was issued that the trial had been closed without enrolling any individuals in the United States. 75
Unfortunately, despite the promising findings shown with NOS therapy, the field of gene therapy has been mottled by two widely known complications. One case occurred as the result of administering a large viral load that led to the death of a patient. 67 In addition, in France, there were at least two cases of malignancy following retroviral gene therapy. 67
Future Directions
As stated earlier, one main limitation of local drug delivery is the finite amount of drug that can be delivered. NOS gene therapy has proved to be able to increase the duration of bioavailability but has its own host of side effects that have caused the field to fall out of favor. Because of these limitations, new materials have been developed that rely on using endogenous S-nitrosothiols that already circulate in our blood as an infinite local source of NO. 58
One of the first studies to describe this was performed by Duan and Lewis.
76
Another example of using endogenous S-nitrosothiols as local NO donors was described by Oh and Meyerhoff. 78 The authors exploited one of the known mechanisms by which S-nitrosothiols release NO, using copper as a catalyst. They developed a biomimetic lipophilic copper complex that is able to reduce S-nitrosothiols and nitrite to NO under physiologic conditions. This complex was doped into polyvinyl chloride and polyurethane films and was shown to catalytically generate NO. The advantage of employing this catalytic surface in vivo is that locally enhanced NO levels are likely to be maintained for extended periods of time by reaction with endogenous S-nitrosothiol compounds that exist in human blood. The authors speculated that this could be used to overcome biocompatibility problems for long-term vascular implants, such as stents and vascular grafts.
Recently,Wu and colleagues attempted to use this same technology when applied to intravascular oxygen sensors. 79 Metallic copper particles were embedded as catalysts into thin polymer coatings on the surface of intravascular electrochemical oxygen-sensing catheters. These catheters were tested in vivo by implanting them into porcine carotid arteries. The NO-releasing catheters exhibited less thrombosis and obtained more accurate measurements compared with control sensors. The authors speculated that because of the improved biocompatibility of these products and their ability to produce NO continuously, this approach could be used with any blood-contacting device.
In the attempt to improve on this technology, Cha and Meyerhoff described the first NO-generating material that uses an immobilized organoselenium moiety as a catalyst for endogenous S-nitrosothiol decomposition. 80 Organoselenium compounds can generate NO from S-nitrosothiols via a catalytic reaction similar to copper. The authors stated that polymers containing immobilized organoselenium species appear to be the most promising as new NO-generating materials for implantation purposes. Yet, at this time, there have been no published studies examining their use to reduce neointimal hyperplasia in animals.
Summary
Atherosclerosis in the form of coronary artery disease and peripheral vascular disease continues to be a major source of morbidity and mortality. Unfortunately, the procedures and materials that are currently used to alleviate these disease states are temporary at best because of the inevitable injury to the native endothelium and the subsequent impairment of NO release. Since the discovery of NO and its role in vascular biology, a main focus in vascular research has been to create novel mechanisms to use NO to combat neointimal hyperplasia. To date, numerous animal studies have restored NO production to the vasculature and have shown that this inhibits neointimal hyperplasia, improves patency rates, and is safe to the animal. Clinical studies using these novel NO-releasing compounds in humans are on the horizon.