
Abstract
Spontaneous thrombosis of the axillary and subclavian venous segments in young, healthy adults (effort thrombosis or Paget-Schroetter syndrome) is a rare but potentially disabling affliction. The diagnosis should be suspected in any young patient presenting with unilateral arm swelling. Typically, the dominant arm is affected, and frequent, repetitive arm use is a common component of the patients' history. Although the diagnosis can often be confirmed with a venous duplex evaluation, the central location of the venous abnormality occasionally mandates cross-sectional imaging or contrast venography to confirm the diagnosis. The underlying pathophysiology of this disorder is felt to be repetitive venous trauma owing to arm motion in the narrow anatomic space between the clavicle and first rib. The treatment of Paget-Schroetter syndrome is controversial and varies according to individual, institutional, and regional preferences. In general, the trend is toward more aggressive endovascular treatment. Prompt anticoagulation is generally accepted as the minimal treatment offered. Catheter-directed thrombolysis has also acquired a prominent role in reestablishing venous patency. The importance of relieving the anatomic compression of the subclavian vein by first rib resection remains controversial, with some experts advocating surgical intervention in all affected patients, whereas others perform this procedure selectively in cases of persistent venous stenosis or ongoing symptoms. Angioplasty with or without stenting is generally discouraged in the absence of anatomic decompression but may play an adjunctive role in patients undergoing first rib resection.
Keywords
Deep venous thrombosis (DVT) of the axillary and subclavian veins is rare in comparison with more frequently diagnosed lower extremity DVT, representing approximately 4% of all episodes of venous thrombosis. 1,2 Although the majority of upper extremity DVT is secondary, primarily from catheter-related causes, primary, idiopathic upper extremity DVT, alternately known as effort thrombosis or Paget-Schroetter syndrome, is increasingly recognized, particularly in the young, healthy, athletic patient population. There is no gender preponderance, although the dominant extremity is involved in 70% of patients. 3 The treatment of axillary-subclavian venous thrombosis (ASVT) is an area of ongoing controversy; however, endovascular treatment is increasingly recognized as a critical component of optimal therapy.
Diagnosis
The initial diagnosis of upper extremity DVT is suggested by physical examination. Acute unilateral arm pain, swelling, discoloration, and venous distention of the extremity or anterior chest wall are suggestive of upper extremity DVT but are nonspecific.
The diagnosis of upper extremity DVT is frequently made by venous duplex evaluation, which is the screening method of choice for this disorder. In randomized prospective trials, duplex ultrasonography has been shown to be effective in diagnosing upper extremity DVT with a sensitivity of 78 to 100% and a specificity of 82 to 100%. 4 One of the potential shortcomings of venous duplex evaluations is the inability to adequately visualize the central portions of the subclavian veins and innominate veins. Additionally, differentiating a central vein from a large collateral can be difficult with duplex scanning. For this reason, contrast or magnetic resonance venography is indicated in situations in which the diagnosis is suspected but unclear. Contrast venography has the additional benefit of being combined with endovascular treatment of Paget-Schroetter syndrome, as is discussed in the following section.
Treatment
Anticoagulation
Considerable controversy remains over optimal management of Paget-Schroetter syndrome. No level 1 data exist regarding optimal management of this disorder; however, endovascular management is increasingly gaining in popularity, with numerous single-center trials demonstrating its effectiveness.
Regardless of the treatment chosen, anticoagulation is generally considered the hallmark of therapy. Anticoagulation is pursued primarily for functional recovery rather than risk of pulmonary embolism. Long-term functional outcomes are significantly improved in patients who are anticoagulated versus those who are not. In a large meta-analysis, residual symptoms were present in 36% of patients who were anticoagulated versus 64% in those who were not. 2,5 The risk of pulmonary embolism in patients with upper extremity DVT appears to be less than in those with lower extremity DVT. Most cases of pulmonary embolism in patients with upper extremity DVT occur in patients with additional comorbidities, such as catheter-associated DVT or malignancy. Pulmonary embolism is rare as a consequence of idiopathic primary upper extremity DVT. 6
Anticoagulation alone has fallen out of favor as more aggressive treatment options have emerged; however, some support for anticoagulation alone still exists, particularly in the European literature. Heron and colleagues from Paris reported 54 patients treated with anticoagulation alone with a mean follow-up of 5 years. 7 Follow-up by ultrasonography demonstrated normal flow in 41%, moderate obstruction in 37%, and severe obstruction or occlusion in 22% of patients. Forty-six percent of patients reported no or negligible symptoms, 41% mild or moderate symptoms, and only 7% severe or intolerable symptoms during follow-up. Based on these data, the authors advocated anticoagulation alone as the standard therapy for ASVT, citing a lack of level 1 data to support a more aggressive approach.
Likewise, Sabeti and colleagues from Vienna retrospectively evaluated 95 consecutive patients with ASVT treated either with anticoagulation plus thrombolysis or anticoagulation alone. 8 Patients undergoing thrombolytic therapy had a significantly increased rate of venous recanalization compared with those undergoing anticoagulation alone (88% technical success rate). After a median follow-up of 40 months, patients who underwent thrombolysis had a 60% adjusted reduced risk for subclavian vein thrombosis; however, hazard ratios for symptomatic upper extremity post-thrombotic syndrome were similar. Periprocedural bleeding complications occurred in 21% of patients treated with thrombolysis versus 0% in patients treated with anticoagulation alone. These findings led the authors to conclude that a conservative approach to ASVT may be favorable.
Thrombolysis
There is a growing body of literature on the successful use of thrombolytic therapy in the management of ASVT, and this is considered by many to be the minimal standard of care. Catheter-directed thrombolysis has supplanted surgical thrombectomy and systemic thrombolysis as the preferred method of reestablishing venous patency. Catheter-directed thrombolytic techniques are designed to deliver thrombolytic agents directly into the area of thrombus using a variety of multisidehole infusion catheters and infusion guidewires. Access is typically achieved through sheath placement in the ipsilateral basilic or brachial vein, although femoral or contralateral upper extremity access may be used on rare occasions.
Direct infusion of the lytic agent into the thrombus is then performed for up to 72 hours, with frequent returns to the angiography suite during the infusion to assess the completeness of response. Although urokinase was the agent used most frequently in early reports of thrombolysis of upper extremity DVT, decreased availability of urokinase has led to the emergence of tissue plasminogen activator as an alternative lytic agent. Both agents appear to be equally safe and effective. In a retrospective review of patients treated with both modalities, Gelabert and colleagues noted equivalence in complete lysis (93%), return of normal arm function, and complication rates were 0% in the two groups. 9
One of the disadvantages of catheter-directed lytic infusions is the length of time involved in treating the thrombus. This may be associated with significant complications, including intracerebral hemorrhage, pulmonary embolism, and access-site bleeding. 10 Additionally, longer hospital lengths of stay may be required. To minimize the period of treatment, modified techniques have been used, including power-pulse spray thrombectomy and mechanical thrombectomy. Although this technique has gained acceptance in the treatment of iliofemoral DVT, it has only recently been described in patients with ASVT. In a small series from Shah and colleagues, three patients were successfully treated in a single session requiring only 2 to 3 hours of treatment time. 11 Schneider and colleagues reported the use of mechanical thrombectomy using the Angiojet (Possis Medical, Inc., Minneapolis, MN) device for thrombus debulking, followed by catheter-directed thrombolysis. 12 Using this strategy, thrombolysis time was reduced from an average of 48 hours for catheter-directed thrombolysis alone to 12 hours with the combined technique. The authors also reported a case of rethrombosis following first rib resection that was successfully treated with mechanical thrombectomy, thereby avoiding the risk of systemic thrombolysis in the early postoperative period.
Arko and colleagues also reported a method of combined mechanical and low-dose thrombolytic therapy to reduce both the time and dosage of thrombolysis. 13 Initial mechanical thrombolysis with the Solera Bacchus thrombectomy catheter (Bacchus Vascular Inc., Santa Clara, CA) was followed by low-dose thrombolysis using the Trellis Infusion System (Bacchus Vascular). Local thrombolytic infusion between the proximal and distal occlusion balloons allows for minimal thrombolytic volume (2.5 mL) and a significant reduction in time for thrombolysis.
The use of thrombolysis as a stand-alone agent for treatment of upper extremity DVT remains an area of controversy. If complete lysis without residual stenosis is achieved, it is reasonable to treat the patient with anticoagulation without further surgical intervention. In these situations, completion venography with the arms in the abducted position should be performed to rule out venous compression between the clavicle and first rib. Significant venous compression with abduction warrants a discussion of further surgical decompression of the thoracic outlet with the patient regardless of the venographic findings with the arms in a neutral position. In patients with incomplete thrombolysis, residual venous stenosis in the thoracic outlet, or both, further discussion should be held with the patient regarding surgical decompression, as is discussed later.
Angioplasty
As a stand-alone procedure in ASVT, angioplasty has been shown to be of questionable durability. Central venous lesions in the thoracic outlet are highly resistant to balloon angioplasty owing to the fibrotic nature of the venous lesions and surrounding connective tissue in addition to the persistent narrowing of the thoracic outlet between the clavicle and first rib. 14,15 If a persistent central vein stenosis is present following thrombolytic therapy, there is little to gain by attempting angioplasty at that point. Not only is the lesion resistant, but also the process of balloon inflation increases the inflammatory process at the angioplasty site, potentially adding to the complexity of any immediate surgical procedures to decompress the thoracic outlet.
For these reasons, angioplasty is usually withheld until after the thoracic outlet has been decompressed. The success rate is significantly enhanced in this setting owing to both removal of the bony constraints and release of fibrous connective tissue surrounding the vein.
Stenting
Stenting of stenotic venous segments in ASVT is generally discouraged, particularly in the absence of first rib removal. Owing to the motion and bony constraints in the thoracic outlet, stents placed without thoracic outlet decompression are highly prone to fracture with subsequent occlusion. Urschel and Patel reported 22 patients who developed subclavian vein occlusion following primary stent placement without first rib resection. 16 Seventeen patients achieved good functional results with repeat thrombolysis and first rib resection.
There is some support in the medical literature for stent placement following first rib resection. Kreienberg and colleagues reported 14 patients with residual (> 50%) stenosis following thrombolysis and first rib resection. 17 Short segment stenoses were treated with 10 to 12 mm self-expanding stents. Nine of 14 stents remained patent with a mean follow-up of 3.5 years. In the majority of case series to date, however, stenting is typically discouraged as adequate results can be obtained with first rib resection and angioplasty alone.
Thoracic Outlet Decompression
Perhaps the largest remaining controversy in the management of ASVT is the necessity and timing of surgical decompression of the thoracic outlet, typically by first rib resection. Although it is clear that some patients benefit from an aggressive approach, the procedure is not without risk and potential complications, so, as with most surgical procedures, proper patient selection is the key to an optimal outcome.
The rationale for first rib resection has been alluded to in previous sections. Persistent venous entrapment in the thoracic outlet is felt by many to lead to a high rate of recurrent venous thrombosis and ongoing disability. Resection of the first rib, along with resection of the associated anterior scalene and subclavius muscles, can be accomplished through a supraclavicular, subclavicular, or transaxillary approach depending on the preference and experience of the operator. Adjunctive angioplasty can be performed intraoperatively to augment reestablishment of optimal luminal diameter (Figures 1 and 2). Excellent anatomic and functional results have been reported in a number of single-center series (Table 1). 17–25

A, Acute thrombus involving subclavian, axillary, and brachial veins in a 25-year-old male. B, Venographic result following 18 hours of thrombolysis demonstrating residual stenosis between the clavicle and first rib. C, Intraoperative imaging following first rib resection and angioplasty of venous stenosis.
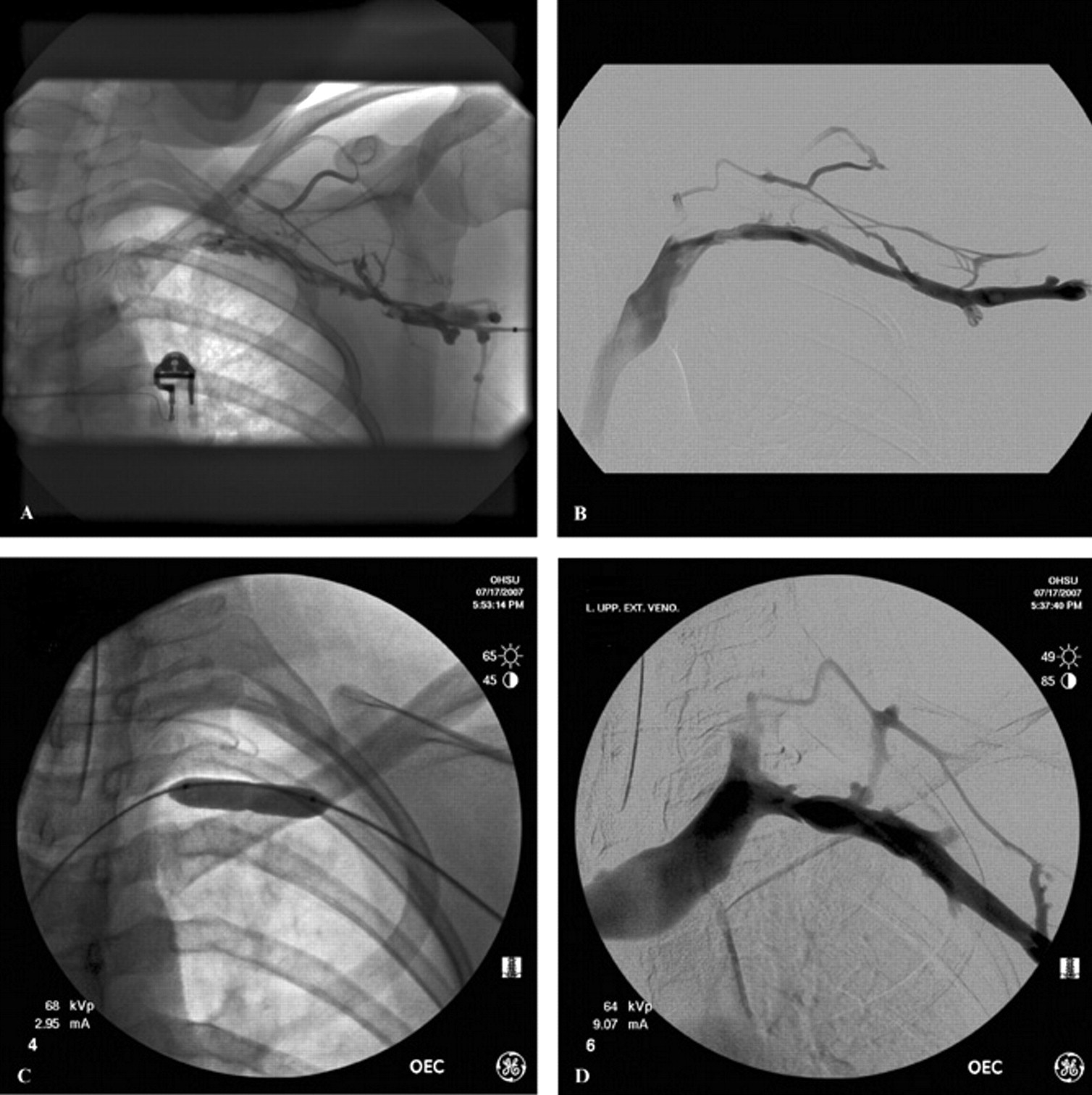
A, Acute thrombosis involving axillary and subclavian veins in a 17-year-old high school athlete. B, Venographic result following 12 hours of thrombolysis demonstrating residual stenosis between the clavicle and first rib. C, Intraoperative angioplasty following first rib resection; note residual waist in the midportion of the angioplasty balloon. D, Completion venogram following first rib resection and venous angioplasty.
Results of Combined Endovascular and Surgical Treatments for Acute Axillary-Subclavian Venous Thrombosis
PTA = percutaneous transluminal angioplasty.
The timing of first rib resection is a subject of ongoing debate. Traditionally, a waiting period of at least 4 to 6 weeks following recanalization has been advocated. The rationale for delayed surgery is the presence of an acute inflammatory response around an acutely thrombosed and recanalized vein.
Favorable reports from a number of recent series demonstrating excellent surgical results with immediate surgical intervention have led to an overall trend toward earlier operative interventions. The group from the University of California-Los Angeles recently compared outcomes of thrombolysis and surgical decompression in patients treated immediately versus those treated with staged resections. 21 The authors found comparable rates of thrombus resolution and functional recovery in both groups, with no increase in operative morbidity in the early treatment group. Azakie and colleagues reported the results of 34 thoracic outlet decompression procedures, 21 of which were performed acutely within 1 week of onset and 13 of which were performed for chronic stenoses or occlusions. 19 In the acute group, 95% regained their preoperative functional status, whereas in the chronic group, four patients reported persistent limitations of activity.
Selective first rib resection is also advocated by a number of groups. Lee and colleagues reported a series of 22 patients with Paget-Schroetter syndrome treated with initial thrombolysis and anticoagulation. 20 Patients were evaluated at 1 month, and surgery was offered to those who remained symptomatic, whereas those whose symptoms had resolved were managed with 2 additional months of anticoagulation. Durable symptomatic improvement was noted in 85% of the surgically treated group and 89% of the conservatively treated group. The same group subsequently evaluated 35 patients managed conservatively. 26 Eight patients (23%) developed worsening symptoms and underwent first rib resection at a mean of 13 months, whereas 27 patients (73%) remained symptom free at a mean of 55 months. Symptomatic recurrences were more frequent in young patients (< 28 years old) and patients treated with stents.
Lokanathan and colleagues also reported the management of 25 patients with acute ASVT treated with thrombolytic therapy and selective surgical decompression. 27 Patients with complete resolution of thrombus were treated with anticoagulation for 3 months. Patients with residual thrombus or stenosis were treated with angioplasty alone with anticoagulation if symptoms were mild or first rib resection for more severe symptoms. Using this strategy, only two patients in this cohort underwent first rib resection. After a mean follow-up of 2.9 years, 28% were symptom free, 62% had mild symptoms, and 10% had more severe symptoms.
In some cases, partial claviculectomy may also be indicated as a method of thoracic outlet decompression. Green and colleagues reported a series of 11 patients with incomplete thrombolysis and persistent venous stenosis in the costoclavicular space who were treated with medial claviculectomy with venous repair. 28 All 11 returned to their preoperative function, although 2 of 11 expressed dissatisfaction with the scarring and bony deficit following this procedure.
Failure of initial surgical management of acute ASVT or chronic ASVT not responsive to thoracic outlet decompression alone may require alternate surgical methods of reconstruction. Endovascular management is less applicable in the chronic situation, in which well-established thrombus is less responsive to lytic therapy or balloon dilatation. Venous bypass procedures using a saphenous or femoral vein and internal jugular turndown procedures have been described for treatment of chronically occluded subclavian veins.
Post-Thrombotic Syndrome
The incidence and severity of post-thrombotic syndrome are less well established for upper extremity DVT than the more common lower extremity DVT. The diagnosis of post-thrombotic syndrome in patients with upper extremity DVT is likewise less clear, although some degree of persistent arm pain and swelling is felt to be necessary for the diagnosis. An attempt has been made to develop an objective scoring system using modifications of existing criteria for lower extremity post-thrombotic syndrome. 29,30 These scales have not yet been validated.
In a recent meta-analysis, Elman and Kahn reported a mean frequency of post-thrombotic syndrome following upper extremity DVT of approximately 15%. 31 Risk factors associated with the development of post-thrombotic syndrome included the presence of residual thrombus and documented thrombophilia. Catheter-associated DVT is less frequently associated with post-thrombotic syndrome than Paget-Schroetter syndrome.
Summary
Endovascular treatment options are gaining increased prominence in the management of primary ASVT. Although anticoagulation alone has long been the standard of care, the benefits of early recanalization with thrombolytic therapy are becoming increasingly recognized. Adjunctive surgical treatment with first rib resection is seen by many to be an essential component of definitive therapy. Evidence to support this is based on numerous single-center series demonstrating excellent functional outcomes with aggressive treatment, although no level 1 evidence to support this currently exists. It is unlikely that a randomized controlled trial comparing operative and nonoperative therapy will be performed, so practitioners will likely have to form their opinions based on the available evidence. Angioplasty is seen by many to also play an adjunctive roll in conjunction with thoracic outlet decompression, although stenting rarely seems indicated in this anatomic location.