
Abstract
Systemic anticoagulation with heparin or its unfractionated derivatives followed by warfarin therapy has been the mainstay of treatment in patients with lower extremity deep venous thrombosis (DVT). Although heparin is an effective treatment modality in preventing thrombus propagation, it provides minimal therapeutic effect in dissolving preexisting venous thrombus. The clinical consequence of DVT, owing in part to loss of venous endothelial and valvular function, is postphlebitic syndrome or chronic venous insufficiency. Current advances in endovascular therapy have resulted in various endovascular thrombectomy systems that can effectively remove a large venous thrombus burden, which may represent a potential advantage of preserving venous valvular function and thereby reduce the likelihood of postphlebitic syndrome. In this article, we review a variety of surgical and interventional methods in venous thrombus removal. Current treatment modalities using mechanical thrombectomy devices and pharmacomechancial thrombectomy strategy are also discussed.
Since the discovery of heparin in 1916, 1 its main clinical use has been in the treatment and prophylaxis of deep venous thrombosis (DVT). For more than 50 years, the mainstay of therapy has been immediate anticoagulation with unfractionated or low-molecular-weight heparin followed by warfarin therapy for some period of time. 2,3 Nonetheless, anticoagulation alone is not completely effective in alleviating or preventing the early and late clinical sequelae associated with lower extremity DVT, such as pulmonary embolism, recurrent DVT, and post-thrombotic syndrome. 4–6 Furthermore, loss of valve integrity either by obstruction or direct damage results in venous hypertension and, eventually, postphlebitic syndrome. Heparin effectively prevents new clot formation but has little effect on the clot already present prior to therapy. As a result, valve destruction and dysfunction are rarely prevented by anticoagulation alone.
Lower extremity acute DVT is a common manifestation of venous thromboembolism, with an incidence of approximately 1 per 1,000 population in the United States. 7 The pathophysiology of early and late lower extremity post-DVT morbidity is believed to be the result of venous outflow obstruction, venous valvular insufficiency, and calf muscle pump dysfunction. 8,9 Complete normalization of a lower extremity venous duplex ultrasound examination will occur only in approximately 75% of patients treated with anticoagulation alone at 6 months. 10 The lack of complete normalization of the duplex ultrasound examination is an independent predictor for recurrent DVT, with up to an eightfold increased risk for DVT recurrence in these patients. 11,12 Furthermore, there is a clear difference in return to normal function based on the segment involved with the DVT. Proximal DVT rarely results in normal venous hemodynamics after anticoagulation therapy, whereas calf vein DVT routinely recanalizes, independent of therapy, without major clinical sequelae. Therefore, if clinical improvement in DVT outcomes is to be achieved, then some therapy other than anticoagulation alone seems necessary, particularly in lower extremity DVT.
Even complete resolution of lower extremity DVT does not guarantee freedom from morbidity, with up to a 60% incidence of valvular insufficiency seen in post-DVT vein segments. 13 Thrombosis is associated with a significant systemic inflammatory response, 14 and this likely plays a role in the observed result. The inflammatory cascade may lead to sclerosis of the vein and its valves, leading to valvular insufficiency. Rapid spontaneous thrombolysis seems to preserve venous valvular function in the iliofemoral vein segments 15,16 ; thus, facilitating this process is a logical evolution of the treatment algorithm. Almost certainly, the inflammatory damage associated with DVT is a duration-related effect. For this reason, early clot lysis or removal would certainly seem to add benefit in preventing postphlebitic valve damage and the resultant venous hypertension.
In a canine DVT model, both pharmacologic thrombolysis and open mechanical thrombectomy preserve valvular competence, with preserved venous vasoreactivity in the thrombolysis group. 17 Over the last 40 years, there have been at least 18 randomized trials comparing systemic thrombolysis with anticoagulation alone in DVT treatment, and although systemic thrombolysis resulted in better thrombus resolution, patients had increased bleeding complications. 18 Nonetheless, early removal of clot did seem to preserve valve function in many of these series. Catheter-directed thrombolysis was developed in an effort to reduce the risk of bleeding complications by minimizing systemic distribution of the thrombolytic agent. Compared with anticoagulation alone, patients randomized to catheter-directed thrombolysis demonstrated increased 6-month patency and lower valvular insufficiency. 19 Patients who have undergone catheter-directed thrombolysis report better physical functioning and fewer post-thrombotic symptoms when answering standardized questionnaires compared with patients who received anticoagulation alone after a mean follow-up of 16 months. 20 The postphlebitic syndrome is cumulative, often occurring years after the initial thrombotic event. Thus, long-term follow-up is the only true proof of the success of any given treatment approach.
Catheter-directed venous thrombolysis, although effective, often requires infusion over hours or even days, with intensive patient monitoring and repeated trips to the endovascular suite for follow-up venograms. In many cases, chronic clot from a previous DVT may be present with acute clot as well. Thrombolysis is generally effective only on acute or subacute clot; therefore, incomplete lysis may be seen even with clinical success. This is particularly true in the setting of proximal left iliac vein webs, also known as May-Thurner syndrome (Figure 1). Chronic webs form as a result of left iliac vein compression by the right common iliac artery, predisposing patients to left-sided DVT, particularly in the proximal venous segments. These defects in the left iliac vein predispose patients to the formation of occlusive iliofemoral DVT on the left side. As a result, even with clot lysis, these chronic occlusions need to be cleared to prevent recurrent iliofemoral DVT. Commonly, venous stents are required to hold the iliac artery off the left iliac vein to prevent restenosis or rethrombosis.

May-Thurner syndrome: compression of the left common iliac vein on this anteroposterior venogram by the calcified right common iliac artery.
Frequently, the underlying medical comorbidities of a patient can represent treatment contraindication to thrombolysis, which severely limits its applicability. Pharmacologic thrombolysis is contraindicated with virtually any intracranial pathology, including stroke, tumor, or arteriovenous malformation. In many of these clinical situations, the use of anticoagulation is contraindicated as well. Even in the setting of a relative contraindication to thrombolysis or anticoagulation, the duration of treatment will result in an increase in bleeding risk for the patient. Therefore, mechanical adjuncts have been used to speed up the process of clot removal compared with catheter-directed thrombolysis alone. Mechanical thrombectomy for lower extremity DVT can debulk thrombus burden without the risks associated with thrombolytic therapy, and with new devices and techniques, this can often be performed using a percutaneous approach.
Open Surgical Thrombectomy for DVT
Prior to the introduction of intravenous heparin, surgical thrombectomy was the only effective means for treating a symptomatic lower extremity DVT, 21 but the reported outcomes of open surgical venous thrombectomy for acute lower extremity DVT have been mixed. 22 The 2004 American College of Chest Physicians consensus statement on the treatment of thromboembolic disease recommended against the routine use of venous thrombectomy in acute DVT except in cases of phlegmasia cerulea dolens. 23 Two issues are seen with conventional open venous thrombectomy. First, open surgical thrombectomy is associated with significant blood loss during the procedure. Owing to the need to remove clot while preventing pulmonary emboli, venous flow is reversed externally and the attendant blood loss is high, particularly in the iliofemoral segments and inferior vena cava. Second, rethrombosis occurs in many patients despite postoperative anticoagulation. This occurs owing to the damage to the venous endothelium, either from the clot itself or from the mechanical damage done in an effort to remove the thrombus. More contemporary reports have demonstrated that open surgical thrombectomy can be effective, 24–29 but, overall, there is a paucity of randomized data.
Plate and colleagues randomized 62 patients with iliofemoral DVT to either conventional anticoagulation or open surgical thrombectomy with temporary arteriovenous fistula (AVF). 25 At 6 months, patients treated with thrombectomy had significantly higher proportions with normal phlebography of the iliofemoral segment, no valvular insufficiency, and freedom from post-thrombotic symptoms. Of note, there was no difference in the patency of the femoropopliteal segments between the two groups. Juhan and colleagues followed 77 patients who underwent open surgical thrombectomy for acute lower extremity DVT and reported results after a mean follow-up of 8 years. 24 The 5-year secondary patency was 84% of the iliofemoral segment, and 80% of patients had no valvular insufficiency at 5 years. Over 90% of patients had no post-thrombotic symptoms at 5 years. Meissner and Huszcza reported on the results of 30 patients who underwent open surgical thrombectomy for DVT with temporary AVF with a 1-year follow-up. 28 There were three deaths owing to complications from phlegmasia cerulea dolens, but none were directly related to the operation. In follow-up, no patients developed recurrent DVT, with a majority of patients reporting no post-thrombotic symptoms at 1 year.
The success of open surgical thrombectomy depends on the complete removal of thrombus from the affected veins. This will require multiple lower extremity incisions and multiple procedural maneuvers, such as balloon embolectomy, milking of thrombus with sequential wrapping of the lower extremity, copious irrigation, and the creation of an AVF 22 and yet may not be successful. Postoperatively, patients are at risk for wound complications and will need a separate procedure to ligate the AVF (if performed) in several months' time. In addition, an open approach does not necessarily address the underlying etiology for the acute DVT, such as left common iliac vein compression by the right common iliac artery, which would require a significantly more complex procedure.
In summary, open surgical thrombectomy has a very limited role in the management of acute DVT. The limitations to the procedure are obvious, and the results are ambiguous at best. For this reason, open surgical thrombectomy for DVT is reserved as a last resort for those patients with threatened limb loss secondary to extensive DVT and phlegmasia.
Percutaneous Thrombectomy
In the United States, open surgical thrombectomy was largely abandoned in the 1980s owing to the severity of complications associated with its use. 30 The one area where its use remains is in those patients with phlegmasia and venous gangrene. In these patients, early removal of the obstruction is the only solution to limb loss, and in this setting, the risks of open surgical thrombectomy are acceptable. Nonetheless, the use of open surgical thrombectomy has waned since the risks exceed the benefits in most clinical situations. Clearly, if a less morbid alternative could be found that could provide results equivalent to those of open surgical thrombectomy, then it would be employed clinically on a much broader scale.
With the endovascular revolution of the 1980s and 1990s, the potential for percutaneous clot removal moved from theory into practice. Numerous devices were developed to facilitate clot removal, from simple suction catheters to elaborate mechanical devices for clot maceration. Although most of these devices were developed for the coronary market, many were better suited for the peripheral clot market, where the circulation remained more forgiving. These devices were variable in their success and were supported by limited data. Nonetheless, refinement of these adjuncts continues to the present.
The concept for mechanical adjuncts was quite simple: by combining rapid mechanical clot debulking with pharmacologic thrombolysis, faster recanalization could be achieved. Furthermore, in patients with relative or absolute contraindications to thrombolysis, mechanical clot debulking in association with anticoagulation alone provided clinical improvement without excessive risk of bleeding. Postsurgical patients with acute DVT can be anticoagulated, but pharmacologic thrombolysis is generally contraindicated. Percutaneous mechanical thrombectomy in combination with anticoagulation can debulk occlusive iliofemoral DVT to provide early restoration of venous flow and avoid valve destruction, even in the early postoperative period. Therefore, effective percutaneous mechanical thrombectomy held great potential for treatment of DVT in many clinical settings.
Of the mechanical devices available, perhaps the most experience in DVT has accrued with the AngioJet device (Possis Medical, Minneapolis, MN). This device combines alternating high-pressure irrigation with high suction, alternating at 60 times per minute. The resultant agitation of clot allows extraction of most acute thrombus and even allows removal by fragmentation of chronic thrombus elements. This device is currently approved by the US Food and Drug Administration for DVT treatment. A family of catheters allows selection of the appropriate size for the vein being cleared. Typically, the Xpedior 120 cm 6F catheter or the newer DVX 90 cm 6F catheter (Possis Medical) is used for treatment of DVT. Access is obtained in the popliteal or posterior tibial vein ipsilateral to the DVT. If necessary, contralateral femoral or great saphenous vein access can be used. The catheter is introduced over a 0.035-inch guidewire and passed to the area of clot. In most cases, the clot is extracted from the bottom upward, leaving the last few centimeters in the proximal vein until the end. This prevents release of emboli from the distal venous segment and avoids pulmonary embolus. After every two to four passes, contrast angiography is performed (Figure 2). For this, a three-way stopcock is inserted into the suction side of the catheter, allowing injection through the stopcock of contrast with removal from the body. If thrombolysis is being used, it can be delivered by power-pulse spray technique or by injection similar to the injection of contrast described above. In the power-pulse spray technique, the stopcock in the suction side is turned off while a concentrated thrombolytic mix is infused using the AngioJet pump. 31 This drives the thrombolytic agent deep within the clot, increasing the surface area for thrombolysis to occur.
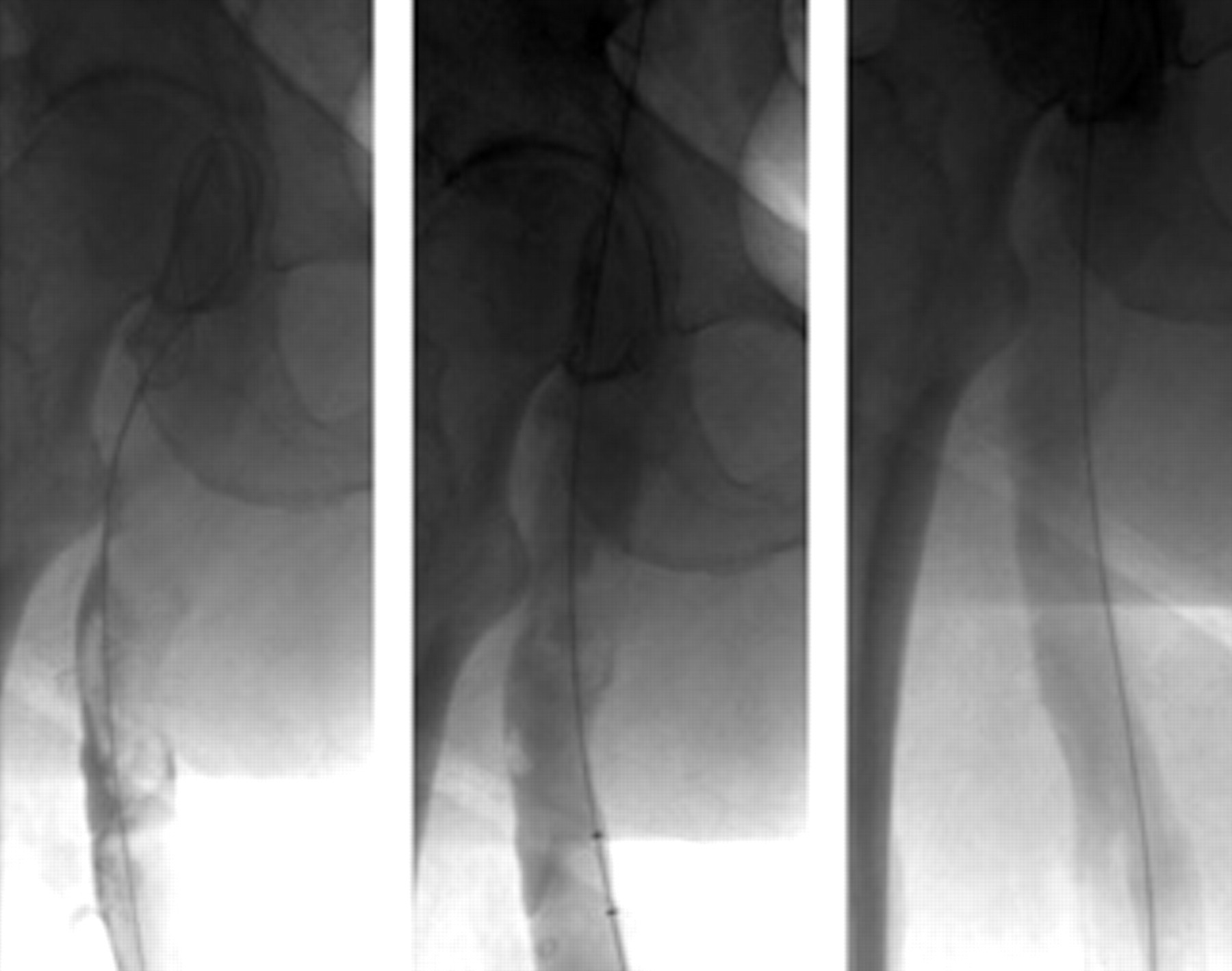
Consecutive AngioJet thrombectomy passes from left to right, showing the rapid clearance of clot in combination with tissue plasminogen activator. In the center panel, the AngioJet device is seen radiographically at the bottom of the image.
Kasirajan and colleagues reported the results of AngioJet thrombectomy in 17 patients who presented with extensive acute lower extremity DVT. 32 Greater than 90% of the thrombus was removed in 24% of patients with AngioJet alone and 76% required adjunctive thrombolytic therapy to achieve > 90% thrombus removal. Kim and colleagues reported that the combination of AngioJet mechanical thrombectomy with catheter-directed thrombolysis (CDT) significantly decreased intraoperative treatment time when compared with thrombolysis alone, and the combination of AngioJet and CDT costs significantly less than CDT alone since less lytic agent was required. 33 Cynamon and colleagues reported complete thrombus removal in 50% of patients treated with the power-pulse spray technique, with 100% clinical success when CDT was used as an adjunct. 34 Lin and colleagues reported compete thrombus removal in 75% of patients using the power-pulse spray technique, with a 68% 1 year primary patency rate. 35 There was also a significant decrease in overall hospital costs when compared with CDT alone ($47,742 vs $85,301; p < .01). 35
Usually, acute or subacute clot can easily be removed using this technique. In proximal DVT, a chronic component is often seen at the site of previous iliofemoral DVT. In May-Thurner syndrome, the proximal left iliac venous web is the source that will need further treatment (Figures 3 and 4), usually with a self-expanding stent. If the clearance of clot is inadequate and the patient is a candidate for thrombolysis, then infusion of a thrombolytic agent is performed via a coaxial multisidehole catheter to deliver thrombolytic agent over the length of the segment to be treated. Typically, the infusion is checked at about 12 hours to assess progress. In our experience, most infusions can be terminated by this time using the combined technique.

In this prone image, the left iliac vein is seen to be diffusely sclerotic secondary to previous deep venous thrombosis.
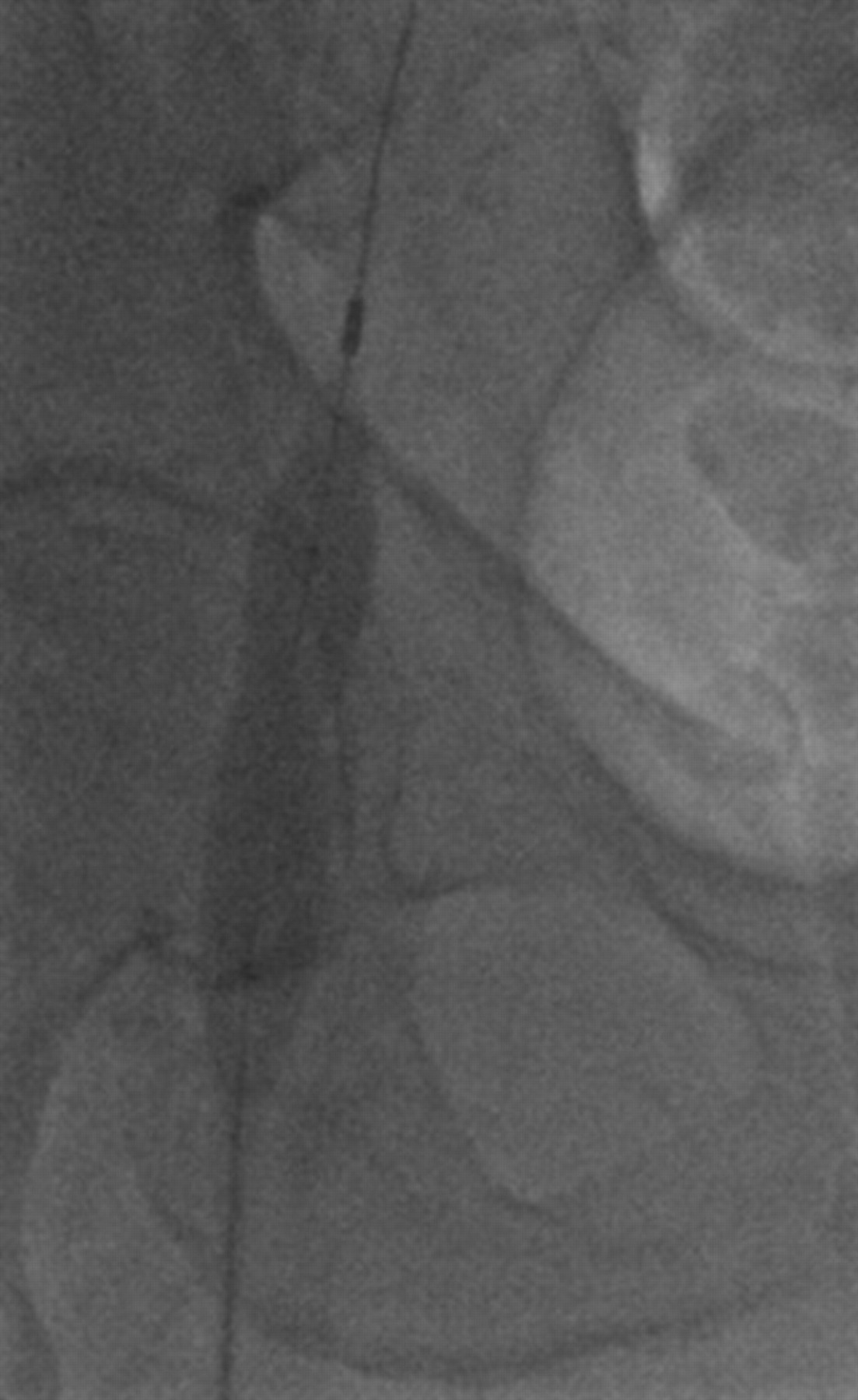
Angioplasty of the chronic venous stenosis restores patency.
Risks of Percutaneous Mechanical Thrombectomy
There are several risks associated with the use of percutaneous AngioJet thrombectomy, none of which are common, but all of which require some knowledge of the issues to prevent complications. Obviously, certain risks are inherent in the use of percutaneous devices, and these are no different with percutaneous thrombectomy. In fact, the combination with thrombolysis and anticoagulation likely leads to an increased risk of bleeding complications compared with conventional percutaneous procedures. 36 Although these bleeding complications clearly occur, they are rarely life threatening and usually can be managed by temporary reduction in the dosage of agents to allow hemostasis to occur.
Perhaps the most common complication associated with the use of percutaneous AngioJet thrombectomy is that of hemolysis. The AngioJet device creates high-force vortices, resulting in fracture of the red cell membrane with release of hemoglobin into the plasma. The degree of hemoglobin release is dose dependent, related to both the device used and the duration of use. Almost all patients experience some degree of hemoglobin release and resultant hemoglobinuria. 34 The main consideration here is to maintain adequate urine output by hydration and to decrease the risk of hemoglobin precipitation by alkalinizing the urine. Typically, sodium bicarbonate is added to the intravenous fluid to result in urine alkalanization to increase hemoglobin solubility. From the clinical perspective, the common mistake made by the managing team is to stop anticoagulation or thrombolysis owing to the “hematuria.” In reality, this is hemoglobinuria rather than hematuria, and the management should be to monitor urine output rather than stop anticoagulation. This lesson is repeated over and over in the clinical arena.
The maximum volume of suction effluent to prevent excessive hemolysis from the AngioJet device is variable depending on many factors. First and foremost is the choice of catheter. Smaller catheters that generate less turbulence result in less hemolysis and can be used for longer durations. On the other hand, the DVX catheter, which is commonly used for DVT, results in fragmentation of red cells to a much higher degree. For this reason, the treating physician needs to understand the differences between the catheters and adjust the duration and volume of effluent accordingly.
A second issue influencing the degree of hemolysis is the volume of blood flow while performing AngioJet thrombectomy. If the treatment is being performed in a relatively closed space, then little of the released hemoglobin will get into the systemic circulation. On the other hand, operating the AngioJet device in an open, flowing vein results in release of virtually all of the hemoglobin into the circulation. As a result, much of the AngioJet suction thrombectomy is typically performed prior to restoring systemic blood flow in the affected extremity. By limiting the volume of blood flow during the period of hemoglobin release, hemoglobinuria can be minimized to avoid renal dysfunction.
An additional complication seen with mechanical thrombectomy, particularly in the coronary circulation, is that of bradycardia with AngioJet use. Although the etiology of this effect is unclear and variable, the theory is that hemolysis can release adenosine from the red cell lysis and result in bradycardia. Dr. Biuckians has performed hundreds of peripheral AngioJet cases and has yet to be convinced that he has actually seen this complication. Reportedly, bradycardia as a complication is more common in the coronary and pulmonary circulations for unclear reasons.
Conclusions
The use of percutaneous suction thrombectomy devices holds great promise for future treatment, particularly with occlusive iliofemoral DVT. Although the long-term outcomes of pharmacologic thrombolysis and percutaneous mechanical thrombectomy remain poorly defined, these techniques hold great promise in preventing postphlebitic syndrome, particularly in proximal venous thrombosis. The exact anatomic distribution of clot that would benefit greatest from this therapy is currently unknown. Nonetheless, the potential for restoration of vein blood flow and preservation of valve function is truly the greatest step forward in the clinical management of DVT since the discovery of heparin.