
Abstract
Symptomatic obstruction of the superior vena cava (SVC) can be caused by either intrathoracic malignancy or nonmalignant etiology resulting in superior vena cava syndrome (SVCS). The objective of this study was to evaluate the clinical outcome of percutaneous stenting of SVCS in patients with malignant and benign disease. During a 9-year period, 56 patients with SVCS underwent percutaneous stenting placement. Among them, malignant and benign disease was responsible for 40 patients (71%) and 16 patients (29%), respectively. The Wallstent was the most commonly used stent and was used in 45 patients (80%), whereas the Palmaz stent was used in 6 patients (11%). In 38 patients (68%), a single stent was deployed to treat an SVC lesion. In contrast, bilateral kissing stents were deployed in 9 patients (16%), which extended from bilateral brachiocephalic veins to the proximal SVC. Technical success was achieved in all patients while symptomatic improvement was noted in 54 patients (96%). No procedural complications occurred in this series. Primary patency in malignant and benign cases at 1 year was 64% and 76%, respectively. Overall symptom-free survival ranged from 1 to 34 months. Our study showed that endovascular treatment with percutaneous stenting provides an effective treatment strategy in patients with SVCS caused by either malignant or benign disease.
Superior vena cava syndrome (SVCS) refers to obstruction of venous flow from the upper torso into the right atrium. In the majority of cases, the etiology is due to an underlying malignancy. Most commonly, these malignancies are small cell or non–small cell lung cancers in the right upper lobes of the lung, but significant mediastinal lymphadenopathy or compression of the heart may produce SVCS as well. 1,2 SVCS can also be caused by nonmalignant etiologies, such as mediastinal fibrosis secondary to an infectious process such as tuberculosis or radiation-induced mediastinal fibrosis. 3,4 With an aging population on the rise, the frequency of central venous device placement such as a pacemaker, defibrillator, central venous infusion port, or chronic hemodialysis catheter is similarly increasing. These devices can cause central venous endothelial irritation owing to mechanical trauma, which can lead to intraluminal fibrosis. The resultant central venous occlusion owing to mechanical trauma caused by these indwelling central venous devices can invariably lead to SVCS. 5,6
Symptomatic SVCS should be treated as a clinical emergency, with immediate treatment strategies including upper body and head elevation and steroid administration to decrease soft tissue swelling and alleviate compressive symptoms. Although up to 80% of cases of malignant SVCS respond to chemotherapy and/or radiation therapy, many patients do not experience any symptomatic improvement owing to underlying critical superior vena cava (SVC) compression. 1–7 In fact, an autopsy study suggested that complete or partial patency was maintained in only 24% of patients treated with radiotherapy, 8 and a recent systematic review failed to show any significant difference between the effectiveness of radiotherapy, chemotherapy, or combination radiation-chemotherapy. 9 Although surgical reconstruction has been reported for palliative treatment in SVCS patients, it is not considered the main treatment of choice owing in part to the high rate of operative morbidity and mortality. 10
Advances in endoluminal vascular interventions have led to numerous reports describing percutaneous stenting of symptomatic SVCS as an effective treatment in providing palliative control of malignancy-related SVCS and definitive treatment in benign cases. 11–14 First described in 1986 by Charnsangavej and colleagues, 15 endovascular stenting for SVCS has been shown to be an effective treatment with high technical success rates. 2,7,12–14 The objective of this study was to review our institutional experience of percutaneous stenting of SVCS in patients caused by both malignant and benign etiologies.
Patients and Methods
Patient Cohort
The clinical data and radiologic records of 56 patients who underwent percutaneous stenting for SVCS from December 1998 to July 2007 were retrospectively reviewed. Patients with either malignant or benign causes of SVCS were included in the analysis. Pertinent hospital records were reviewed for information with regard to underlying etiology of SVCS, clinical presentation, relevant medical comorbidity, technical approach, procedural complications, and clinical outcome. Follow-up information regarding symptomatic relief or recurrence was obtained from clinic charts or telephone interview.
Technique of SVC Stenting
The SVC stenting procedure was performed in either the hybrid endovascular operating room (n = 12) or interventional radiology suite (n = 44). Femoral venous access was established in all patients with a 9F introducer sheath (Boston Scientific, Natick, MA). A 260 cm Bentson guidewire (Boston Scientific) followed by a pigtail catheter was placed in the SVC. Venography of the SVC and brachiocephalic veins was performed via a femoral approach to visualize the SVC lesion. Whenever possible, a hydrophilic guidewire was used to traverse across the SVC lesion. Once the lesion was successfully cannulated using a hydrophilic wire, a guidewire exchange was performed for a stiff Amplatz (Boston Scientific) or a Lunderquist wire (Cook, Bloomington, IN) for stent delivery. In the event of venous occlusion involving the SVC or brachiocephalic veins, bilateral upper extremity venous access via either a brachial or basic vein approach (n = 11, 20%) was established to facilitate the catheterization of the central vein occlusion. Jugular venous access was necessary in six patients (11%) to establish a through-and-through guidewire access for stent delivery and deployment. System anticoagulation with intravenous heparin (5,000 U/kg) was given prior to any catheter-based intervention. Balloon angioplasty to dilate the SVC or brachiocephalic venous lesion was performed routinely with either a 10 × 40 mm or 12 × 40 mm balloon angioplasty catheter. Following balloon dilatation of the SVC lesion, either a balloon-expandable stent (Palmaz stent, Johnson & Johnson Interventional System, Warren, NY) or a Wallstent (Boston Scientific) is deployed across the lesion. The choice of stent placement was based on the discretion of the treating interventionalist. If a single stent was insufficient to cover the entire lesion length, additional stent placement was deployed to ensure that at least 10 mm of the stent was bridged beyond the lesion segment. Post-stenting balloon dilatation was routinely performed when the Wallstent was deployed. If the segment of SVC adjacent to the stricture was greater than 16 mm in diameter, a bilateral brachiocephalic kissing stent technique using either 12 or 14 mm diameter Wallstents was performed. This brachiocephalic kissing stent technique was performed either via the bilateral femoral vein (n = 3; 5%) or a bilateral upper extremity approach (n = 5; 9%). In this kissing stent technique, the proximal Wallstent was positioned in the proximal SVC, whereas the distal stent was extended to the respective brachiocephalic vein. Bilateral post-stenting kissing balloon dilatation was performed simultaneously across the lesion. Completion venography was performed to document the treatment result (Figure 1). Introducer sheaths and guidewires were next removed, and manual pressure compression was performed to achieve hemostasis.

A representative image of a patient with symptomatic superior vena cava syndrome. A, A high-grade superior vena cava stenosis depicted in the venogram (black arrow). B, Luminal patency was established by the placement of a balloon-expandable Palmaz stent (white arrow). C, Chest radiography revealed the location of the Palmaz stent (long white arrow).
Anticoagulation Regimen
All patients received an intravenous bolus of heparin (100 U/kg) prior to the balloon dilation and stenting procedure. Systemic anticoagulation with heparin was continued for 3 to 6 days following the intervention. During this time, oral anticoagulation with warfarin was initialed to maintain an international normalized ratio between 2.0 and 3.0. Thirty-two patients (57%) received this regimen in which warfarin was continued for 6 months, whereas eight patients (14%) were placed on a lifelong regimen of oral warfarin therapy. In the remaining 16 patients (29%) patients, systemic heparin was maintained for 24 hours following the therapy and antiplatelet agent clopidogrel was continued for 6 months.
Definition and Parameter Analysis
Technical success was defined by the ability to recanalize occluded or strictured SVC followed by deployment of a stent to establish luminal patency. In the event of bilateral brachiocephalic occlusion, technical success was defined by the establishment of luminal patency of at least one brachiocephalic venous stent. Clinical success was defined by significant improvement in or resolution of symptoms of SVCS within 48 hours following the stenting procedure. Relevant factors in the consideration of clinical success included resolution of facial and upper extremity swelling, dizziness, headache, plethora, tinnitus, or dyspnea. In patients whose persistent dyspnea was attributable to underlying thoracic or mediastinal malignancy, their dyspneic symptom was not excluded from consideration when assessing treatment success. Follow-up visits were performed at 1, 3, 6, and 12 months. Upright chest radiography and venous Doppler ultrasonography were performed to evaluate the patency of jugular and brachiocephalic veins and SVC. Primary and secondary patency rates of stented vessels were analyzed.
Results
Patient Characteristics
Among the 56 patients treated with percutaneous stenting of SVCS, malignancy causes were identified in 40 patients (71%), whereas the remaining 16 patients (29%) suffered nonmalignant processes resulting in their SVCS. The etiologic factors of their SVCS are shown in Table 1. Overall, 60 stenting procedures, including 62 stents, were performed in these 56 patients (42 men; mean age 62.6 ± 8.4 years, range 32–82 years).
Etiologies of Superior Vena Cava Syndrome
SVCS = superior vena cava syndrome.
Treatment Outcome
Technical success was achieved in all patients, whereas clinical success was achieved in 96% (54 of 56). Two patients with small cell cancer of the lung experienced persistent neck and upper extremity swelling despite successful stent placement in their SVC and brachiocephalic lesions. One of these two patients experienced moderated symptomatic improvement following radiotherapy. In two patients (4%) whose brachiocephalic occlusion was attributed to a thrombotic process, successful recanalization was achieved with rheolytic AngioJet mechanical thrombectomy (Possis, Minneapolis, MN) and catheter-directed mechanical infusion of tissue plasminogen activator (Alteplase, 10 mg, Genentech, San Francisco, CA). Following the pharmacomechanical thrombectomy, successful stenting of his brachiocephalic vein and SVC was performed using two overlapping Wallstents.
Successful balloon dilatation was achieved prior to stent placement in all patients (100%). A Palmaz stent (Johnson & Johnson) was used in 6 patients (11%), whereas a Wallstent was used in the remaining 45 patients (80%). With regard to the Wallstent, the most commonly used stent diameter size was 16 mm (n = 24; 53%), followed by 14 mm (n = 12; 27%) and 18 mm (n = 2; 4%). A single stent was used in 38 patients (68%), whereas two and three stents were necessary in 14 patients (25%) and 4 patients (7%), respectively.
There were no procedure-related complications in our series. Four patients with benign SVCS (25%) who required chronic hemodialysis developed SVC stent occlusion in 4, 6, 7, and 10 months, respectively, following the stent placement. They all underwent successful reintervention with balloon dilatation. Additional stent placement was necessary in two of these patients in their secondary intervention.
A Kaplan-Meier life table depicting their survival rate is shown in Figure 2. Primary patency in patients with malignant and benign causes of SVCS was 64% and 76%, respectively, at 1 year (Figure 3). Eighteen patients (45%) with malignant SVCS died from their underlying malignancy within 6 months following SVCS intervention, and seven patients (18%) of the same group remained alive at 1 year. Six patients with benign SVCS underwent reintervention owing to recurrence of facial or upper torso swelling. High-grade stenosis was demonstrated on a venogram during secondary intervention in all four patients. With a mean pressure gradient of 25 mm Hg, these lesions were successfully treated with balloon dilatation (n = 2) or repeat stent placement (n = 2). The mean follow-up period in patients with malignant and benign causes was 8.3 months (range 1–21 months) and 28 months (4–57 months), respectively. Overall symptom-free survival ranged from 1 to 34 months (mean 14.8 months).

Kaplan-Meier survival curves of patients with malignant (solid line) and benign (dotted line) superior vena cava syndrome.
Discussion
The traditional treatment for SVCS associated with thoracic malignancy has been radiotherapy, chemotherapy, or combination radiation-chemotherapy. Responses to these treatments are frequently delayed, however, and a significant number of patients either fail to respond or experience recurrence of SVCS. 8 In contrast, nonmalignant processes can lead to the development of SVCS, with common etiologies including indwelling venous catheters or cardiac pacemaker devices. For these patients, even fewer effective treatment options existed. Endovascular stenting of the SVC, however, has emerged as a treatment armamentarium for both malignant and nonmalignant SVCS. In contrast to medical therapy for malignant SVCS, endovascular stenting of SVC establishes luminal patency immediately and provides rapid symptomatic relief, which results in a high clinical success rate. 2–4 Consistent with other reports, 4–7,11–13 the findings of our study underscored the therapeutic role of percutaneous stenting in SVCS in both malignant diseases and benign etiologies.
Although the therapeutic efficacy of percutaneous stenting in intra-arterial lesions is well proven, 16 comparable evidence in venous pathology remains scarce, particularly with regard to vena cava obstruction. Since the first use of stenting in SVCS was described, reports of using a variety of metallic stents have been described in palliative treatment of SVCS. 17–20 In the earlier clinical series, the Gianturco Z-stent (Cook) was the most commonly used stent of choice. 21,22 Because the Z-stent provides the greatest radial force in the middle segment of the stent, placement of multiple overlapping Z-stents is necessary when treating long venous lesions. Several studies have highlighted the benefit of using a Z-stent in recanalized SVC occlusion. 23–25 Despite the high radial force of the stent, it did not gain wide acceptance in clinical practice owing to metal fatigue with the possibility of fracture in a long-term study. 15,26 Another type of stent that is widely used in the treatment of vascular lesions is the Palmaz stent (Johnson & Johnson), a balloon-expandable stent with a high radial force that is ideally suited in lesions with extrinsic luminal compression. We used this device in six patients in our series, whose causative factors of SVC lesions were catheter-related fibrosis and focal narrowing owing to radiation-induced fibrosis. This stent can be deployed precisely based on the location of balloon expansion. A major advantage of this stent is that it can be dilated to nearly 80% larger than its intended diameter using an oversized balloon catheter while maintaining strong radial force. However, the disadvantage of this stent relates to its compressibility, which may lead to stent deformation or occlusion caused by extrinsic compression from an adjacent extraluminal mass. 27,28
The most commonly used stent in this study, consistent with other reported series, 5,12,17,20 was the Wallstent, which was used in 80% of patients. The primary advantages of this stent are its flexibility and ease of deployment, which are ideally suited for long or tortuous lesions. However, a potential disadvantage is noteworthy when using a large-diameter Wallstent in patients with a critically stenotic SVC, which may result in low radial force owing to uneven stent conformability. When using this stent to treat a long-segment vascular lesion, significant stent foreshortening can occur, which may lead to stent migration if the device is not centered on the stenosis. 13,29 The clinical efficacy of the Wallstent in SVCS has been reported by several authors. 30,31 Dyet and colleagues reported a primary patency rate of 90% and a secondary patency rate of 100% in patients with symptomatic SVCS. 32 Oudkerk and colleagues reported the outcome of a comparative analysis between the Wallstent and the Z-stent in palliative treatment of SVCS and showed similar clinical success and patency rates between the two devices. 33 Because the majority of currently available self-expanding nitinol stents do not have a diameter greater than 12 mm, their role in the management of SVCS remains limited. In contrast, the wide range of large-diameter Wallstents (up to 18 mm) provides a versatile treatment option in structures such as SVC or brachiocephalic vein. Although researchers have proposed the use of stent graft in venous pathology, we do not believe that it provides a significant advantage compared with a Wallstent because of potential coverage of important venous collaterals in patients with SVCS, which might worsen the symptoms if the stent graft becomes occluded.
Access for percutaneous stenting of the SVC is typically obtained via the femoral vein, but brachial, basilic, or internal jugular access can also provide useful therapeutic access to the central veins. 34–36 Although we established femoral access in all patients in our series, additional upper extremity venous access was necessary in 20% of patients, which not only enabled antegrade and retrograde venography but also facilitated canalization of the SVC lesion. Jugular-femoral access was used in six patients because it enabled the creation of an exteriorized through-and-through guidewire to facilitate stent delivery. Initial balloon dilatation is an important maneuver as it dilates luminal patency, which facilitates subsequent stent deployment; other researchers have similarly supported this maneuver. 34,37 In contrast, others have advocated the avoidance of this maneuver in an effort to reduce the risk of thrombus embolization. 38 Treatment by means of balloon dilation alone yields poor clinical results in the long term owing to a high percentage of restenosis. Given the available clinical results, stenting of the SVC lesion is the preferred treatment compared with SVC balloon angioplasty.
In a Cochrane systematic review of treatment for malignant SVC obstruction, Rowell and Gleeson reported that stent insertion provided more rapid symptomatic relief and in a higher proportion of patients (95%) compared with radiation therapy or chemotherapy. 9 Other researchers have reported similar success rates of 95 to 100% in patients with malignancy-associated SVCS following endovascular interventions. 39 In our series, clinical success was achieved in 96% (54 of 56). Primary patency in patients with malignant and benign causes of SVCS was 64% and 76% at 1 year, respectively. During the follow-up period, symptoms owing to thrombosis recurred in three patients who required chronic hemodialysis via upper extremity arteriovenous access. All of these patients were successfully treated with repeated stent placement in their SVC or brachiocephalic veins. Kee and colleagues reported technical success of 95% (56 of 59 patients), primary clinical patency of 79%, and secondary clinical patency of 93%. 40 Their mortality and morbidity rates were 3% and 10%, respectively. Rosch and colleagues reported one recurrence in a group of 20 patients during a follow-up period of 7 months (range 1–11 months). 21 The reported recurrence rate in the literature ranges from 0 to 45%. 5,12,17,20,34 Gross and colleagues reported a primary patency rate of 100% at 6 months in 13 patients without recurrences during a follow-up period ranging from 3 to 180 days. 41 Nicholson and colleagues performed a comparative study between the results obtained in 76 SVCS patients treated with stents with or without associated radiotherapy, with those of 25 retrospective cases treated only with radiotherapy. 42 These authors concluded that stent insertion provided faster relief of symptoms and significantly greater improvement in the SVC obstruction score than radiation therapy.
In our series, benign disease was responsible for SVCS in 29% (n = 16) of patients. The proportion of these benign etiologies was surprisingly greater compared with other contemporary series. 11–13,15,17,18,20,34 The clinical outcome of our series is comparable to a study by Gregorio Ariza and colleagues, whose clinical success was 85%. 34 Petersen and Uchida reported the long-term result of stenting in 19 patients with SVCS caused by benign processes. 18 With a mean follow-up period of 33 months, their primary patency was 83%, and secondary patency was 100%. In a similar study, Sheikh and colleagues performed SVC stenting in 19 patients with nonmalignant SVCS. 37 It is noteworthy that 74% of them (16 of 19) developed SVCS owing to underlying indwelling intravascular catheters or devices. These patients had a remarkable clinical response following stenting, with a clinical success rate of 100%.
SVC or brachiocephalic vein occlusion in patients requiring chronic hemodialysis poses a particular clinical challenge. Owing in part to the high turbulent flow created during episodic hemodialysis treatment, their central venous lesion tends to exhibit a higher incidence of restenosis following stent placement and a shorter treatment patency rate. Kovalik and colleagues reported their experience of treating 20 patients requiring hemodialysis who developed symptomatic central vein stenosis. 43 In those patients who showed nonelastic central venous stenosis (defined by residual lumen greater than 50%), their recurrence rate was 81% during a follow-up period of 7.6 months. In contrast, in those with elastic stenosis, the average time from treatment to recurrence was 2.9 months and the recurrence rate was 100%. The authors observed that the placement of Wallstent prostheses in nonelastic lesions had a lower recurrence rate than those with elastic stenotic lesions. Consequently, these researchers postulated that it may be necessary to place stents in nonelastic stenoses in patients subjected to hemodialysis but not in those cases of elastic stenosis or minimal elasticity. 43 A similar finding was noted in our series in which four patients with a chronic indwelling hemodialysis catheter all developed in-stent stenosis following SVCS intervention. Secondary intervention was necessary in all four patients to restore the luminal patency of their stents.
Many groups performing endovascular stenting for SVCS administer thrombolytic agents. 34,44 Gregorio Ariza and colleagues administered a urokinase 500,000 IU bolus followed by an infusion of 80,000 to 100,000 IU/h for 24 to 48 hours after stent implantation. 34 Other groups performed no thrombolysis, perhaps electing to perform repeated stenting when stent thrombosis occurred. 35 Either heparin, oral anticoagulants, or antiplatelet therapy is typically given after the procedure, for a duration of at least 6 months and possibly indefinitely. 34–38 Overall, this anticoagulation is well tolerated and appears to decrease the risk of stent thrombosis, but fatal subdural hematoma was reported in a patient with nonmalignant SVCS. 37 In our series, one patient with brachiocephalic vein thrombosis underwent a successful rheolytic thrombectomy with concomitant catheter-directed tissue plasminogen activator infusion. This treatment of pharmacomechanical thrombectomy was adapted from our previously reported technique in deep venous thrombosis intervention, 45 and it was successful in removing acute thrombus in the SVC and brachiocephalic vein.
In summary, our study showed that percutaneous stenting provided remarkable clinical benefit in patients with both malignant and nonmalignant SVCS. This is an effective treatment for palliative therapy in patients with malignant SVCS. Nearly all patients experienced complete symptomatic relief following SVC stenting, and excellent long-term symptomatic relief was sustained following this percutaneous intervention. Repeat intervention may be necessary in patients requiring chronic hemodialysis. The role of long-term anticoagulation may play a role in SVCS patients with thrombotic predispositions. Additional study is needed to determine the ideal imaging and timing for periodic surveillance following SVC stenting and the adjunctive therapy with regard to the use and duration of anticoagulation regimens.
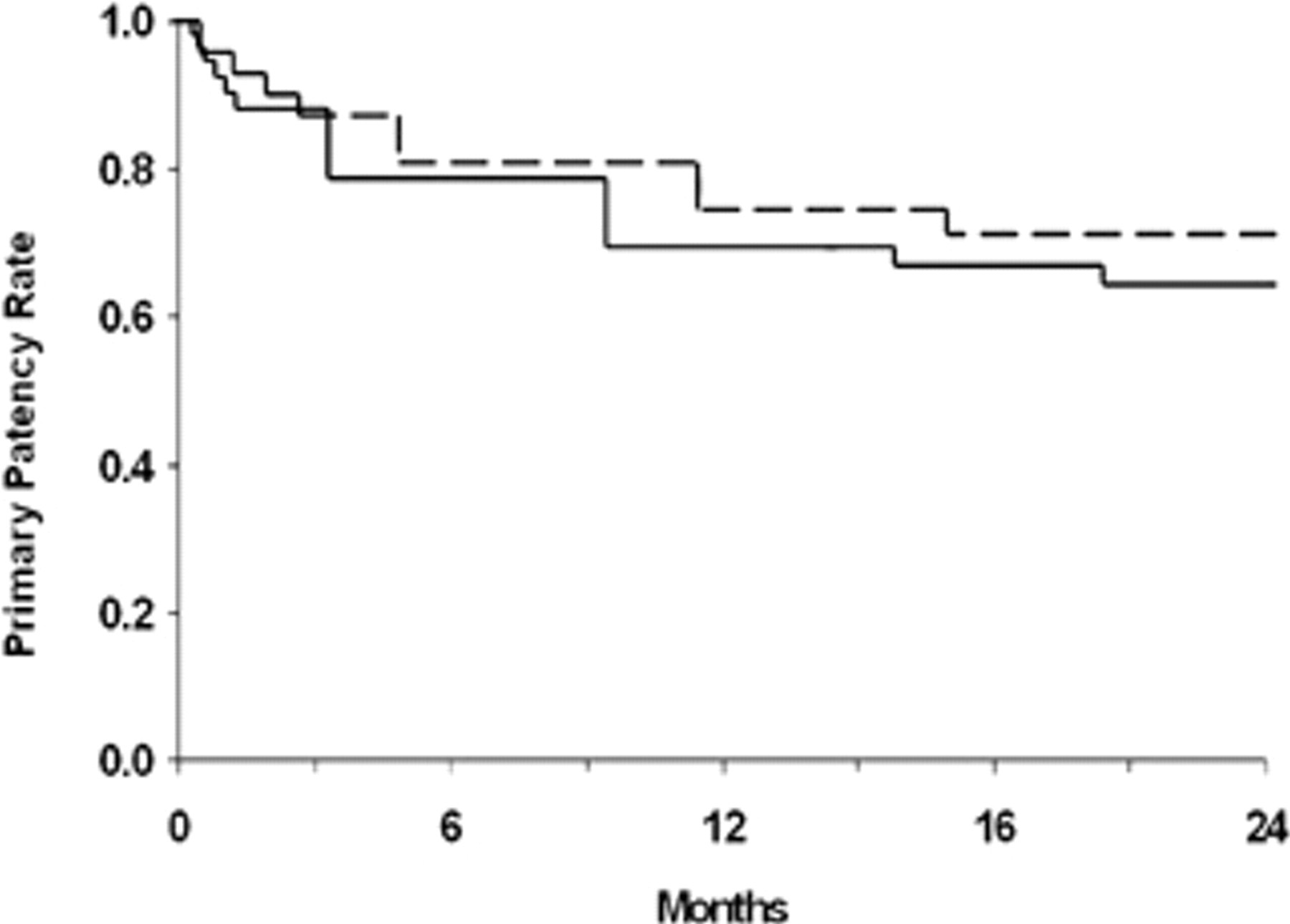
Primary stent patency rates of patients with malignant (solid line) and benign (dotted line) superior vena cava syndrome.