
Abstract
Abdominal aortic aneurysm (AAA) is a common and deadly problem. The aortic diameter increases in association with a complex remodeling process that includes changes in the structure and content of key proteins, elastin and collagen. As these changes occur, the tissue mechanical properties also change. The natural history of AAA is progressive enlargement to a point of mechanical tissue failure, typically followed by death. Currently, the marker used to predict the risk of impending rupture is the largest transverse diameter. After reaching a diameter threshold of 5.5 cm, the aneurysm is surgically repaired. This criterion does not consider any patient-specific information or the known heterogeneity of the aneurysm that may, in some cases, lead to rupture before the aneurysm reaches the standard intervention threshold. Conversely, in many patients, continued observation beyond this threshold is safe. Although no medical treatment is yet approved, doxycycline has been shown to greatly reduce aortic aneurysm growth in animal models and has been shown to slow growth in several small clinical trials. Although larger prospective randomized trials are needed, one unknown is what effect doxycycline has on the structural integrity of the aortic wall. That is, does slowed aneurysm growth by doxycycline treatments, in fact, prevent rupture, or does the wall continue to weaken and the aneurysm instead ruptures at a smaller diameter? Research has begun to answer these questions before a large clinical trial begins.
Abdominal aortic aneurysm (AAA) is a common and deadly problem. Aortic aneurysms develop because of weakening of the artery wall, leading to gradual enlargement to a point where the arterial wall tears. The aortic diameter increases in association with a complex remodeling process that includes changes in the structure and content of key proteins, elastin and collagen. As these changes occur, the tissue mechanical properties also change. The natural history of AAA is progressive enlargement to a point of mechanical tissue failure, typically followed by death. At present, we do not have a way to determine the point at which aneurysm rupture will occur. Currently, the marker used to predict the risk of impending rupture is the largest transverse diameter. After an aneurysm reaches the surgical threshold, it is repaired. This criterion does not consider any patient-specific information or the known heterogeneity of the aneurysm that may, in some cases, lead to rupture before the aneurysm reaches the standard intervention threshold.
AAA affects 2 to 9% of the elderly in the US population 1 and results in at least 15,000 deaths per year from rupture. 2 This is likely a conservative estimate of AAA-associated deaths because the true cause of sudden death is rarely determined in elderly patients and aneurysm rupture will undoubtedly be ascribed to coexistent coronary artery disease in some cases. 3–5 More than 40,000 surgical procedures on AAA are performed annually in the United States, the vast majority being done to prevent rupture. 2 There is evidence that the general prevalence of AAAs is steadily increasing, both in the United States and other industrial nations. 6 Even by conservative estimates, extrapolation of these figures to US census data indicates that aneurysm disease currently affects at least 1.7 million individuals. One estimate is that there are 360,000 undetected small AAAs in the United States. 7 Moreover, the incidence of AAAs can be expected to exceed 3 million by 2025 as 70 million “baby boomers” will have reached their seventh decade of life. The current demographics indicate that 29% of the entire population of the United States is now between the ages of 40 and 60 years. During the next 20 years, this group will move into the “at risk” population for aortic aneurysm disease. Recognizing this epidemic, the Centers for Medicare and Medicaid Services have made reimbursement available for aneurysm screening for men over the age of 65 years who have ever smoked. Thus, the detection of unrecognized aortic aneurysms will become increasingly common.
Surgical intervention involves small but significant risk, and the procedure is costly. Conversely, monitoring aneurysm growth with semiannual ultrasonography or computed tomography (CT) can be unsettling for patients. Most aneurysms at the time of detection are below the threshold that would warrant immediate repair. The large number of patients under observation with small aneurysms presents a great opportunity to attempt to alter the natural progression of the disease process. With advances in our understanding of the underlying disease process, pharmacologic therapy to slow, stop, or possibly even induce regression of existing aneurysm has become feasible. Currently, the only proven treatment for AAA is surgical intervention. Control of hypertension and cessation of tobacco use may have a small impact on aneurysm expansion. 8–14 There is no medically approved treatment to prevent aortic aneurysm expansion. Often beta-blocking agents are used to decrease blood pressure in the hope of reducing the rate of dilatation. 15,16 However, two prospective studies failed to show a reduction in the expansion rate. 17,18
Surgical repair is effective in preventing aneurysm rupture; however, for small aneurysms, the risk associated with repair exceeds the risk of rupture. Therefore, once diagnosed, the current practice is to follow these aneurysms at 6- to 12-month intervals with ultrasonography or CT until the diameter exceeds 5.0 cm in women and 5.5 cm in men. 19 The risk of rupture for aneurysms smaller than 4 cm is low, 20,21 but in some studies, 10 to 24% of the ruptured aneurysms had maximum diameters of 5 cm or smaller. 22,23 This suggests that the critical aneurysm size of 5.5 cm may not be the best or only predictor of rupture.
Although we can reassure these patients that the risk of rupture is extremely low during this period of observation, many find this approach unsettling. A number of studies have, in fact, demonstrated that there is a significant decrease in an individual's perception of his or her health when made aware of the presence of an aneurysm, which will be observed. 24 This may manifest in a number of ways, such as anxiety or depression, resulting in a decrease in quality of life. This “watchful waiting” observational approach is particularly unsettling given that the biologic factors influencing aneurysm expansion are incompletely understood and no treatment can be offered to alter the natural history of progression. This is a very difficult dilemma and explains why some small aneurysms are now being treated with less invasive but extremely costly ($20–25,000/procedure) endografts. 25 These procedures are still risky in some patients. In fact, recent studies report a mortality rate of > 5% after elective endograft repair in high-risk patients. 26,27 Further, two clinical trials have shown that early, prophylactic elective surgery does not improve 5-year survival among patients with a small AAA (4.0–5.5 cm). 28,29 These studies show that there was no evidence that the number of life-years gained was improved significantly by a policy of early surgery. Interestingly, there are also data demonstrating that the majority of patients will tolerate expansion to 6 cm without rupture. 22 Thus, using diameter alone, without patient-specific information, a small number of aneurysms are not repaired in time and a large number are being repaired prematurely.
With the approved screening strategy for Medicare patients, we will presumably begin to identify a larger proportion of those 360,000 undiagnosed small AAAs. Broadening the indications for endovascular repair to include small AAA would be cost-prohibitive unless the cost of the devices is drastically reduced.or there were an accepted means of stratification that allowed for repair of selected small AAAs. Therefore, considering the large numbers of affected patients, the surgical costs of intervention, and the risk of surgery, an alternative and more attractive approach would be medical treatment to prevent the progression of aortic aneurysms.
Potential Treatment Options
Remarkable advances in our understanding of AAA pathophysiology have occurred in the past several years. The critical role of a family of matrix degrading enzymes (matrix metalloproteinases [MMPs]) has been elucidated through animal models that closely mimic human disease. MMP-2 and MMP-9 are particularly important local factors in aneurysm formation 30,31 ; MMP-9 serves as a systemic serum marker for the disease. 32,33 MMPs preferentially degrade elastin and fibrillar collagen. Invading inflammatory cells are believed to be directly responsible for MMP-9 and indirectly for MMP-2 by stimulating their production in the resident smooth muscle cells and fibroblasts. Blocking MMP production is one of the most obvious approaches to the medical treatment of AAA.
Tetracycline antibiotics have been found to be active against MMPs 34 and have been successfully used to treat several conditions associated with elevated MMP activity and connective tissue destruction. 35 These studies showed that tetracyclines have substantial metalloproteinase-inhibiting effects. Subsequent work since the initial discovery has shown that this effect is not related to the antimicrobial activity. 36 Doxycycline was shown to inhibit aneurysm formation in a rodent model of aneurysms in 1996. 37 Subsequent work has shown it to be effective in essentially every model of aortic aneurysm in which it has been tested. Work from our laboratory has shown that doxycycline at standard therapeutic serum concentrations inhibits MMP-2 expression from cultured human aortic smooth muscle cell and AAA tissue explants. 38 The plasma levels required to achieve inhibition are similar to those that can be expected in patients taking standard doses of doxycycline. 39 Furthermore, a short course of preoperative doxycycline has been shown to inhibit the MMP content of the aneurysmal aorta. 40 There has been a single small randomized trial assessing the ability of doxycycline to inhibit the growth of aortic aneurysms. At 6 and 12 months, there was no growth noted in doxycycline-treated patients. 41 A recent study showed that doxycycline, at pharmacologically achievable nontoxic doses, inhibited transforming growth factor β (TGF-β)-induced MMP-9 production and activity through the Smad and MAPK signaling pathways. 42 These findings support the idea that doxycycline may treat diseases in which TGF-β plays a role in pathogenesis by causing a secondary increase in MMPs, such as occurs in Marfan syndrome. Taken together, these data suggest that doxycycline could be an effective therapy for treating aneurysms.
Treatment Effects
The impact of growth inhibition on the progression of aneurysm expansion is shown in Figure 1, considering three scenarios: 30%, 40%, or 50% inhibition of growth rate. Since most patients with AAA are in their seventh or eighth decade, a significant reduction in the aneurysm growth rate may alleviate the need for repair. This is especially true for the high-risk population, in which all cause mortality is as high as 8% per year. 43 Although regression should be the ultimate goal, inhibiting progression of small aneurysms may be a more achievable goal in the short term.
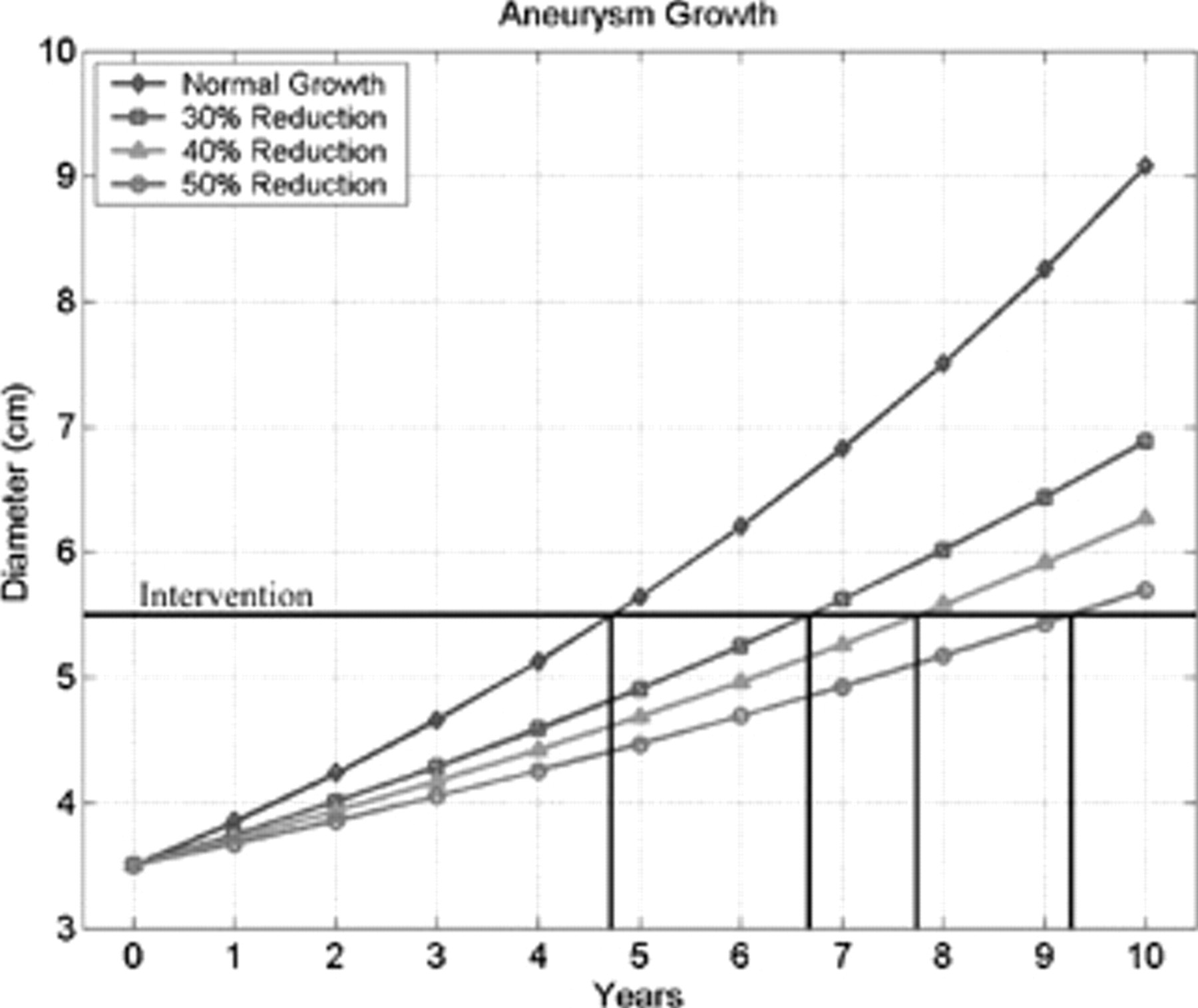
Impact of inhibiting aneurysm expansion by 30%, 40%, and 50% as shown. This figure is on the basis of a normal expansion rate of 10% per year.
Inhibition of aneurysm growth is essential to preventing rupture. As an aneurysm grows, the transverse diameter increases. Increases in diameter result in increases in circumferential and longitudinal forces and stresses in the tissue. By maintaining a smaller diameter, the resultant forces and stresses in the tissue wall are kept lower. This helps prevent the wall stresses from exceeding the failure strength limit of the wall.
Future Research Areas
As doxycycline and other tetracyclines are studied for AAA treatment, research needs to remain focused on both slowing aneurysm growth and maintaining the aortic wall integrity. Slowed growth will help maintain lower levels of mechanical stress in the wall, whereas a properly maintained wall structure will help retain compliance. Maintaining or improving compliance of the aorta will also reduce wall stress and probably increased strength.
Although larger prospective randomized trials are needed, two unanswered questions remain. What effect does doxycycline have on the aortic wall structure, and will doxycycline be effective in developed, preexisting aneurysms? That is, can doxycycline slow an established aneurysm's growth, and does this, in fact, prevent rupture, or does the wall continue to weaken so that the aneurysm may rupture at a smaller diameter? These important questions need to be answered before a large clinical trial begins.
We have begun to test the effects of doxycycline on wall strength, compliance, and structural integrity in a murine model, using a series of pressure-diameter experiments and histologic studies. The results indicate that a physical test measurement may be a good method by which to screen drugs for positive or stabilizing effects on the aorta. Looking only at the aneurysm growth rate may be too one-dimensional. This approach would help predict the long-term safety and efficacy of the treatment.