
Abstract
The factor V Leiden (FVL) mutation has been demonstrated to be associated with the development of venous thrombosis in humans. Whether such a propensity also exists in the arterial circulation remains controversial. In an effort to minimize the variability that clouds the clinical study of arterial thrombosis, we studied FVL-associated arterial thrombosis in an experimental model of homozygous, heterozygous, and wild-type mice. Heterozygous FVL mice were crossbred to C57BL/6J mice over several generations. The genotypes of the resulting three genotype groups (wild type, heterozygous FVL, and homozygous FVL) were blinded to the investigators. Arterial injury was produced with the injection of ferric chloride into an isolated segment of carotid artery. Arterial thrombosis was assessed with an ultrasonic flow probe and the time to occlusion (TTO) was recorded. The carotid artery occluded within 60 minutes of injury in 72 of the animals studied (97.3%). The carotid artery remained patent at 60 minutes in the remaining two animals, both of whom were subsequently found to be genotypically wild type. There was a statistically significant relationship between TTO and genotype (p = .002). TTO was greatest in the wild-type mice (p < .001 vs heterozygous, < .001 vs homozygous) and least in the homozygotes (p < .001 vs heterozygotes). Increased thrombogenicity is present in mice with the FVL mutation and is more prolonged in homozygotes than heterozygotes. These findings provide some corroboration to the clinical studies that suggest an increased risk of arterial events in patients with the FVL mutation.
Protein C is one of the key regulatory proteins in the coagulation cascade. Activated protein C (APC) is an antithrombotic protein that cleaves and inactivates factor Va and VIIIa, thereby inhibiting the coagulation cascade. Resistance to APC has been described in some patient groups with deep venous thrombosis (DVT), 1,2 documented to be due to a point mutation in the gene encoding factor V (Arg506-Gln), 1–8 also called the factor V Leiden (FVL) mutation. As a result of this point mutation, APC is unable to cleave factor Va and inhibit the coagulation cascade, resulting in a lifelong procoagulatory condition with an increased risk of thrombosis in humans. The FVL mutation has been shown to be the most occurring risk factor, known to date, for hypercoagulability.
Studies have documented APC resistance owing to FVL in 20 to 60% of patients with DVT. 3 By contrast, the impact of the FVL mutation on arterial thrombogenicity remains ill-defined. We hypothesized that APC resistance on the basis of FVL mutation may predispose to thrombosis following vascular injury. Recently, mice have been generated carrying heterozygous (FvQ/+) and homozygous (FvQ/Q) factor V mutations. 9 We chose to use this animal model of FVL to determine whether this genotypic variant predisposes to the development of arterial occlusion following vascular injury.
Materials and Methods
Animals
All experimental procedures were approved by The Cleveland Clinic Foundation Animal Committee on Use and Care of Laboratory Animals. Knockout mice carrying the FVL mutation, as previously described, were used. 9,10 Two pairs of heterozygous FVL mice were obtained (Dr. David Ginsburg, University of Michigan, Ann Arbor, MI) and were crossbred to C57BL/6J mice for more than eight generations. The offspring comprising the three genotype groups (wild type, heterozygous FVL, and homozygous FVL) were blinded to the investigators (Table 1). On reaching adulthood (32–52 weeks of age, weight 25–30 g), the animals were anesthetized (intraperitoneal pentobarbital, 120 mg/kg) and placed on a warm blanket maintained at 37°C (Figure 1) using an experimental set-up previously described. 11–16 The common carotid artery was exposed through a midline cervical incision and was isolated using a dissecting microscope with digital imaging capabilities. An ultrasonic flow probe (Model 0.5VB, Transonic Systems, Ithaca, NY) was positioned around the common carotid artery and the vessel was bathed in 0.9% sodium chloride solution to allow continuous flow monitoring using data acquisition software (WinDaq, DataQ Instruments, Akron, OH).
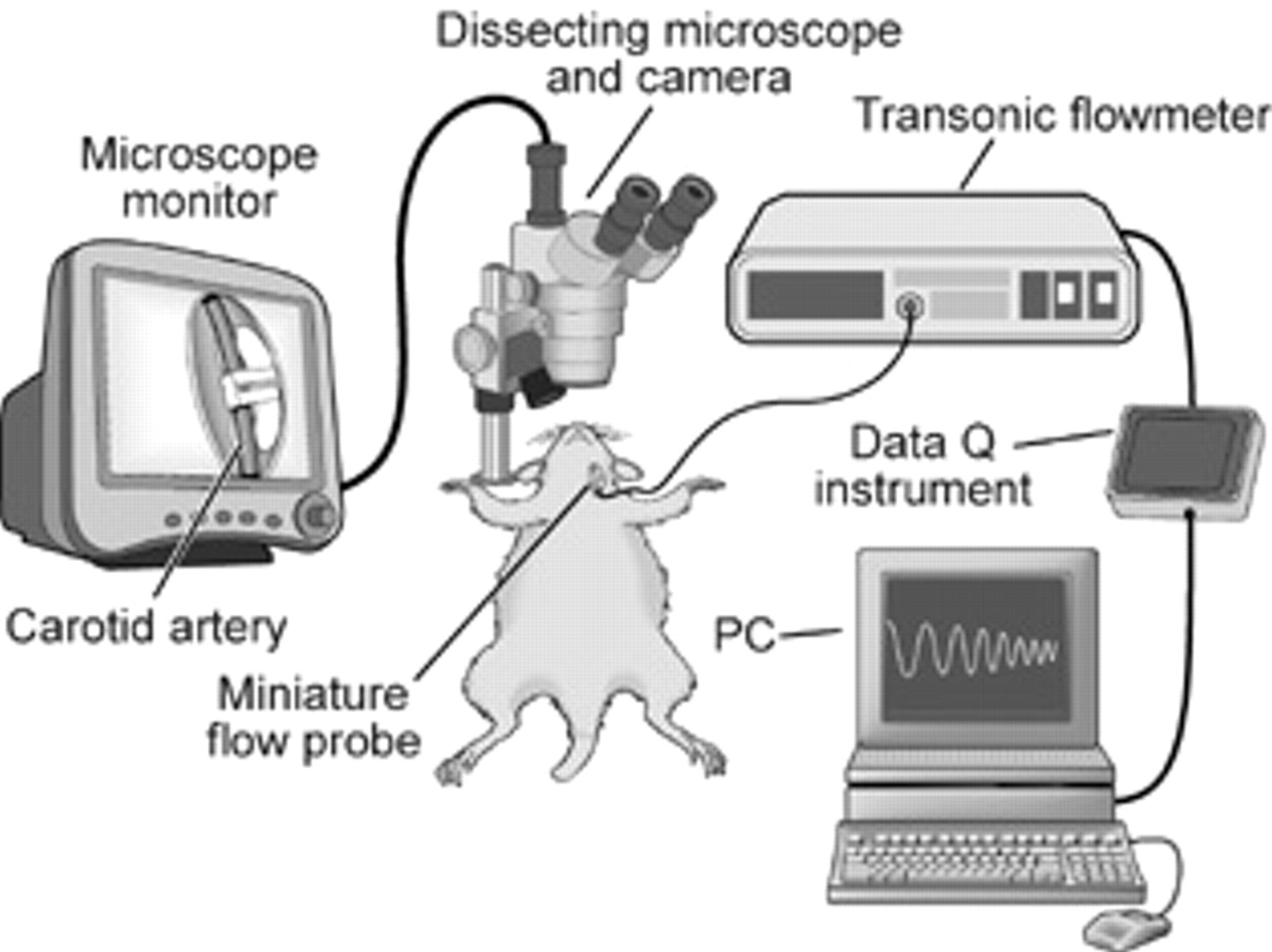
The experimental study set-up. Reprinted with the permission of The Cleveland Clinic Center for Medical Art & Photography® 2008. All rights reserved.
Frequency of the Three Genotypes in the 74 Animals Bred to Adulthood
Endothelial Injury
The sodium chloride solution was removed from the wound and filter paper (0.5 × 1.0 mm) saturated with 10% ferric chloride (FeCl3) was applied to the adventitial surface of the carotid artery at a point immediately proximal to the flow probe. The filter paper was removed after 3 minutes and saline was replaced in the wound. Carotid blood flow was continuously monitored and the time to occlusion (TTO) was defined as the duration between removal of the FeCl3 filter paper and the cessation of flow. The experiment was terminated after 60 minutes in animals that did not develop occlusion. The pathophysiology of FeCl3 vascular injury has been described. 16
Genotype
At the end of each experiment, the toes and the tail of each mouse were amputated, frozen, and stored for future genotyping. Genotyping was performed on the frozen tail tissue with polymerase chain reaction as previously described. 11
Statistical Analyses
Differences in the actual versus expected genotype frequencies were assessed with the chi-square test. The statistical significance of differences in TTO between the various groups was assessed with the Student t-test to compare two groups and with one-way analysis of variance (followed by pairwise post hoc comparison) when multiple groups were compared. A two-tailed p value of less than .05 was considered significant.
Results
Seventy-four offspring were successfully bred to adulthood and underwent genotypic analysis. By genotypic analysis, 33.8% were wild type, 59.5% were heterozygous, and 6.8% were homozygous for the FVL mutation (see Table 1). These frequencies were significantly different from the expected ratio of 25% wild type, 50% heterozygotes, and 25% homozygotes (p = .001), suggesting a link between early mortality and the homozygous genotype.
Overall, 72 of 74 animals occluded the carotid vessel within 60 minutes of FeCl3. The two animals that did not develop occlusions were subsequently demonstrated to be genotypically wild type. The TTO differed among the three genotypes (p = .002; Table 2). TTO was greatest in the wild-type mice (p < .001 vs heterozygous, < .001 vs homozygous) and least in the homozygotes (p < .001 vs heterozygotes).
Time to Occlusion in the Three Genotype Groups
CI = confidence interval; FVL = factor V Leiden; TTO = time to occlusion.
Discussion
Dahlback and colleagues first described APC resistance in 1993. 1 Knowledge of this abnormality, related to a mutation that is associated with abnormal factor V, has grown tremendously since then. FVL is now described as the most occurring genetic risk factor for vascular thrombosis. 2–4,7,8 Patients heterozygous for FVL exhibit a fivefold increase in the rate of thrombosis. 17 In homozygotes, the risk is dramatically increased to as much as 80 times that of the general population. 17 But in contrast to a solid association between FVL and venous thrombosis, the data relating FVL and arterial events remain controversial. Nevertheless, some clinical studies suggest an increased risk of thrombosis after arterial revascularization, 18–25 implicating vessel wall injury during the revascularization procedure as the triggering event. Not unexpectedly, the relationship between FVL and failure of arterial reconstructive procedures appears especially high in homozygotes. These findings are not universal, however, and several studies have failed to detect a solid relationship between FVL and arterial occlusion. 26–28
Paradoxically, clinical studies have preceded basic investigation on FVL and arterial occlusion. Noting the paucity of well-controlled experimental data, we sought to investigate the relationship between FVL and arterial thrombosis in a knockout animal model. Systematic back-crossbreeding produced 22 wild types, 44 heterozygotes, and 5 homozygotes. These frequencies differed substantially from the expected mendelian inheritance frequencies of 25%, 50%, and 25%, respectively. During the breeding process, there were many perinatal deaths. The genotype of these animals was not tested since the blinding dictated by the experimental protocol did not allow knowledge of animal genotypes during the experiment. Nevertheless, it is quite likely that many of the deaths occurred in homozygotes, a contention consistent with the known association between human FVL and spontaneous abortion. 29–32 Our frequencies would suggest an 80% perinatal mortality rate in homozygotes, and previous studies demonstrated widespread multiorgan thrombois in FVL mice that died during the perinatal period. 10
Our study documented more rapid vascular thrombosis in the setting of FVL and arterial injury. This finding was more prominent in homozygous mice compared with heterozygotes. A recent study by Eitzman and colleagues, using rose Bengal, found similar results to our study. 33 Although clinical data have been conflicting, with some studies demonstrating an increase in the risk of arterial events and others not, the well-controlled laboratory setting minimized variability and confirmed the relationship between FVL and arterial thrombosis. Noting the importance of APC and the role of factor V in intrinsic anticoagulation, an increased risk in FVL mice was not unexpected.
This finding has clinical relevance; the presence of FVL would be anticipated to be a risk factor for such arterial events as in situ thrombosis over an atherosclerotic plaque or occlusion of a vascular reconstructive procedure. It raises the question of whether patients with FVL develop arterial complications in the presence of more mild disease. For instance, are FVL patients more susceptible to cerebral embolization in the setting of a lower-profile carotid bifurcation plaque? Are patients with lesser degrees of restenosis at the site of a coronary or peripheral arterial stent more likely to develop occlusion? These and other clinical questions can be answered only by thoughtful, well-designed clinical studies; our experimental findings serve only to stimulate the performance of clinical analyses. Until such data are available, clinicians should maintain a high index of suspicion for FVL in patients with failed arterial reconstructions. As well, one should have a lowered threshold for the use of periprocedural antithrombotic therapy in patients with known FVL.