
Abstract
Iliac venous outflow obstruction has an important role in the expression of symptomatic chronic venous insufficiency. This anatomic obstruction is frequently overlooked, owing in part to diagnostic difficulty. The combination of venous obstruction and reflux leads to more severe clinical disease. Current diagnostic modalities do not allow an definitive assessment of hemodynamically critical venous obstruction. No single invasive or noninvasive study can accurately detect borderline obstruction of potential hemodynamic significance. A high index of suspicion is critical in the initial recognition of chronic venous obstruction. The diagnosis relies on clinical signs and symptoms and radiologic assessment of morphologic venous outflow obstruction. Treatment strategy should be based on the results of morphologic investigations such as transfemoral phlebography or, preferably, intravascular ultrasonography. Percutaneous iliac venous stenting offers a safe and efficient method to correct pelvic venous obstruction. Percutaneous iliac stenting does not preclude subsequent venous bypass or corrective superficial and deep reflux surgery. This article reviews the etiologic factors and diagnostic modalities of iliac venous obstruction. The therapeutic role of percutaneous iliac stenting in the management of venous obstruction is also discussed.
Keywords
Percutaneous endovenous stenting has emerged during the last decade as the “method of choice” in the treatment of chronic obstruction of the femoroiliocaval venous outflow. It has replaced bypass surgery as the primary treatment. Open surgery is presently used only in selected cases of failed stent procedures or reocclusion of stents. Stenting of the iliofemoral veins guided by intravascular ultrasonography (IVUS) can be performed with low morbidity and mortality with appropriate technique. Overall the post-stent rate of thrombotic events is reported as 4 to 5%. 1,2 Late thrombosis of 982 stented iliac veins occurred in 3% of limbs 2 to 77 months after stenting. Overall cumulative primary, assisted primary, and secondary patency rates up to 72 months have been reported as 67 to 73%, 88 to 89%, and 90 to 93%, respectively. 1,2 The stent-related outcome was mainly related to the presence and severity of thrombotic disease. Primary and secondary patency rates dropped markedly from nonthrombotic limbs to thrombotic limbs with obstruction and to thrombotic limbs with occlusion (79 and 100%, 57 and 86%, and 54 and 74%, respectively). The cumulative severe (> 50%) in-stent recurrent stenosis rate remains low in the long term, 5 to 13% at 72 months. 1,2 Stenting of the iliofemoral vein appears to be durable. Patients have now been followed for more than 10 years with no precipitous decrease in patency observed.
The durability of the stenting is important since patients with chronic venous disease (CVD) are younger, will live longer, and have a better prognosis compared with patients with arterial atherosclerotic disease. CVD rarely threatens the survival of limb or patient. End points such as mortality, morbidity, and limb loss, therefore, poorly capture the treatment outcome of this disease. The goal is to improve symptoms and the quality of life (QOL). Hurst and colleagues showed resolution or substantial improvement in 72% of limbs, 1 and Hartung and colleagues reported a marked improvement in venous clinical severity and venous disability scores (median score decreased from 8.5 to 2.0 and from 2 to 0, respectively). 3
We recently reported a clinical follow-up of up to 8¾ years (mean 24 months, range 1–107). 2 A substantial improvement in limb pain and swelling, high rate of ulcer healing even in the presence of residual reflux, and enhanced QOL were observed. The beneficial clinical outcome occurred regardless of the presence of remaining reflux, adjunct saphenous procedures, or etiology of obstruction. The rate of limbs with severe pain (≥ 5 on a visual analogue scale of 0–10) fell from 41 to 11% after intervention; gross swelling (grade 3) in limbs decreased from 36 to 18%. After 5 years, overall, 62% and 32% remained completely free of pain and swelling, respectively. These numbers were based on complete relief of swelling and pain (grade 0 swelling and 0 level of pain) and did not reflect partial improvement. The incidence of ulcer healing after stent placement in 148 limbs with active ulcer was 68%, and the cumulative ulcer recurrence-free rate at 5 years was 58%. If healing of the ulcer was achieved after stenting, ulcer recurrence was rare within the study period.
It has previously been shown that both primary CVD with “simple” varicose veins and secondary CVD with development of post-thrombotic stigmata significantly reduce QOL. 4–6 Specifically, previous iliofemoral deep venous thrombosis (DVT) may cause clinically pertinent iliac outflow obstruction, resulting in a marked compromise of QOL. 7 A validated health-related QOL questionnaire has been used to assess the effect of stenting on subjective leg pain, sleep disturbance owing to leg problems, work-related leg problems, and the effect of leg symptoms on morale and social activities (CIVIQ). 8 There was significant improvement in all five problem categories after stenting of both nonthrombotic and thrombotic outflow obstructions. 2 CVD, regardless of etiology, affects QOL adversely, and stenting in patients with chronic venous outflow obstruction frequently markedly improves it.
Availability of a relatively simple and effective endovenous treatment with low morbidity and mortality has also led to a reappraisal of the role of venous outflow obstruction in the pathophysiology of CVD. The awareness of the possible presence of iliofemoral obstruction is increasing; consequently, the venous outflow is now evaluated more carefully and stenting is frequently considered. The major obstacle to further progress is a lack of precise criteria for selection of patients for stenting.
The degree of hemodynamic venous obstruction depends on multiple factors, for example, the number, location, degree of narrowing, and length of the lesions; development of collaterals; and the volume flow varying at rest and during exercise. Even the geometric form of an obstruction may change the pattern of blood flow. A slit-like narrowing of the lumen of a vein, even with no alteration in cross-sectional area, may increase resistance to flow. Any test to measure venous outflow obstruction must be identified as to whether it evaluates anatomic or functional aspects.
Hemodynamically Significant Venous Obstruction
The concept of a hemodynamically significant vessel obstruction being a stenosis of more than 70 to 80% is derived from observations on the arterial system. These conclusions are probably not applicable in the venous system since there are many fundamental differences. The venous circulation is a low-pressure, low-velocity, large-volume, and low-resistance converging vascular system (sewage draining system) compared with the high-pressure, high-velocity, small-volume, and high-resistance diverging arterial system (water supply system). A proximal arterial stenosis does not become significant until it meets and exceeds the level of the high peripheral resistance downstream. Contrarily, the iliac vein stenosis has to override only a low peripheral resistance and should, therefore, constitute a significant stenosis at a lesser degree. 9 It is presently not known, however, at what degree a venous stenosis is hemodynamically significant (Figure 1). Consequently, there is no accurate hemodynamic test, a gold standard, available to properly assess venous outflow obstruction and its improvement after stenting in individual limbs. Plethysmographic outflow fraction determination and pressure tests (hand-foot pressure differential, hyperemia-induced dorsal foot venous pressure increase) are global hemodynamic tests and may suggest obstruction to the venous outflow at any anatomic site and level, but significant blockage may exist in the presence of a normal result. 3,10,11 Positive tests may support further investigation and intervention, but a negative test does not exclude clinically significant venous outflow obstruction.
Images obtained by intravascular ultrasonography (IVUS). The black circle inside the vein (v) represents the inserted IVUS catheter. A shows evidence of early compression of the left common iliac vein by the right common iliac artery (a). B to D show a progressively significant compression at the left common iliac vessel crossing. The decision to intervene by iliac stent placement is largely judged by the location where most significant iliac vein compression is visualized.
Femoral venous pressure is a test for focal outflow obstruction. A pull-through pressure differential over a lesion or a pressure increase peripheral to the lesion with augmentation of venous inflow may be indicative of a significant stenosis. 12–14 The venous pressure is not only a function of resistance to the flow but is also dependent to a high degree on the flow velocity and magnitude of volume flow. It is unknown to what degree the resting venous flow must be increased to detect a functionally significant stenosis, and the method to reproduce this flow rate consistently is not available. Pressure gradients recorded in the venous system are much lower than in the arterial system, and only small pressure differentials may indicate significant obstruction. Studies suggest that a prestenotic pressure rise in the supine position greater than 2 to 4 mm Hg on provocation, a slow return to base level (> 30 seconds), or a gradient compared with the contralateral femoral pressure exceeding 2 to 5 mm Hg indicates a hemodynamically significant obstruction. 12–14 It has been suggested that a pressure differential on exercise should be at least 5 mm Hg to warrant intervention, but none of these pressure limitations have been validated. Treatment should not be limited to those limbs with increased pressures since good clinical results have been obtained treating morphologic obstruction with normal femoral venous pressure findings. 15
The accuracy of conventional hemodynamic tests is insufficient to detect borderline obstructions. They play only a limited role in the management of obstructive disease as a positive hemodynamic test may indicate hemodynamic significance, but a normal test does not necessarily exclude it. Clinical success can be achieved even in the presence of normal hemodynamic tests.
Morphologic Venous Obstruction
In lieu of an adequate hemodynamic test, morphologic tests must be used. Ascending venography after injection of contrast dye in a foot vein and antegrade transfemoral venography reveal the distribution and nature of the morphologic changes, including occlusion, stenosis, and presence of collateral circulation, but are inadequate to show any hemodynamic impact of visualized lesions. Ascending venography usually insufficiently visualizes the iliac vein to permit assessment of any obstruction of that segment. It is mainly used today as a preoperative mapping tool to delineate the inflow to a post-thrombotic iliac vein segment considered for stenting. To increase accuracy, all antegrade transfemoral venograms should be performed using arterial angiographic techniques with subtraction imaging, multiple oblique projections, and pressure injectors (Figure 2). With this technique, the quality of the images will improve and the contrast medium load will be minimal. A single-plane venogram was actually considered “normal” in at least one-fourth of limbs despite the fact that IVUS showed > 50% obstruction. 16 Interestingly, Cockett and colleagues made similar observations. Venography was diagnostic in only 65% of obstructed limbs in their material, and collaterals were visualized in only 63%. It was noted that in 54% of symptomatic patients, transfemoral venography appeared “normal,” with smooth contours of contrast in the iliac vein and without collaterals. The authors noted that absence of collateral formation should not negate consideration of the pathology. 17–19
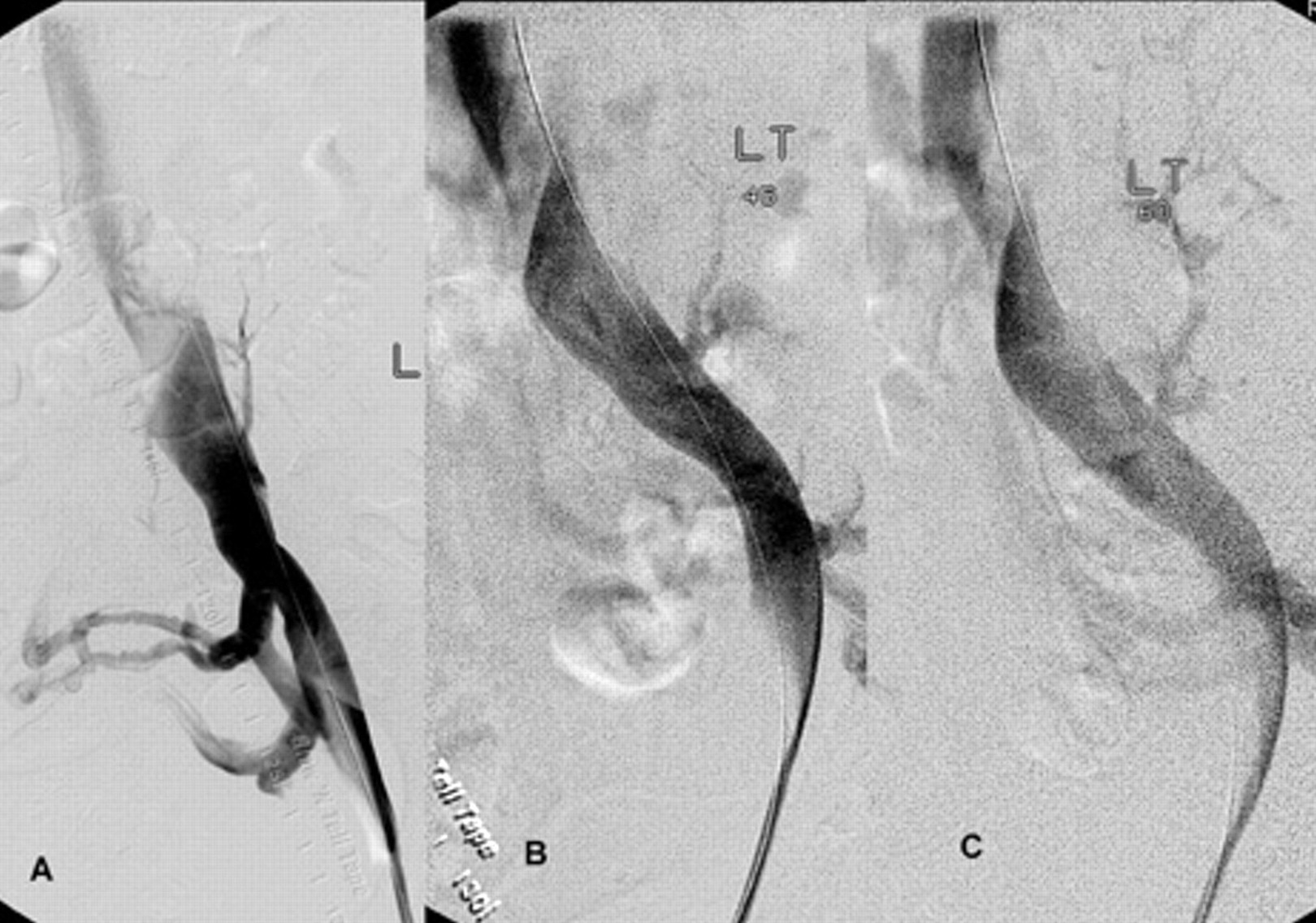
Left transfemoral venogram with multiple projections. The anteroposterior projection (A) shows compression of the common iliac vein with transpelvic collaterals. The oblique views of 45° rotation (B) and 60° rotation (C) better delineate the stenosis and the “corkscrew-like” compression by the artery transversing the vein.
Although the formation of collaterals is classically regarded as a compensatory mechanism to bypass and thus alleviate an obstruction, the mechanism and inducement of collateral formation are unknown. Collateral circulation shown prior to stenting is often not visualized following stenting of a venous stenosis. The flow through the stent is obviously favored (Figures 3 and 4). Although the pelvic collaterals may appear large on a venogram, they may be of little functional value. The flow is often retrograde owing to reversed valve orientation and impeded owing to the meandering course of the vessel. Interestingly, it has been shown by IVUS that the average iliac venous stenosis was tighter in the presence of collaterals than without. The rate of a significant obstruction as per preoperative pressure measurements was the same as in limbs with and without collaterals. 20 The rate of limbs with femoral pressure increase on intra-arterial injection of papaverine, suggesting a hemodynamic obstruction, was three times more common in patients with collaterals. It appears that a presumed increased flow through collaterals did not adequately compensate for the outflow obstruction in all instances. The prevailing view that collateral formation compensates for a venous outflow obstruction is, therefore, challenged. These observations support the concept of pelvic collateralization as an indicator of obstruction and that collaterals poorly compensate for the blockage in symptomatic patients.
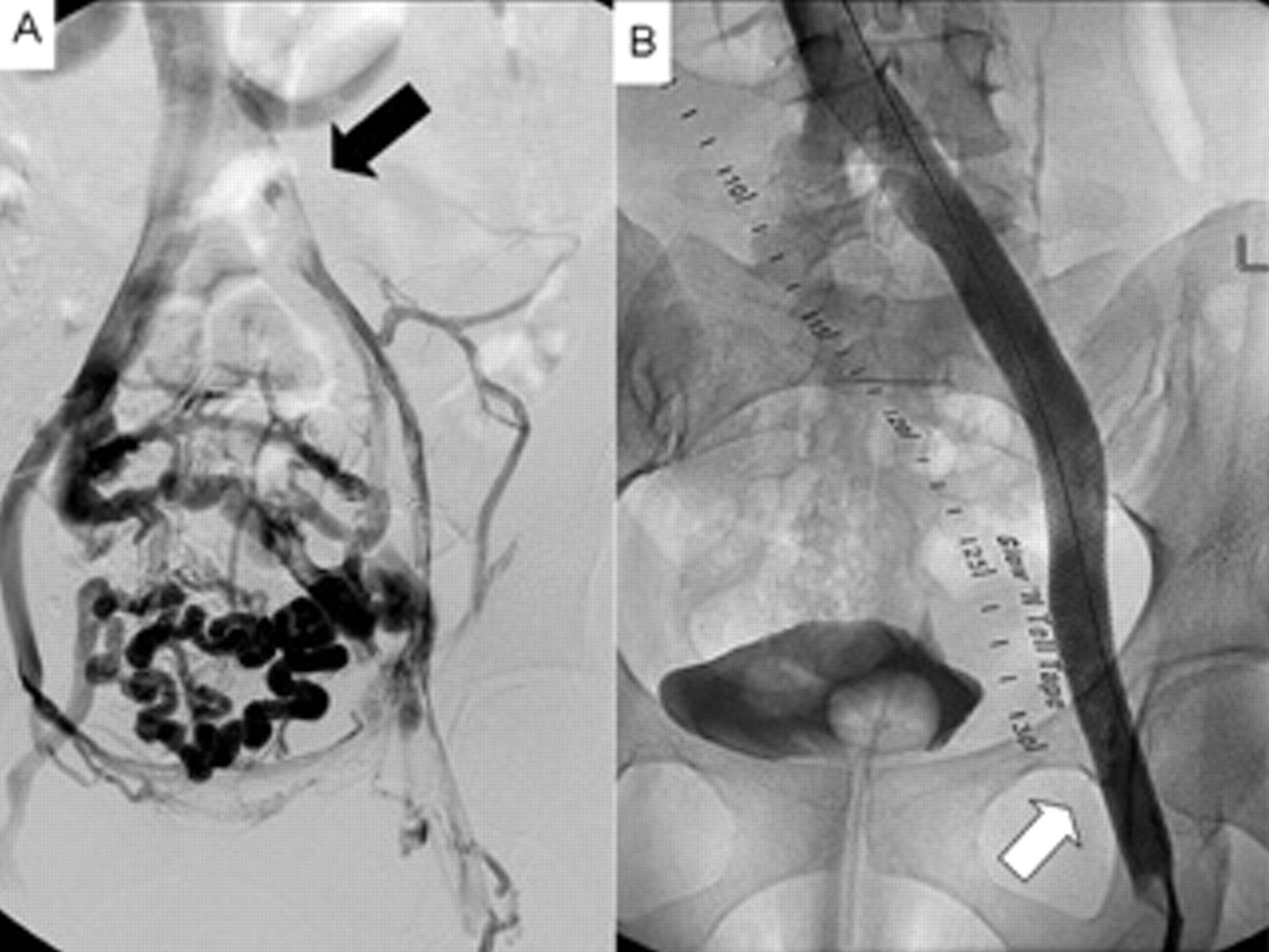
Chronic iliofemoral thrombotic obstruction before (A, black arrow) and after stenting (B). The stenting is carried into the common femoral vein (B, white arrow) to ensure an adequate inflow to prevent later occlusion. Note the nonfilling of the collateral circulation; the stent flow is obviously favored.
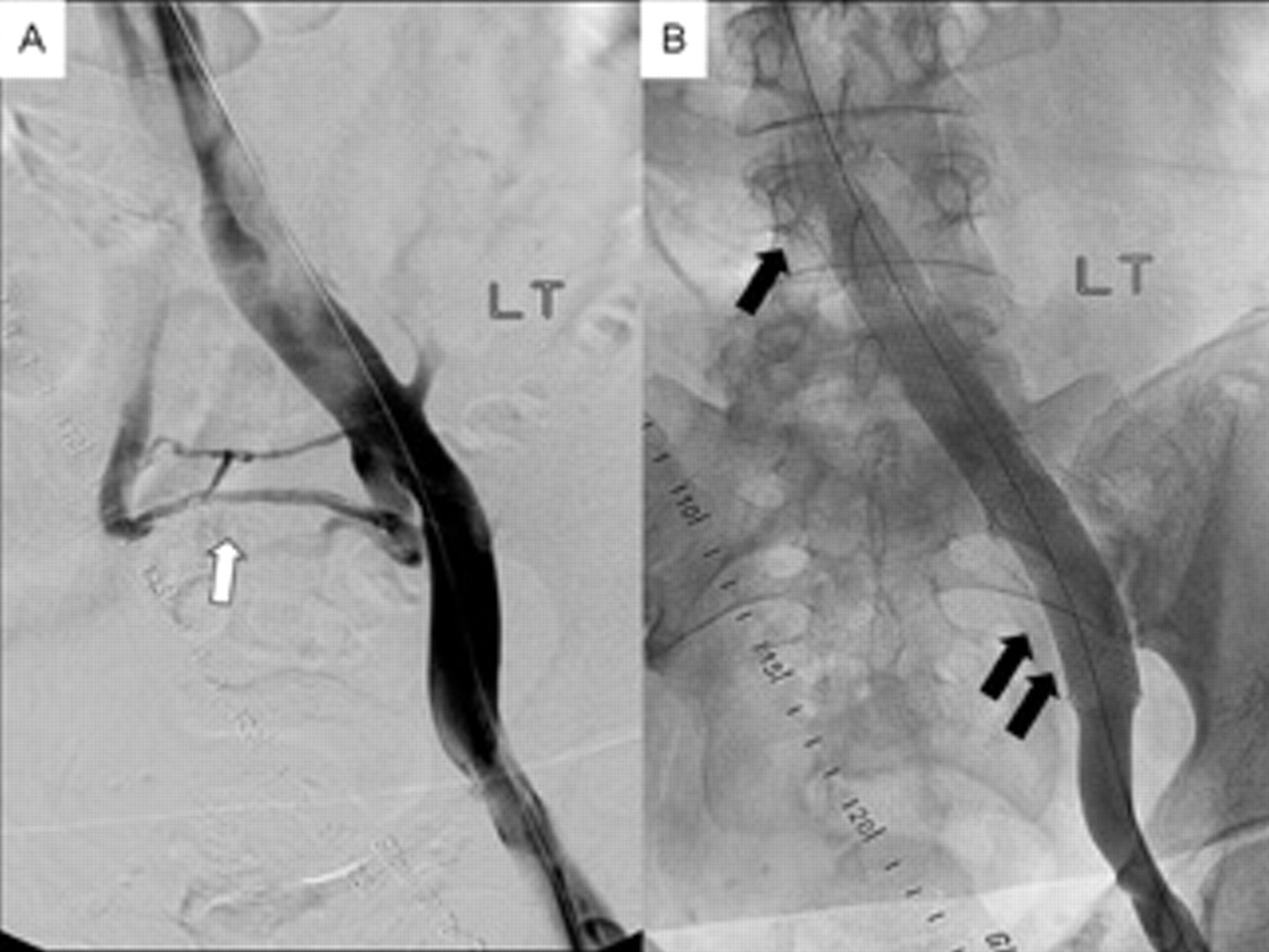
Transfemoral venogram (A) showing a typical nonthrombotic iliac vein lesion with prestent translucency at the vessel crossing and transpelvic collaterals (white arrow). Post-stent venogram (B) revealing no stenosis or collaterals. Note that the Wallstent (Boston Scientific, Natick, MA) is placed well into the inferior vena cava (B, single black arrow) to prevent retrograde migration. The stent is carried into the external iliac vein (B, double black arrows) since a significant stenosis was found on intravascular ultrasonography at the external and internal iliac vein confluence.
Ultrasound scanning of the iliac vein is under development but still lacks the adequate accuracy to detect partial obstruction or occlusion and to distinguish axial collaterals from the main stem veins. It can be used to evaluate patency of inserted stents. Spiral computed tomography (CT) and magnetic resonance venography are under evaluation and may replace transfemoral venography for screening in the future. Like ultrasound scanning, none of these tests have been validated.
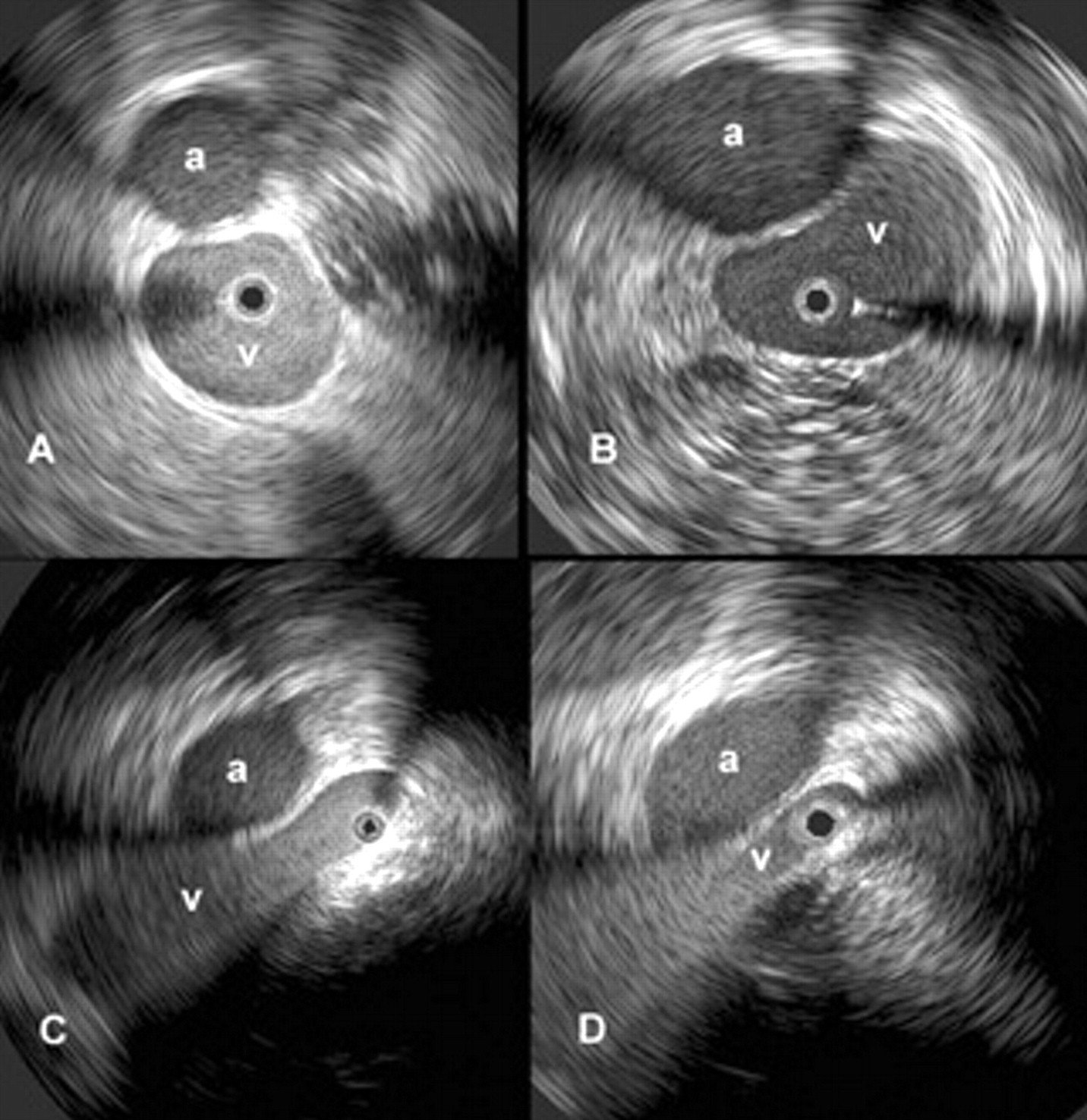
IVUS is superior to the single- and multiplane venography in detection of the extent and type of morphologic lesions of the vein. 20–24 It is the most accurate test in this aspect and should be used to validate findings of other morphologic imaging methods (Figure 5). IVUS better shows intraluminal details, for example, trabeculations and webs, which may be hidden in the contrast medium. Venous wall thickness, neointimal hyperplasia, and movement can be adequately assessed. An external compression with the resulting deformity of the venous lumen or post-thrombotic remodeling can be directly visualized. The degree of stenosis can be precisely calculated by measurement of the cross-cut areas and diameters of the normal and compressed or diseased veins using the software built into the IVUS apparatus. In addition to being a diagnostic tool, it is also a crucial aid in guiding stent insertion. Morphologic obstruction > 50% as measured by IVUS has arbitrarily been chosen for stenting. 1,25
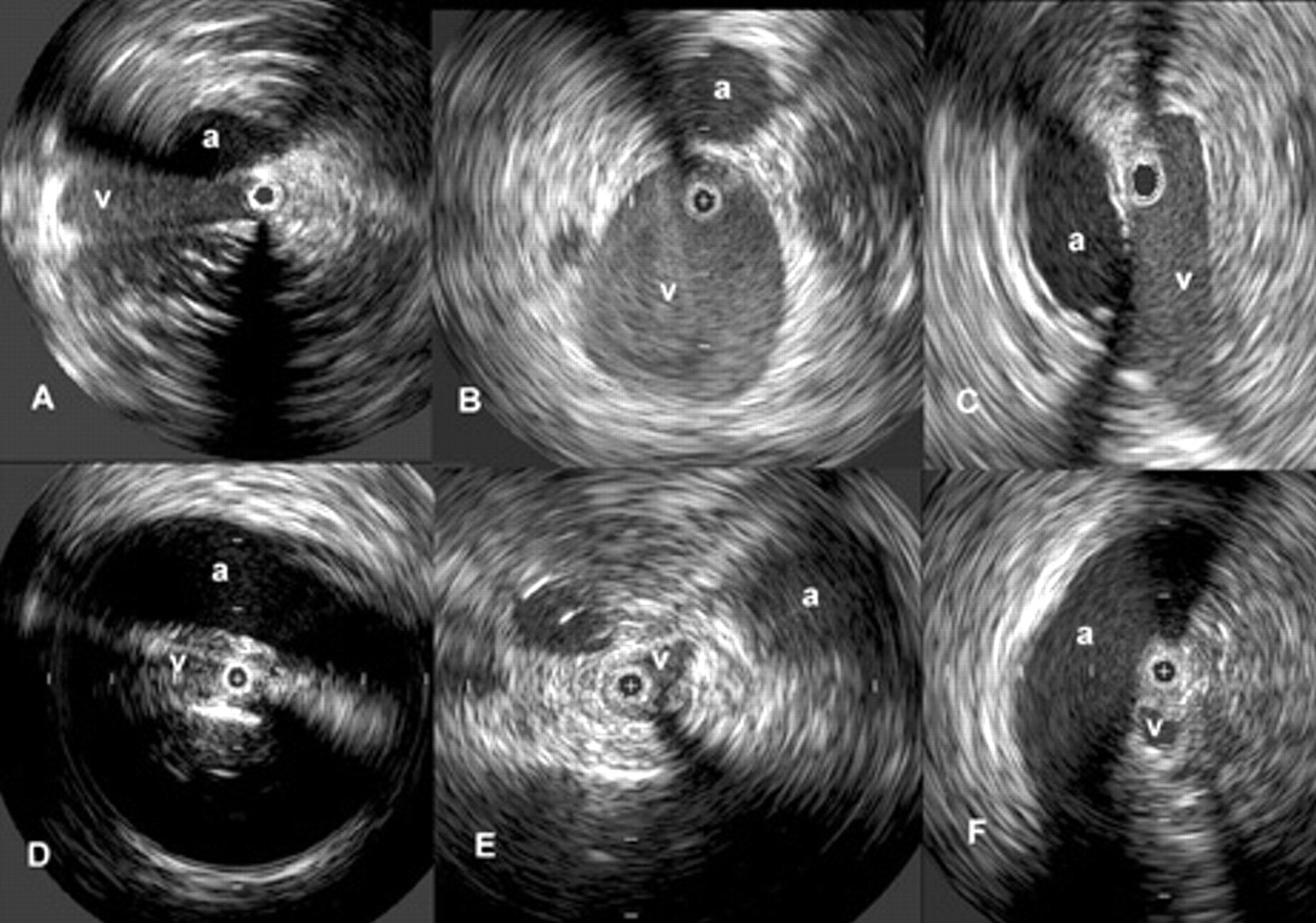
Images obtained by intravascular ultrasound (IVUS). The black circle inside the vein (v) represents the inserted IVUS catheter (a = artery). A to C are from a limb with nonthrombotic iliac vein compression (A, compression of proximal common iliac vein; B, normal distal common iliac vein; C, compression of the external iliac vein by the internal iliac artery). D to F are from a limb with chronic post-thrombotic obstruction (D, occluded compressed proximal common iliac vein at vessel crossing; E, obstruction of the distal iliac vein with an axial collateral. The border to the surrounding tissue is obscure owing to fibrosis; F, partially recanalized post-thrombotic occlusion of the compressed external iliac vein).
Etiology of an Obstructive Lesion
The typical post-thrombotic iliofemoral lesion often involves both common and external iliac veins with irregular stenosis or occlusions, and axial, transpelvic, and ascending lumbar collaterals are present (see Figure 3). Following acute iliofemoral DVT, only approximately 20% of the veins will completely recanalize on anticoagulation treatment, whereas the remaining veins recanalize partly and develop varying degrees of obstruction and collateral formation. 26,27 In the 1960s, Cockett and colleagues described venous outflow obstruction, compression of the iliac veins, and its relationship to thrombosis. 13,17–19,28 They observed that the obstructive lesion that precipitated the thrombosis impeded its resolution and the post-thrombotic perivenous fibrosis appeared to develop excessively at the initiating lesion site. Recently, this observation was confirmed by serial spiral CT-venography studies, which showed inhibited and incomplete recanalization in the presence of an external compression, for example, left iliac vein compression. 29 This observation is of great importance since it has been reported that 80% of limbs with iliofemoral DVT had underlying extrinsic iliac compression-type lesions revealed by the same technique (see Figure 5). 30
Even without thrombosis, iliac vein compressions are in themselves more pathogenic than previously thought, although they have been considered a common finding of little clinical importance. Previous studies have established the frequent findings of intraluminal and varying degrees of external compression of the iliac vein in the general population (22–33% 31–33 and 66–88%, 17,18,34 respectively). Although a nonthrombotic iliac vein compression lesion (NIVL) of the left proximal common iliac vein with secondary band or web formation is believed to be the most frequent finding in symptomatic limbs, involvement of both the common and the external iliac veins is, in fact, more commonly seen (see Figure 4). Using IVUS, compression of the common iliac vein has been reported in 36%, the external iliac vein in 18%, and both sites in 46% of symptomatic limbs (Figure 6). 19,35 In our experience of treating iliofemoral obstruction in 938 limbs in 879 patients, 53% of limbs had nonthrombotic compression lesions (defined as no history of DVT and no venographic or ultrasound findings indicating previous DVT), 40% had post-thrombotic obstruction, and 7% had a combined etiology. The ages of the patients with nonthrombotic blockage ranged from 18 to 90 years (median 54 years), 20% of patients were men, and 25% of the symptomatic lower limbs were on the right side. 35

Transfemoral ascending venograms showing different sites of nonthrombotic iliac vein lesions. A, typical compression of the left common iliac vein is seen here in an elderly woman with filling of the ascending lumbar vein; B, distal compression of the left proximal external iliac vein in the sagittal plane; C, compression of the right external iliac vein at the confluence of the internal and external iliac veins is noted by the distal right common and internal iliac arteries (arrow).
In lieu of hemodynamic tests, it may be intuitively easier to accept stenting a > 50% post-thrombotic obstruction than an NIVL on only morphologic grounds since the NIVL is frequently observed in the normal population. Nevertheless, the presence of an NIVL may be symptomatic and has previously been described as May-Thurner syndrome 31 or Cockett or iliac vein compression syndrome. 18 Why a silent lesion should suddenly become significant in the pathophysiology is not fully understood. It has been suggested that the NIVL is a so-called permissive lesion, which does not become clinically significant until other components of the venous circulation of the lower limb fail. There are many silent permissive lesions in human disease, for example, patent foramen ovale, which permits paradoxic embolic stroke, and, similarly, ureteric reflux and pyelonephritis, obesity and secondary diabetes, and carotid stenosis and transient ischemic attack. Correction of the permissive lesion alone often results in cure, even when the secondary pathology is not addressed. This may explain the surprisingly good results of venous stenting in CVD, even in the presence of untreated reflux. 35,36
Impact on Symptoms by Iliac Obstruction
Venous outflow obstruction plays an important role in the clinical expression of CVD, especially of pain. 36 Remaining obstruction is the principal cause of symptoms in approximately one-third of post-thrombotic limbs. 37,38 The iliac vein is the common outflow tract of the lower extremity, and chronic obstruction of this segment appears to result in more severe symptoms than does lower segmental blockage. Femoropopliteal venous obstruction appears to be better compensated for by collateral formation than obstruction of the iliac and common femoral veins. 39,40 The clinical expression is influenced by any concomitant deep or superficial reflux. In addition, it has been demonstrated that persistent obstruction of proximal veins is associated with progressive distal vein incompetence. 41,42 It is well recognized that the combination of reflux and obstruction gives the highest levels of venous hypertension and the most severe symptoms compared with either alone. 43,44 Negus and colleagues suggested that limb swelling and pain were related to the obstructive component, whereas limb ulceration resulted from valve reflux. 19 It has been shown that ulcers occur rarely in the presence of isolated iliofemoral obstruction (3%) but more often when obstruction is associated with reflux (24%). 36 A substantial number of patients with CVD complain of disabling pain and swelling of the lower limbs without skin changes. It is possible that these symptoms are mainly attributable to obstruction rather than to reflux. Five years after iliofemoral DVT is treated conservatively with anticoagulation, 90% of patients suffer symptoms of CVD. Debilitating venous claudication is found in 15 to 44% of patients, and venous ulcer has developed in 15% of limbs. 7,26 Venous claudication is a dramatic condition described as an exercise-induced “bursting” pain, which requires several minutes of rest and sometimes leg elevation to achieve relief. Certainly, patients with significant outflow obstruction may also have less distinct lower extremity pain and discomfort with decreased QOL and moderate disability. As discussed above, stenting of the venous outflow obstruction resulted in major symptom relief in patients with CVD. The beneficial clinical outcome occurred regardless of the presence of remaining reflux or etiology of obstruction.
When to Stent
The major obstacle for precise selection of patients for venous outflow stenting is the lack of a reliable test to measure a hemodynamically significant stenosis. The key for the physician is to be aware of the importance and possibility of venous blockage combined with increased suspicion in patients with a history and clinical signs and symptoms suggestive of outflow obstruction. Patients with previous DVT; patients with limb symptoms, especially pain, out of proportion to detectable pathology; patients not improving on conservative treatment; and patients with no other detectable pathology to explain their symptoms are specifically targeted. Although a positive noninvasive or invasive test may support further studies, a negative test should not exclude them. The diagnosis and treatment must presently be based on invasive morphologic investigations of the iliac venous outflow, although hemodynamic criteria would be preferred. When algorithms are constructed for workup of patients with significant CVD, morphologic investigation of the outflow must be included. Limiting workup of these patients to only duplex ultrasonography will not suffice, especially not when restricted to the infrainguinal vein segments. IVUS investigation is the ultimate test and should be generously used in symptomatic patients with suspicion of outflow obstruction. Morphologic obstruction > 50% as measured by IVUS has arbitrarily been chosen for stenting, with gratifying clinical results. Stenting specifically alleviates pain and swelling and promotes sustained ulcer healing. Most importantly, the QOL of the patients is significantly improved. It can be performed with low morbidity, no mortality, a long-term high patency rate, and a low rate of in-stent restenosis. Endovenous stenting is, therefore, the current method of choice in the treatment of chronic venous obstruction.
Stenting is a minimally invasive outpatient procedure and results in marked clinical improvement whether or not an adjunct procedure to control superficial reflux is performed. In the presence of combined iliac vein obstruction and superficial or deep reflux, therefore, the emerging course of treatment is primarily to correct the obstructive component. When significant great saphenous vein reflux is present, the great saphenous vein has increasingly been obliterated by percutaneous technique at the time of the stenting. 45 Any concomitant deep venous reflux should be addressed later if necessary.