
Abstract
Open surgical repair of iliac aneurysms has been usually associated with significant morbidity and mortality. The introduction of novel endovascular techniques has expanded the currently available options to treat these aneurysms. However, the use of endoluminal stent grafts to treat common iliac artery aneurysms by landing their distal end into the hypogastric artery in patients where flow into the latter artery is crucial to avoid end-organ ischemia has only been rarely reported in the past. A case report of a common iliac aneurysm case treated with a novel therapeutic approach, not previously reported is herein presented. Three telescopically-overlapping Hemobahn/Viabahn polytetrafluoroethylene (PTFE)-covered endoprosthesis (W.L. Gore & Associates, Flagstaff, AZ) were used with success.
Large aneurysms of the iliac arteries are relatively uncommon lesions that require surgical repair to prevent rupture. Open surgical repair of these aneurysms has been traditionally associated with major morbidity and mortality. 1,2 More recently, endovascular techniques have expanded the therapeutic horizon, especially for patients at high risk for open interventions. In selected cases, endovascular repair of these aneurysms requires interruption of the circulation to the hypogastric arteries. This is often well tolerated if unilateral, with preservation of the contralateral hypogastric flow. However, bilateral interruption of antegrade hypogastric artery flow during endovascular aneurysm repair may be associated with significant morbidity, including buttock claudication or gluteal muscle necrosis, erectile dysfunction, and ischemia of the sigmoid colon and perineum. 3 Such complications prompted vascular endovascular surgeons to be creative and modify the already existing endovascular tools and techniques to accommodate the different clinical situations encountered.
A challenging common iliac aneurysm case treated with three telescopically overlapping Hemobahn/Viabahn polytetrafluoroethylene-covered endoprostheses (W.L. Gore & Associates, Flagstaff, AZ) is presented and a novel therapeutic approach that has not been previously reported is described.
Case Report
We recently evaluated a 58-year-old man whose past history was significant for hypertension, coronary artery disease, a soft tissue sarcoma that required radiation therapy, and a left hemipelvectomy 19 years ago. The left external iliac artery was interrupted during the latter operation as this constitutes a standard and essential step of a hemipelvectomy procedure. He also had a history of lung cancer, which required a right lower lobe resection 22 years previously. He was “disease free” from both malignancies. His referral was prompted by the incidental computed tomographic scan finding of a 3.8 cm left common iliac artery aneurysm (Figure 1). Given his multiple comorbidities, an endovascular approach was proposed. He underwent a preintervention angiogram that demonstrated no pelvic cross-filling from the right hypogastric artery (Figure 2). Therefore, an endovascular exclusion of the left common iliac artery aneurysm with maintenance of antegrade left hypogastric arterial perfusion was performed using covered stent grafts with an up-and-over approach from the right common femoral artery. The procedure was uneventful, and the patient was discharged without immediate complications.

Computed tomographic scan showing an aneurysm located in the left common iliac artery that measured 3.8 cm in maximum diameter as an incidental finding. Note postsurgical changes in the left pelvis consistent with a history of left hip disarticulation for a left lower extremity malignancy.

Preintervention, early-phase angiography with balloon occlusion of the left common iliac artery origin and selective injection of the right hypogastric artery, demonstrating lack of cross-filling from right to left. Late films did not demonstrate cross-circulation either. This led us to think that flow preservation through the left hypogastric artery was essential to avoid pelvic ischemic complications.
Technique
Under fluoroscopic guidance and sterile technique, the right common femoral artery was accessed percutaneously and a 6F vascular access sheath was placed. A marker pigtail catheter was advanced over a wire into the proximal abdominal aorta, contrast was injected, and abdominal aortography was performed. The catheter was then repositioned into the distal abdominal aorta, above the bifurcation, contrast was injected, and pelvic angiography was performed (Figure 3).

Abdominal and pelvic aortography showing previous ligation of the left external iliac artery (after left hip disarticulation) and a widely patent right hypogastric artery but a lack of crossover pelvic collaterals. Sheath and wire access have been established for endovascular intervention.
Using an Omni-flush catheter (Angio Dynamics, Queensbury, NY), a glidewire (Boston Scientific, Natick, MA) was advanced and a Kumpe catheter (Cook, Bloomington, IN) was used to reposition the wire more distally into the anterior division of the left hypogastric artery. Then the Kumpe catheter was advanced, and the glidewire was removed and exchanged for a stiff Amplatz exchange-length wire (Cook, Bloomington, IN).
The catheter and the existing vascular access sheath were removed and a 9F sheath was placed over the aortic bifurcation into the proximal left common iliac artery (see Figure 3). An 8 mm × 5 cm Viabahn stent was advanced over the wire and deployed into the internal iliac artery, above its bifurcation. The stent was then dilated using a 6 mm × 4 cm balloon dilation catheter (Figure 4).

Deployment of the first Viabahn stent (8 mm × 5 cm), which was deployed into the left internal iliac artery, above its bifurcation. The stent was then dilated using a 6 mm × 4 cm balloon dilation catheter.
At this point, the existing vascular access sheath was removed over the wire and a 12F vascular access sheath was placed over the bifurcation, with its tip in the left common iliac artery. A Kumpe catheter was used to exchange the existing wire for a 0.025 Platinum Plus wire (Boston Scientific, Natick, MA).
Next, a 10 mm × 5 cm Viabahn stent was advanced over the wire and deployed into the left common and internal iliac arteries and the initial, distally placed covered stent, with approximately 50% overlap, using the telescoping technique. An 8 mm × 6 cm balloon dilation catheter was advanced, and angioplasty within the proximal stent was performed (Figure 5).

Deployment of the second Viabahn stent (10 mm × 5 cm), which was deployed proximal to the first stent with a 50% overlap. This stent was dilated using a 8 mm × 6 cm balloon dilation catheter. Note that the wire and the sheath have been exchanged for those that allow the advancement and deployment of larger sizes of Viabahn stents.
Then a 13 mm × 5 cm Viabahn stent was advanced over the 0.025 inch wire and deployed into the left common iliac artery, with its proximal end at its origin and the distal end telescoped into the 10 mm × 5 cm stent. The wire was removed through the Kumpe catheter, and using a Rosen wire and a pseudo-“Waltman loop,” the left common iliac artery stent was angioplastied using a 10 mm × 4 cm balloon dilation catheter. Contrast injection demonstrated an excellent angiographic result (Figure 6), with complete common iliac aneurysm exclusion and maintenance of left hypogastric arterial flow. The catheter and vascular access sheath were removed, and hemostasis was obtained by manual pressure. There were no immediate complications.
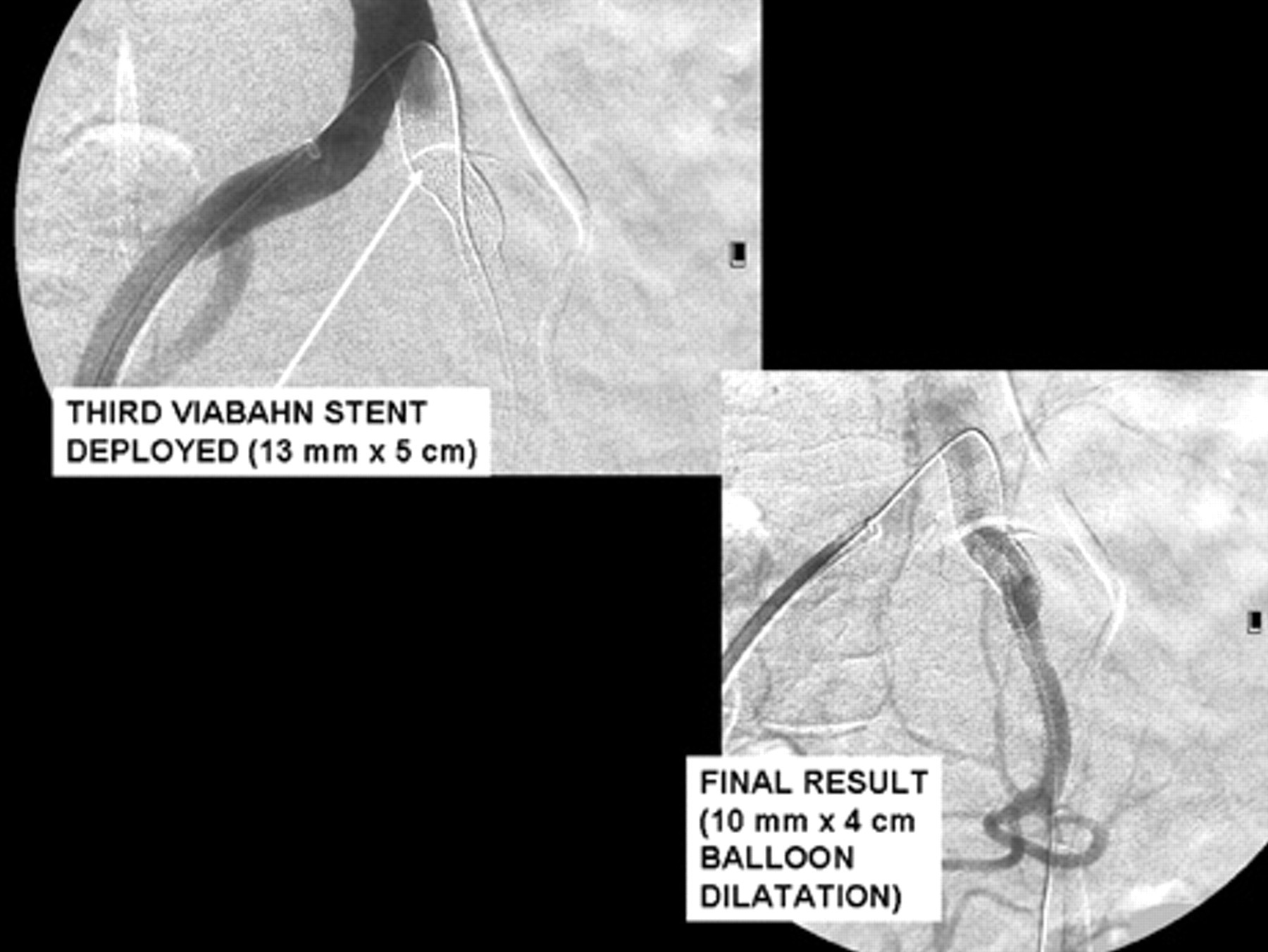
Final angiographic result after endovascular exclusion of a left common iliac artery aneurysm after deploying a third Viabahn covered stent graft (13 mm × 5 cm) with its proximal end at the origin of the common iliac artery.
Discussion
Iliac artery aneurysms are well known to be difficult to diagnose and to manage. They have been traditionally associated with high operative mortality rates in reported series. 1,2 These observations prompted the search for alternative techniques with lower mortality and morbidity rates. Percutaneous techniques were then developed; however, their durability and effectiveness when compared with direct surgical repair have been questioned. 2 Our current work reports for the first time a novel endovascular technique and augments the currently available armamentarium for treating iliac artery aneurysms in complex, high-risk patients.
The short- and midterm results of endoluminal stents to treat iliac artery aneurysms are favorable. 4–6 Therefore, several alternatives (hybrid 7,8 or pure endovascular) to open surgery have been reported for cases in which maintenance of pelvic circulation on one side is crucial to avoid potentially serious ischemic complications. In the case of our patient, initial consideration was given to coil embolization of the left hypogastric artery as definitive therapy for this aneurysm, especially with his history of a previous left hip disarticulation. It was thought that with a widely patent contralateral hypogastric artery, his pelvic organs would not suffer a major impact from the flow interruption of the left hypogastric artery. However, concerns were raised with regard to the effect of the left hemipelvectomy and radiation therapy on the pelvic collateral circulation. To reassure ourselves that coil embolization of the left hypogastric artery was the therapy of choice, preintervention diagnostic angiography was performed, selectively injecting contrast into the right hypogastric artery with simultaneous balloon occlusion of the proximal left common iliac artery. This maneuver demonstrated a complete lack of pelvic collateral cross-filling from right to left. The patient's left pelvic arterial flow therefore was completely dependent on the left hypogastric artery blood supply. On clinical examination, he still had sufficient left gluteal and pelvic soft tissue mass to suggest to us that the occurrence of soft tissue ischemia and gangrene would be severely deleterious for this patient. The potential for colonic ischemia was also obviously an issue of major concern if the left pelvic circulation were to be interrupted.
Moreover, it has been previously shown that branches of the ipsilateral external iliofemoral artery system provide important ipsilateral pelvic arterial collateral pathways of potentially greater hemodynamic significance than the contralateral hypogastric artery. 9 This patient's left external iliac artery had been ligated previously as part of the hemipelvectomy, thus eliminating this important potential source of compensatory collateral development. Because of all of these considerations, maintenance of left hypogastric perfusion was felt to be of critical importance in this patient.
A great deal of creativity is needed to apply the currently available endovascular devices to the anatomic configuration of the aneurysm, especially when an open approach is thought to be associated with a high risk of complications. This patient's history of previous pelvic surgery and radiation therapy prompted us to consider a purely endovascular approach as the option of choice, avoiding all surgical incisions if possible. We proposed a modification of a technique that Delle and colleagues used to treat patients with aortoiliac aneurysms. 10 A step of their technique involved hypogastric artery catheterization from a left brachial artery access and placement of a flexible stent graft deployed from the distal end of an abdominal aortic aneurysm stent graft limb into the hypogastric artery. To our knowledge, this is the only report of an endoluminal stent used to treat a common iliac artery aneurysm, by extension of its distal end into the hypogastric artery. De Baere and colleagues used a covered endovascular stent to treat a patient who had a bleeding iliac artery pseudoaneurysm and had undergone radiation therapy and surgery for pelvic malignancies. 11 We chose a contralateral femoral approach given that our patient had a normal right femoral pulse and no radiation damage to the right pelvis. Moreover, the type and size of the stent graft that we planned to use required the placement of a 12F sheath, which would have been associated with significant potential for arterial damage if a percutaneous brachial artery approach would have been used. Another key difficulty in this case resulted from the major diameter discrepancy between the common iliac artery (about 11 mm) and the distal hypogastric artery (about 6 mm). Tapered stents of such a size reduction are not currently commercially available. Therefore, a “telescoping” stent graft technique was used, overlapping progressively larger stents in a stepwise, gradual manner from distal to proximal, to successfully exclude the common iliac aneurysm. The latter technique has not been previously reported.
Conclusions
The introduction of endovascular therapies to treat aneurysmal disease of the iliac arteries greatly broadens the therapeutic possibilities, which is especially important in patients at high risk for open surgical intervention. In circumstances in which major morbidity from exclusion of the hypogastric artery flow is of significant clinical concern, endovascular repair of common iliac aneurysms using covered stent grafts extending from the common iliac artery into the hypogastric artery is a safe and effective technique with good short-term results. This approach should be considered in patients with medical, surgical, or anatomic contraindications to open surgical repair. The short-term results are favorable; however, long-term follow-up of these procedures is warranted to assess the durability of the repair and the absence of complications.