
Abstract
Recent trends toward less invasive technologies for treating varicose veins have led to expanding interest in transilluminated powered phlebectomy. Although initial experience with transilluminated powered phlebectomy was variable, with the newer-generation system and modification of technique that allow for slower oscillation speed, higher suction, and extensive tumescence irrigation and drainage, these previous problems have been mostly eliminated. The following report reviews current instrumentation, operative technique, and reported outcomes for transilluminated powered phlebectomy.
Treatment of varicose vein tributaries has traditionally involved a variety of phlebectomy techniques, which have fallen under the term ambulatory phlebectomy but include various descriptors, such as excisional phlebectomy, stab avulsion phlebectomy, hook phlebectomy, and micropuncture phlebectomy. Although the terminology can be confusing, the basic technique is the same, involving multiple small incisions for direct removal of varicosities. With advances in tumescence anesthesia, these phlebectomy techniques are able to be performed in the outpatient setting; are associated with low complications, high patient satisfaction, and excellent cosmesis; and have become a safe and effective method for varicose vein removal. There are some limitations, however, including the need for multiple incisions, poor visualization, incomplete resection, and technical challenges for patients with extensive varicosities.
Advances in the past decade toward minimally invasive technologies have permeated all aspects of surgery. With US Food and Drug Administration (FDA) approval of transilluminated powered phlebectomy (TPP) (TriVex, Smith & Nephew Endoscopy, Andover, MA) in 1999 came the expansion of less invasive operative options for varicose veins. Although the initial experience with TPP was variable, with the newer-generation system and modification of technique, these problems have been mostly eliminated. The following report reviews current instrumentation, operative technique, and reported outcomes for TPP.
Operative Technique
Instrumentation
Current instrumentation for TPP available through Smith & Nephew Endoscopy represents the second generation of the device and became available in 2004 with several upgrades from the original configuration (Figure 1). The TriVex System Control Unit is the central power unit with controls for xenon light source intensity, an irrigation pump, and resection oscillation speeds. The TriVex Illuminator connects to the control unit with a fiber-optic cable and provides high-intensity light for transillumination and tumescence irrigation control. The TriVex Resector Handpiece has both 4.5 and 5.5 mm resector blade options, control of oscillation direction and rate, and connectors for suction tubing.
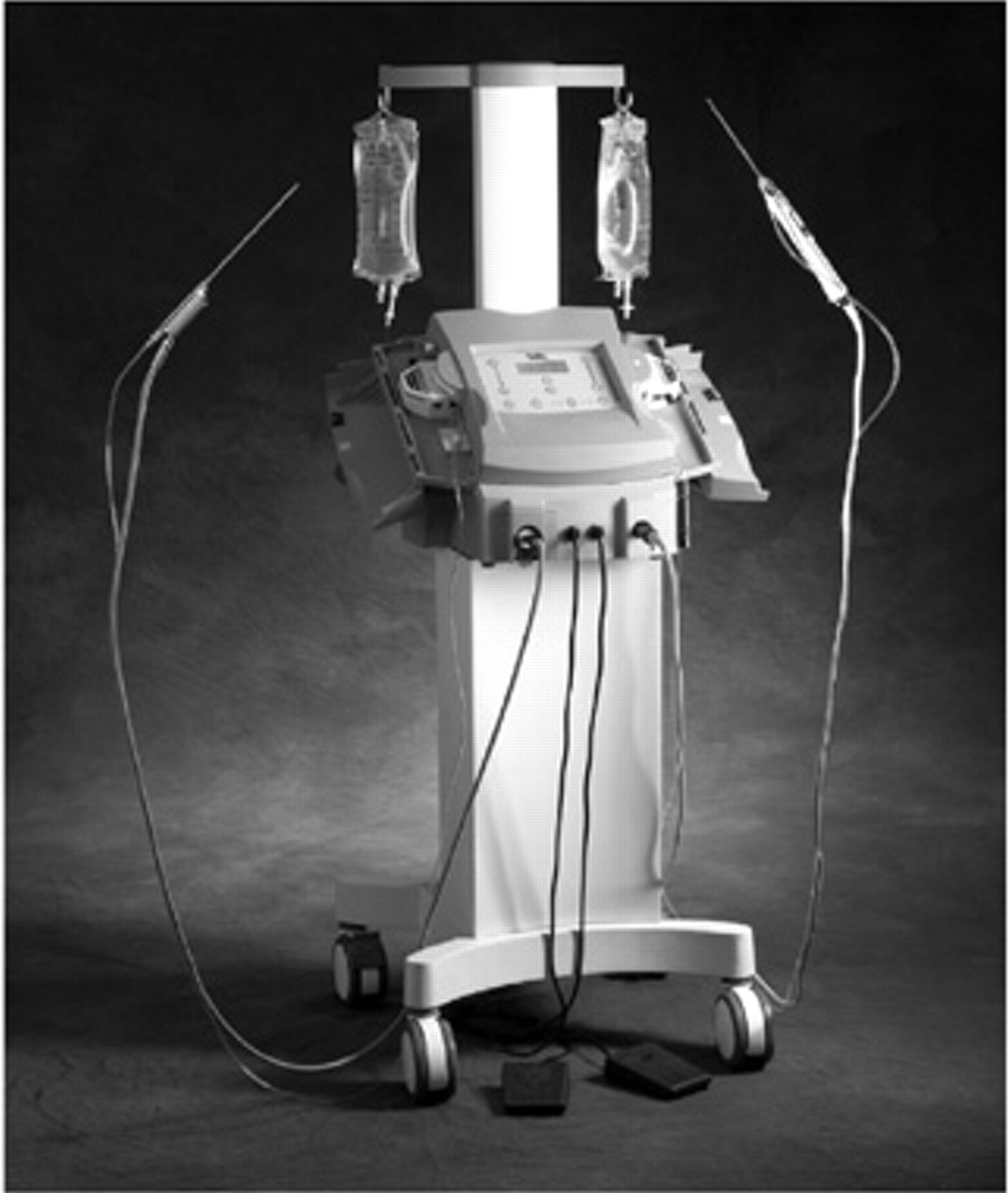
The new-generation TriVex System Control Unit with connected TriVex Illuminator and TriVex Resector Handpiece used for transilluminated powered phlebectomy as available from Smith & Nephew Endoscopy (Andover, MA). Reproduced with permission from Smith & Nephew Endoscopy.
Patient Preparation
Preoperative marking is performed with the patient standing to maximize varicose vein dilation. Unlike standard phlebectomy, which requires direct marking over the varicosity, for TPP, an outline is made around the area of varicosities to avoid obscuring the vein with the skin mark. General, epidural, or spinal anesthesia can be used depending on patient preference. Local tumescence anesthesia and conscious sedation are options for limited varicosities in selected patients. The patient is positioned supine with the lower extremity elevated 30° (Figure 2). Standard sterile preparation and drape are performed with care to avoid removal of preoperative marks. If other procedures such as saphenous stripping or endovenous ablation are required, these are performed first. Especially in regard to endovenous ablation, use of tumescence with TPP can cause problems with ultrasound visualization needed for endovenous ablation and should be delayed until the entire endovenous ablation procedure has been completed. Incisions used for these other procedures can be subsequently used for TPP when appropriate based on preoperative marking.
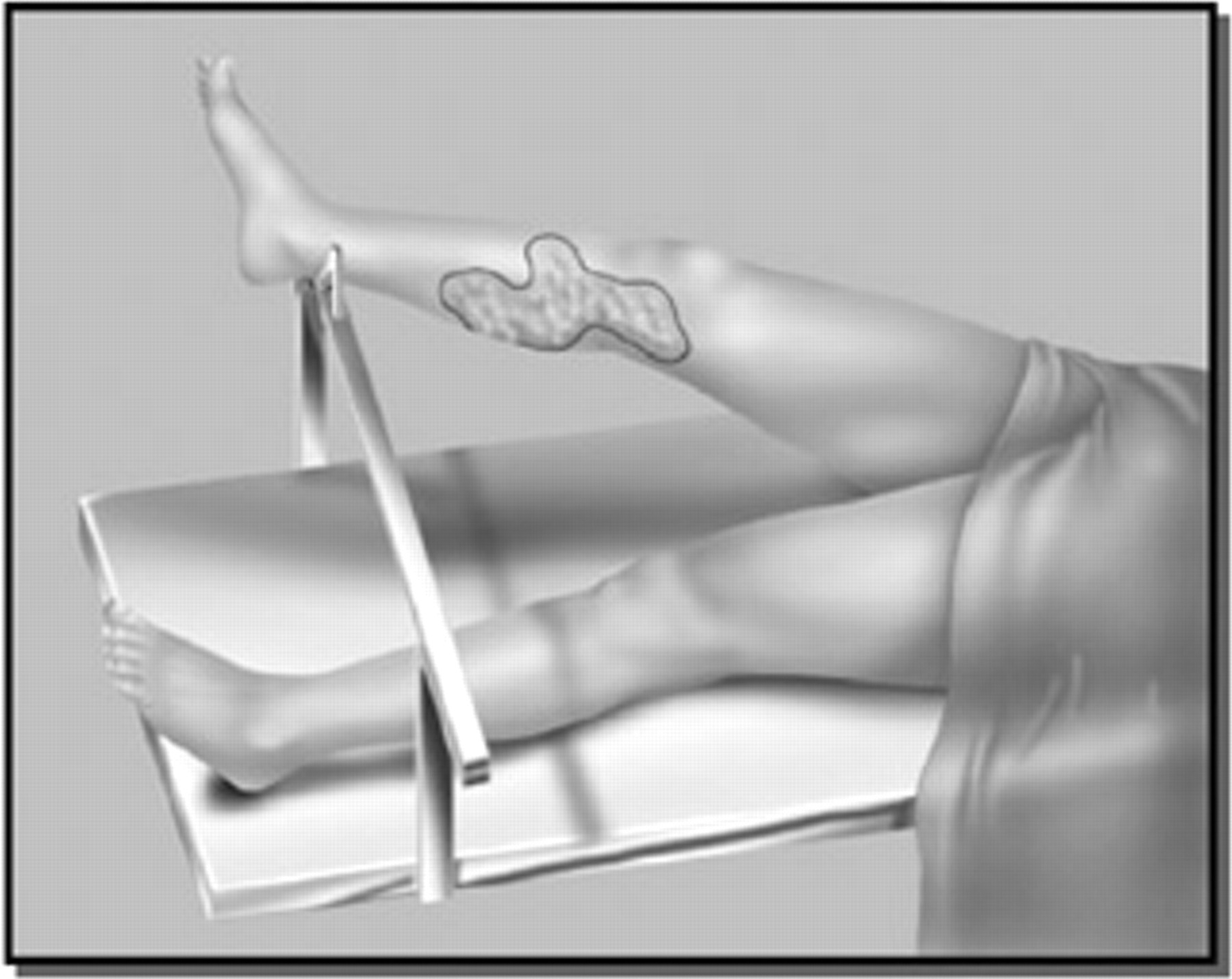
Preprocedure marking outlining the area of varicose veins undergoing resection using a transilluminated powered phlebectomy technique. Reproduced with permission from Smith & Nephew Endoscopy.
Tumescence
Tumescent solution is prepared with 50 mL of 1% xylocaine and 1 to 2 mL of 1:1,000 epinephrine diluted in 1,000 mL 0.9% normal saline. The original device configuration required a separate irrigation pump, but with the second-generation system, the irrigation pump is incorporated into the TriVex System Control Unit. Adjustment can be made in the intensity of pump pressure generated, but higher settings are more commonly used.
Incisions
Incisions should be strategically planned to minimize the number of incisions and to use the maximum length of the TriVex Resector Handpiece. Incisions can also be interchanged between instruments to allow extension of the resection range. The position of the incisions should also be oriented so that the instruments approach the intended area of resection at 180° if possible to maximize the area of resection, although at times the angle of instrumentation will decrease to accommodate the best position and to avoid limitations while approaching knee or ankle varicosities. Incisions are 2 to 3 mm in length and are vertically oriented in the thigh and calf and transversely at the knee level following natural Langer skin lines for the most cosmetically appealing results. Resection of varicosities across the foot is avoided.
Visualization: Resection
The TriVex Illuminator is placed initially, and first-stage tumescence is performed (Figure 3A). The illuminator is placed a few millimeters deeper than the target varicosity, and tumescence solution is infiltrated into the area along the course of the vein. With adequate infiltration, visualization with transillumination effect will improve, but overinfiltration should be avoided to prevent compression of the vein and loss of visualization. Tumescence also allows for hydrodissection of the varicosities, which will assist with resection. Through the counter incision, the TriVex Resector Handpiece is placed, and the tip is directed to just underneath the varicosity (Figure 3B). Resection along the longitudinal axis of the vein is preferred when possible to maximize the amount of vein resected with a single pass. As the angle to the vein becomes more acute, multiple passes to reposition the tip of the resector will be required for complete removal. Although the earlier technique with the first-generation system included higher oscillation frequencies (800–1,200 rpm), modification with the newer-generation system allows for lower oscillation frequency (300–500 rpm). With the lower speed and a rapid on-off pulsing, limited dissection with the resector is employed to gently loosen the vein from supporting tissue, with most of the resection then accomplished by the high suction. During resection, skin is held taut to facilitate resection and prevent skin penetration. Additional tumescence is infiltrated as resection proceeds to flush any residual vein tissue and blood into the suction and to increase pressure along the resected vein to provide a tamponade effect (Figure 3C). Successful resection of the vein will be confirmed with blanching along the vein tract. The TriVex Illuminator and TriVex Resector Handpiece are then exchanged through respective incisions. After completing resection in one area, attention is then directed to the next segment of the leg.
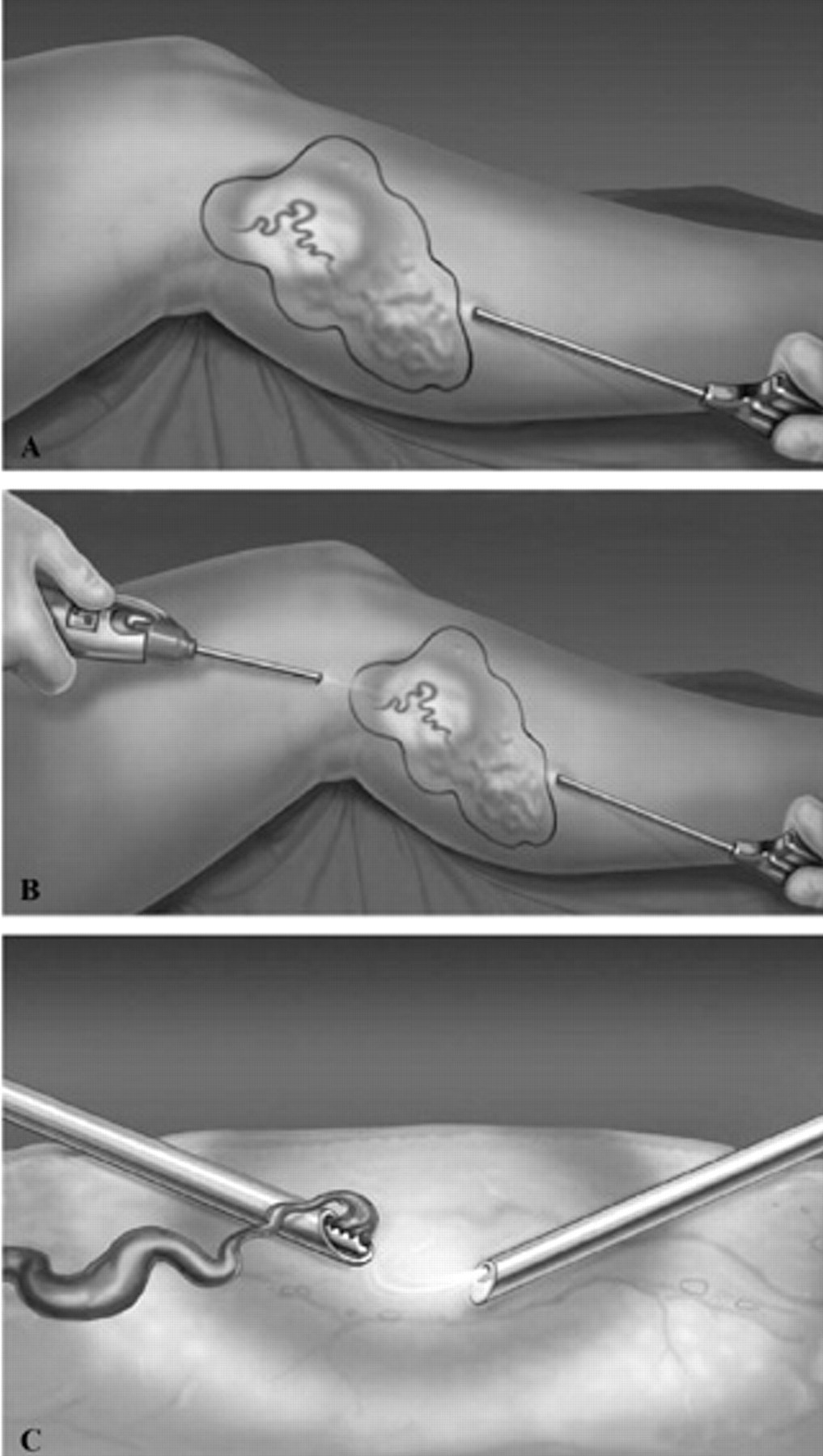
A, Placement of the TriVex Illuminator for primary tumescence irrigation and transillumination showing visualization of varicose vein. B, Placement of the TriVex Resector Handpiece through counterincision with the tip directed to the varicose vein for resection. C, Resection of varicose vein by the oscillating tip of the TriVex Resector Handpiece under direct visualization facilitated by the TriVex Illuminator with additional tumescence irrigation along the vein tract during resection. Reproduced with permission from Smith & Nephew Endoscopy.
Irrigation: Drainage
Modification of technique with the newer-generation device also includes a more extensive secondary tumescence phase through additional drainage incisions made using a 1.5 mm dermal punch biopsy (Figure 4A). Punch holes can be made either before resection along the course of the vein or after resection in areas where blood pools subcutaneously as visualized with transillumination. Evacuation of any hematoma is facilitated with manual compression along the vein tract. Copious irrigation is performed through the dermal punch incisions using the TriVex Illuminator until drainage is clear (Figure 4B). After resection is completed, tertiary tumescence is performed in the subdermal plane using a spinal needle connected to the pressure tubing to create a peau d'orange effect in the skin (Figure 4C). This allows for additional irrigation and drainage, provides increased subdermal–subcutaneous pressure to decrease the potential for delayed hematoma, and extends the anesthetic effect of the tumescence. Only passive drainage of irrigation fluid is recommended at this stage.
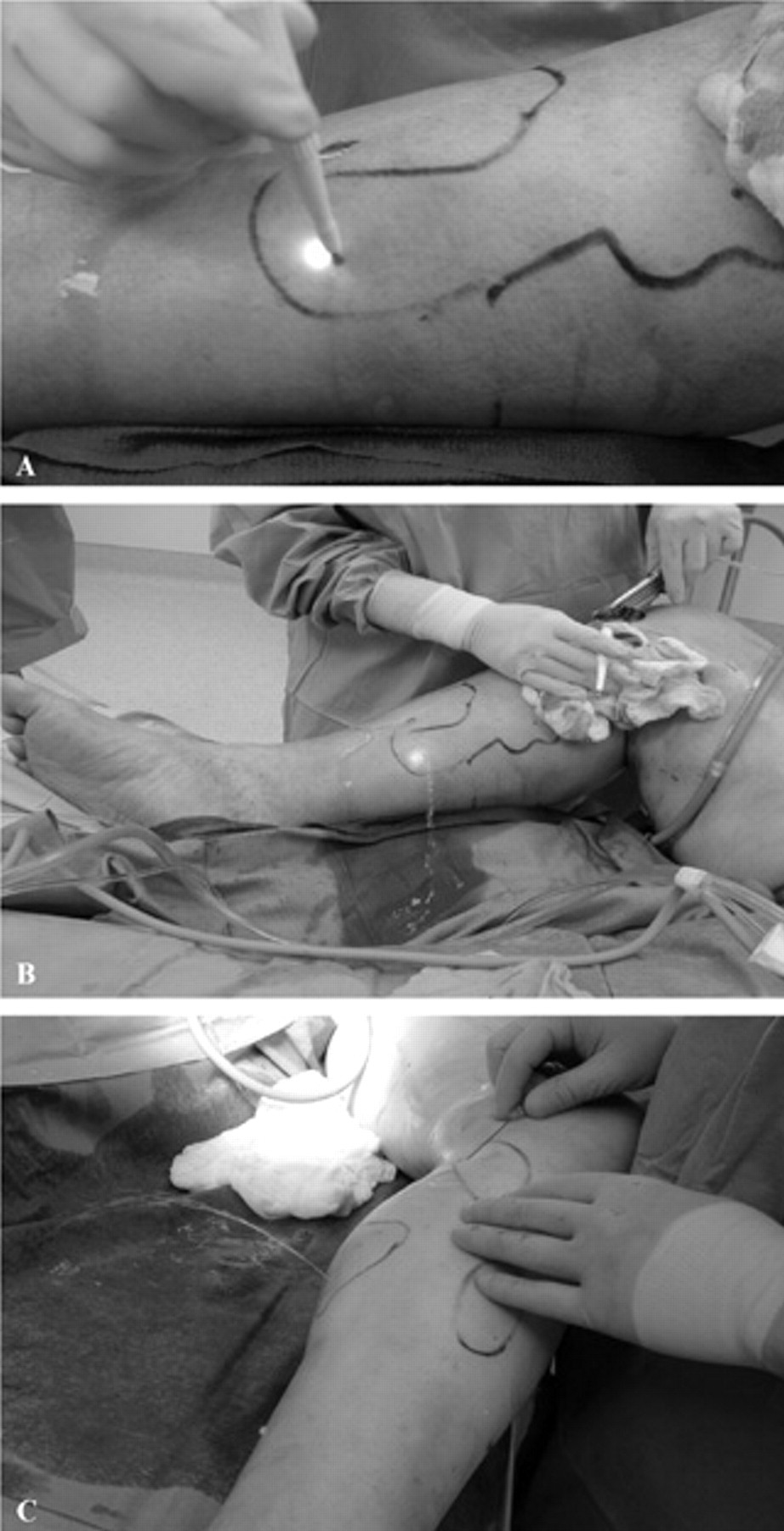
A, Additional dermal punch biopsy drainage hole for secondary tumescence and irrigation of residual blood and vein tissue fragments. B, Copious irrigation is performed using the TriVex Illuminator until drainage is clear. Tertiary tumescence performed using a spinal needle in the subdermal plane creating a peau d'orange effect in the skin. Reproduced with permission from Smith & Nephew Endoscopy.
Dressing: Postoperative Protocol
Incisions are too small for suture closure and are covered with benzoin and Steri-Strips. A layered compression dressing (ABD pads, Webril, Kerlix, Ace Wrap, Coban) is applied from the base of the toes to high up on the thigh. Some delayed passive drainage and staining of the dressing should be expected. Although ambulation is encouraged, elevation of the extremity should be recommended during periods of rest in the initial few postoperative days. Nonsteroidal anti-inflammatory medications are avoided in the first week to avoid increased bruising and bleeding risk. Compression is continued in the first week with an Ace Wrap with transition to graduated compression stockings. Compression is continued for an additional 1 to 2 months. Postoperative visits are usually within 1 week and between 4 and 8 weeks.
Discussion
Recent trends toward less invasive procedures for treating varicose veins have led to expanding interest in ambulatory phlebectomy, ultrasound-guided sclerotherapy, and TPP, each of which has certain advantages and disadvantages. Although there is some debate regarding what is considered less invasive, the distinction is usually based on the size and number of required incisions. In this regard, much like endovenous ablation is less invasive than saphenous ligation and stripping, TPP is less invasive than ambulatory phlebectomy, each of which requires fewer incisions than its traditional counterpart. However, with expansion of outpatient venous techniques using smaller hook phlebectomy instrumentation and sclerotherapy using fine needles, the concept of less invasive is relative. Current techniques for ambulatory phlebectomy using small incisions and hook dissectors are similar to those originally described by Muller in 1966 1 and remain the standard operative approach for varicose veins. Additional modifications using extended tumescence anesthesia have allowed for expansion of these procedures in the outpatient setting, with excellent outcomes and low complication rates. However, for extensive varicose veins, ambulatory phlebectomy can be time consuming and tedious to perform, has poor visualization, and requires multiple incisions, all of which can lead to incomplete resection and diminished satisfactory results. More recently, ultrasound-guided sclerotherapy has also gained favor. With the use of fine needles, incisions are avoided. Yet limitations include the need for higher concentration of sclerosant, decreased effectiveness for larger veins, and potential for leakage of sclerosant into the deep venous system. Although foam sclerotherapy may hold future promise, foam reconstitution of sclerosant agents is not currently FDA approved, with evidence-based outcomes lacking and limited published reports suggesting some problems, especially with venous thrombophlebitis and generalized somatic complaints. 2–4
The use of transillumination for mapping of varicose veins prior to ambulatory phlebectomy was described in 1998 by Weiss and Goldman. 5 Spitz and colleagues reported combining transillumination with pressurized tumescence irrigation and powered resection for treatment of varicose veins. 6 Original device configuration had been adapted from endoscopic instrumentation used for arthroscopy, with modifications to make vein resection less traumatic. FDA approval for the first generation TriVex system and instrumentation occurred in 1999. Initial reports confirmed advantages, including improved visualization, fewer incisions, and less operative time, with outcomes being safe and efficacious. 6–9
Four studies have directly compared TPP with conventional varicose vein surgery: two prospective nonrandomized studies and two randomized controlled trials. Whereas Spitz and colleagues, comparing 59 TPP procedures with 114 historical controls of hook phlebectomy, showed decreased operating times, fewer incisions, and acceptable postoperative pain levels and complication rates, 6 Scavee and colleagues, in a nonrandom comparison of 40 patients undergoing TPP and 40 patients undergoing hook phlebectomy, similarily showed fewer incisions and no difference in pain, cosmetic results, complications, and residual varices but longer operative time and more hematomas. 9 In a recent prospective randomized study by Aremu and colleagues, 188 limbs with varicose veins were randomized to conventional stab phlebectomy (n = 100) or TPP (n = 88), the latter demonstrating a need for significantly fewer incisions (n = 5) than conventional stab phlebectomy cases (n = 29) (p < .0001); a trend for decreased operative time for extensive varicosities; similar outcomes for pain, bruising, cellulitis, numbness, nerve injury, residual veins, and cosmetic score; and overall satisfaction between the two procedures. 10 The authors concluded that TPP compared appropriately after a learning curve with conventional methods in complications and recurrence and was safe and effective for treatment of varicose veins. Chetter and colleagues also conducted a randomized clinical trial evaluating perioperative variables and early patient-reported subjective outcomes after TPP (n = 29) compared with multiple stab incision phlebectomy (n = 33). 11 Although the total operating times were similar in both groups, the TPP group had a reduction in the number of skin incisions. The authors also reported that although the incidence of hematoma in this study was not increased by the use of TPP, there was a higher incidence of bruising, saphenous neuropathy, and persistent pain and reduced early quality of life parameters in the TPP group, suggesting that the full benefit of the procedure may not be realized in the early postoperative period.
Scavee conducted a review of the literature to examine whether TPP demonstrated any benefit, other than reducing the number of incisions, when compared with standard varicose vein treatment (ambulatory phlebectomy), identifying nine trials (the four studies comparing TPP with conventional surgery discussed above and five other prospective observational studies). 12 Complications following TPP varied considerably and consisted primarily of ecchymosis and/or hematoma formation (4.9–95%), paresthesias or nerve injury (9.5–39%), skin perforation (1.2–5%), superficial phlebitis (2.4–13%), swelling (5–17.5%), hyperpigmentation (1.2–3.3%, and deep venous thrombosis (< 1%). Although most studies reported fewer incisions for TPP compared with conventional surgery, differences in operating time varied. With regard to cosmetic scores, outcomes were similar for both groups, although some authors reported more favorable results with conventional surgery. Residual or recurrent varicose veins varied between 9.1 and 21.2 %. Although overall patient satisfaction scores were not statistically significant, the scores had a tendency to be lower for TPP compared with conventional surgery. Conclusion from this review was that no data clearly proved any significant statistical advantage of TPP over conventional treatment, except for the number of incisions, with further randomized trials needed to determine any additional potential benefits of the procedure.
Currently, TPP is most efficacious for extensive varicose veins as the improved visualization allows for more complete resection with fewer incisions. However, for patients with less extensive varicosities, the margin of benefit of TPP decreases when compared with ambulatory phlebectomy. This difference is also heightened by the need for general or regional anesthesia when performing TPP, which limits its use to an operating room setting. Use of TPP with local tumescence anesthesia alone was recently reported, with periprocedure pain noted to be minimal and acceptable in selected patients. 13 As experience grows using local tumescence alone, expansion of TPP more into the outpatient clinic setting may be on the horizon.
The problem with most of the published literature cited above is that the operative technique included the early-generation TriVex system and/or initial technical recommendations for higher oscillation frequencies (800–1,200 rpm) and primary and secondary tumescence stages only. In an effort to improve these outcomes, the second-generation system was introduced in 2004 with additional technical modifications incorporating lower oscillation frequency (300–500 rpm), dermal punch drainage technique, secondary tumescence with extensive flushing of residual hematoma and residual venous tissue fragments, and the addition of a tertiary tumescence stage in the subdermal plane. The practice pattern at our academic medical center was reviewed in regard to transition from combined open to less invasive operative vein approaches over an 8-year period. 14 In the early portion of the study period, our combined operative approach was exclusively saphenous vein stripping with stab avulsion phlebectomy. With the introduction at our institution of TPP in 2001 and endovenous ablation in 2003, there had been a complete frame shift by the end of the study period toward a combined less invasive approach with a time-dependent expansion of vein operative clinical volume (1998–2005: 72 limbs in 59 patients treated with combined stripping and phlebectomy; 2001–2005: 92 limbs in 81 patients with combined stripping and TPP; and 2003–2005: 99 limbs in 76 patients with combined endovenous ablation and TPP). The overall distribution of complications remained unchanged between the early (stripping-phlebectomy) and later (endovenous ablation–TPP) portions of the study, although there was an increase in complications during the transition phase (stripping-TPP) related mostly to the increased hematomas with the earlier TPP techniques. With the described modifications of TPP, problems with hematoma after endovenous ablation–TPP decreased to levels comparable to stripping and phlebectomy (stripping-phlebectomy, 5.6%; stripping-TPP, 16.3% (p < .05); endovenous ablation–TPP, 6.9%). Furthermore, when the individual techniques of endovenous ablation and TPP were evaluated separately, the outcomes reported were not different for those published individually for each technique, respectively. In our experience, with the shift of combined operative vein approaches for concomitant saphenous vein insufficiency and secondary varicosities toward less invasive techniques, there had been an associated shift in the distribution of postoperative problems, although the overall complication rate had remained unchanged. We concluded that although combined endovenous ablation–TPP offers some advantage of “less” invasiveness, this perceived benefit should be balanced against the unchanged overall risk over traditional operative approaches. Although recent reports have suggested regression of varicose veins after saphenous endovenous ablation alone, 15 given the extent of resection usually reserved for TPP and the need for general or regional anesthesia, a combined approach is usually recommended.
In conclusion, although there are no published data clearly showing any significant statistical advantage of TPP over conventional treatment except for the number of incisions, most of the published literature represents an earlier-generation system and techniques. With a newer-generation device, smaller instrumentation, and modification of technique that allow for slower oscillation speed, higher suction, and extensive tumescence irrigation and drainage, the technique of TPP has become less traumatic, which should impart decreased potential for complications and improved outcomes over those previously reported. However, until additional randomized trials evaluating these newer techniques are published, any additional potential benefits of the procedure have yet to be determined.