
Abstract
The objective of this study was to determine the prevalence of significant carotid artery disease (SCAD) in a cohort of Egyptian patients to compare it with matched groups of patients in published data of Western populations. One thousand consecutive patients referred for color flow duplex scanning of the carotid arteries were included. SCAD was defined as carotid stenosis ≥ 50% or occlusion. There were 567 males (56.7%), and the mean age was 60.4 years. There were 382 (38.2%) patients presenting with and 617 (61.7%) patients without specific carotid territory symptoms. SCAD was significantly more prevalent in patients aged ≥ 60 (13.2%, vs 6.25%; p < .001), in symptomatic patients (16.45% vs 6.32%; p < .001), in diabetics (15.96% vs 7.39%; p < .001), in patients with ischemic heart disease (17.65% vs 7.22%; p < .001), in hypertensive patients (12% vs 7.54%; p = .025), and in patients with dyslipidemia (12.53% vs 6.56%; p < .025). The prevalence of SCAD in this cohort of Egyptian patients was similar to that of matched patients of Western populations. Screening for SCAD in patients with specific carotid territory symptoms is recommended. Screening of asymptomatic subjects could be considered if they are ≥ 60 years of age and have three or more associated risk factors.
Stroke places a heavy financial burden on society. 1–4 Significant proportions of patients who suffer cerebral infarction die or suffer severe long-term disability as a result of their illness. 5–10 Most cerebral infarctions occur without previous warning signs in previously asymptomatic patients. 11,12 Carotid artery disease is considered to be the underlying cause of cerebral infarction in 20 to 30% of patients. 13–15 By identifying and appropriately treating carotid artery disease, many cerebral infarctions could be prevented. Color flow duplex scanning (CFD) is highly accurate in identifying carotid artery disease. 16–20 CFD is a noninvasive study, relatively inexpensive, and therefore suitable as a screening test for the identification of significant carotid artery disease (SCAD). 21,22
It was previously shown that Chinese patients have a higher incidence of intracranial disease and a lower incidence of significant extracranial carotid artery disease compared with Western populations. 23 It was extrapolated from these data that Egyptian patients and perhaps Middle Eastern patients may have a lower incidence of SCAD compared with Western populations. The prevalence of SCAD among Egyptian patients or other Middle Eastern populations has never been assessed before. The objective of this study was to determine the prevalence of SCAD in a cohort of Egyptian patients, to compare it with matched groups of patients in published data of Western populations, and to define which subgroups of patients are at high risk of developing SCAD, for whom screening would be justified.
Methods
Institutional review committee approval was obtained. All patients referred for CFD were enrolled in the study starting from January 2004. The study was completed in January 2006 by the enrollment of 1,000 consecutive patients. Patients were referred through their primary care physicians. Patients were not specifically referred to be enrolled in this study but rather followed the local referral pattern, based on clinical grounds. Patients were referred for CFD if they had specific carotid territory symptoms or nonspecific cerebral symptoms or prior to surgical coronary revascularization procedures. Data were collected prospectively regarding age, gender, risk factors, symptoms, and CFD findings. The following were considered risk factors: diabetes mellitus (DM), ischemic heart disease (IHD), hypertension, smoking, and dyslipidemia. The presence of each risk factor was determined by patient questioning and by reviewing the patient's hospital records. Patients were considered to have IHD if they had a history of IHD or underwent operative or percutaneous coronary revascularization. Patients were considered hypertensive if their blood pressure was > 140/90 mm Hg or were taking antihypertensive medications. Patients were considered smokers if they were current smokers. Patients were considered to have dyslipidemia if they had an elevated cholesterol level (> 200 mg/dL), elevated low-density lipoprotein (> 130 mg/dL), or elevated triglycerides (> 150 mg/dL) or were taking lipid-lowering agents.
Patients were considered “symptomatic” if they had specific carotid territory symptoms: transient ischemic attack reversed neurologic deficit, stroke, amaurosis fugax, and central retinal artery occlusion. Otherwise, patients were considered “asymptomatic.”
CFD was performed by highly experienced operators (W.T. and N.W.) using high-end dedicated cardiovascular equipment: ATL-HDI-3000 (Philips/Advanced Technology Laboratories, Bothell, WA, and Philips Medical Systems, Eindhoven, The Netherlands) and HP Sonos-7500 (Philips Medical Systems, Andover, MA). Bilateral CFD of the carotid and vertebral arteries was performed for all patients. Duplex findings were classified into the following categories: normal or < 50%, 50 to 69%, or 70 to 99% occluded. The degree of stenosis was calculated according to the hemodynamic parameters described by Strandness 24–27 and reported according to the European Carotid Surgery Trial method. 28–30 SCAD was defined as carotid stenosis > 50% or occlusion.
Data were prospectively maintained in a computerized database. SPSS statistical software (SPSS Inc, Chicago, IL) was used for analysis. Statistical comparisons were performed with the chi-square test. Analysis of variance was used to compare means. Multivariate analysis was performed to determine the risk factors responsible for SCAD using stepwise multiple logistic regression analysis, and r 2 was used to indicate the strength of the association between the risk factors. A p value ≤ .05 was considered statistically significant.
Results
One patient was found to have an aneurysm of the extracranial internal carotid artery and was excluded from further analysis. The following analysis therefore concerns the remaining 999 patients.
Demographic Data
There were 567 males and 432 females (56.7% male, 43.2% female), and their mean age was 60.4 years (range 10–93 years, median 62.0 years); 568 patients were aged ≥ 60 years.
Risk Factors
The distribution of risk factors was as follows: 599 (59.9%) patients were hypertensive, 389 (38.9%) patients were smokers, 391 (39.1%) had dyslipidemia, 331 (33.1%) were diabetic, and 283 (28.3%) had IHD. Three hundred eighty-two (38.2%) patients had specific carotid territory symptoms, whereas 617 (61.7%) patients did not have specific carotid territory symptoms. The breakdown of patients with specific carotid territory symptoms is as follows: amaurosis fugax and central retinal artery thrombosis, 26 (2.6%); transient ischemic attack, 190 (19%); and stroke, 166 (16.6%).
Significant Carotid Artery Disease
Half of the patients (50.6%) were found to have normal carotid arteries, 391 (39.1%) had < 50% stenosis, 42 (4.2%) had 50 to 69% stenosis, 42 (4.2%) had 70 to 99% stenosis, and 18 (1.8%) had occluded internal carotid arteries. Therefore, 10.2% of the patients (102 of 999) had SCAD.
Data Analysis
The prevalence of SCAD (defined as ≥ 50% stenosis or occlusion) was analyzed in each subgroup of patients. SCAD was significantly more prevalent in patients aged 60 years or older, patients who complained of specific carotid territory symptoms, “symptomatic patients,” diabetic patients, patients with IHD, hypertensive patients, and patients with dyslipidemia. There was no statistically significant difference in the prevalence of SCAD between smokers and nonsmokers and between males and females Table 1.
Prevalence of Significant Carotid Artery Disease in Relation to Risk Factors
HTN = hypertension; IHD = ischemic heart disease; NS = not significant; SCAD = significant coronary artery disease.
The prevalence of SCAD in symptomatic patients aged ≥ 60 years was 20.6% in diabetics, 26.4% in patients with IHD, 19.8% in hypertensive patients, 22.2% in patients with dyslipidemia, and 12.5% in smokers.
The prevalence of SCAD in asymptomatic patients aged ≥ 60 years was 17.4% in diabetics, 15.8% in patients with IHD, 10.6% in hypertensive patients, 9.8% in patients with dyslipidemia, and 11.3% in smokers.
The prevalence of SCAD in symptomatic patients increased with the increase in the number of associated risk factors present: age < 60 years, 13.0%; age ≥ 60 years, 18.9%; and age ≥ 60 years plus one risk factor, 20.6%; plus two risk factors, 25.5%; plus three risk factors, 27.5%; and plus four risk factors, 33.3%. The prevalence of SCAD in asymptomatic patients increased with the increase in the number of associated risk factors present: age < 60 years, 2.6%; age ≥ 60 years, 9.4%; and age ≥ 60 plus one risk factor, 17.4%; plus two risk factors, 24.5%; plus three risk factors, 25%; and plus four risk factors, 36.8% (Figure 1).
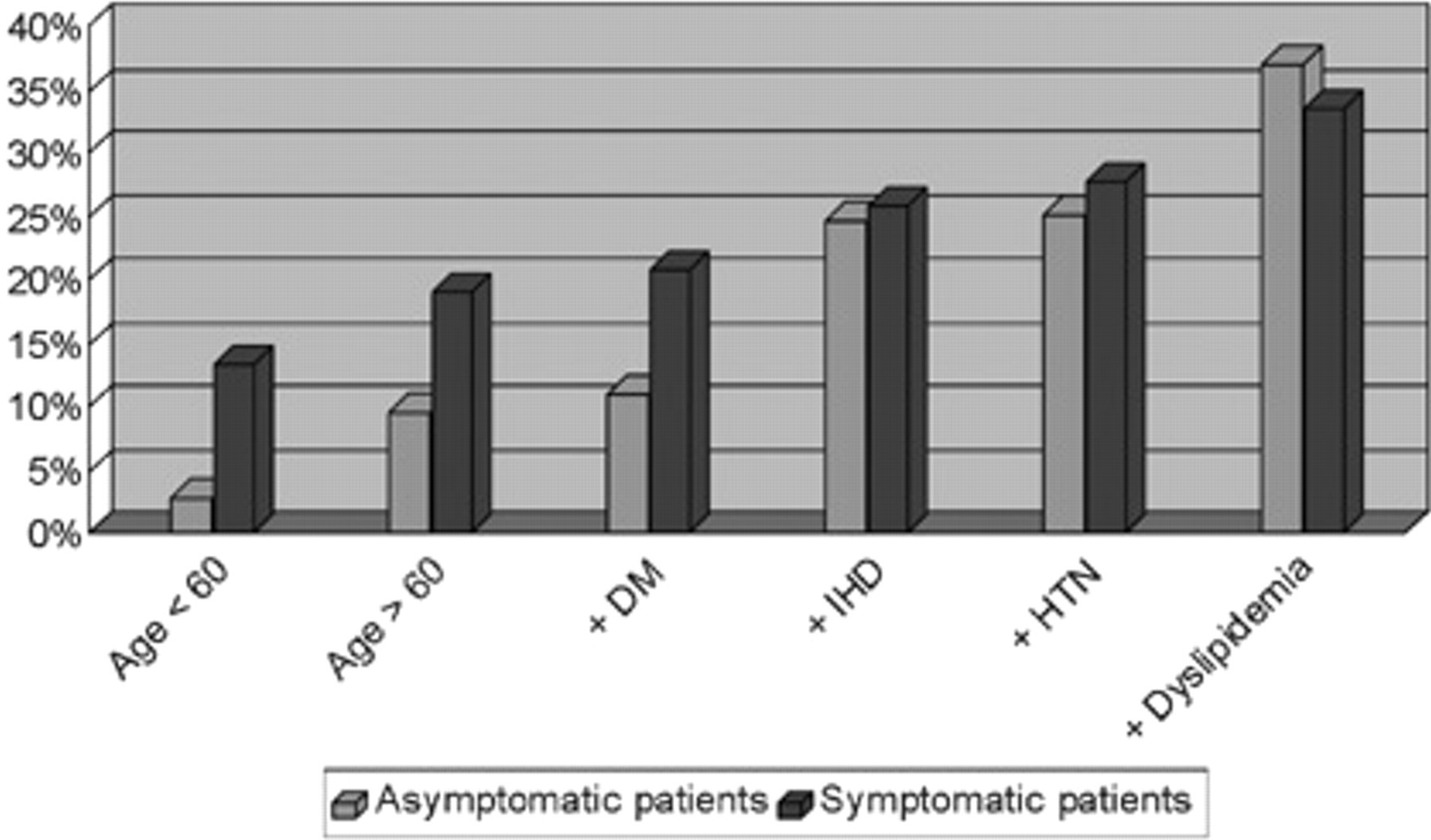
Prevalence of significant carotid disease in symptomatic and asymptomatic patients in relation to risk factors. The third columns represent age ≥ 60 + one risk factor (diabetes mellitus [DM]), the fourth represents age ≥ 60 + two risk factors (DM + ischemic heart disease [IHD]), etc. HTN = hypertension.
Multivariate analysis was performed to determine the significant independent predictors of SCAD. Multivariate analysis with a stepwise multiple logistic regression model was performed. All variables that approached statistical significance at univariate analysis with a p value ≤ .5 were included in the multivariate analysis; r 2 indicated the strength of association between SCAD and the variables. Age showed the strongest association with SCAD. Specific carotid territory symptoms, IHD, DM, and dyslipidemia were independent predictors of SCAD (Figure 2).

Strength of association between significant carotid artery disease and the risk factors. The numbers in percent represent the value of r 2, which was calculated by stepwise logistic regression analysis (p < .05). The first column represents one risk factor (age ≥ 60 years), the second represents two risk factors (age + SYMPT), etc. DM = diabetes mellitus; DYSLIPID = dyslipidemia; IHD = ischemic heart disease; SYMPT = specific carotid territory symptoms.
Discussion
It is estimated that 20 to 30% of strokes in the United States are caused by extracranial carotid artery disease. 14,31,32 Appropriate early management of this condition can prevent future strokes. 33,34 Previous studies identified subgroups of patients at high risk of developing SCAD in Western populations. 35–38 The prevalence of SCAD was shown to be affected by race. 23,39 To our knowledge, no previous studies have been performed to determine the prevalence of SCAD among a large cohort of Egyptian or Middle Eastern patients. This study was performed to assess the prevalence of SCAD among specific subgroups of Egyptian patients, to compare these data with previously published data of Western patients, and therefore to identify patients in whom duplex screening would be most effective in identifying SCAD. This is important not only in our country but also in many Western countries in which there are large numbers of expatriates of Middle Eastern origin.
Comparison with Western Populations
Jacobowitz and colleagues studied the prevalence of occult SCAD in a group of 394 asymptomatic patients aged ≥ 60 years old who had one or more of the following risk factors: hypertension, heart disease, current smoking, and family history of stroke. 38 The prevalence of SCAD in their study was 1.8% in the absence of risk factors, 5.8% with one risk factor, and 13.5% with two risk factors. The prevalence of SCAD in a comparable group in our study, patients aged ≥ 60 years who had no specific carotid territory symptoms, was 9.4% in the absence of risk factors, 10.5% in the presence of hypertension, and 17.4% in the presence of hypertension and IHD.
In a community-based study, Rockman and colleagues compared the prevalence of SCAD in patients aged ≥ 60 years with and without hypertension. 37 The prevalence of SCAD in their study was 12.7% versus 7.8%, respectively, compared with 10.5% versus 7.4% in a comparable group in our study. Similarly, the prevalence of SCAD in the Rockman and colleagues study in patients with and without heart disease was 18.2% versus 8% 37 compared with 15.7% versus 6.2% in a similar group in our study.
Our findings are in agreement with previous publications showing that patients with IHD and hypercholesterolemia are more prone to develop SCAD. 36
Although hypertension showed a significant association with SCAD on univariate analysis, it was not significant in the multivariate model, a finding similar to that of Qureshi and colleagues. 36
SCAD was not significantly associated with smoking in our study. This finding is in agreement with a previously published study that showed that association with smoking is affected by race, being strong among white patients and less strong among black patients, and there was no association among Hispanics. 40
These data suggest that the cohort of patients included in our study had a very close prevalence of SCAD to comparable cohorts of patients in Western studies. It could therefore be assumed that current practice in Western populations is also applicable to our population.
Screening of Symptomatic Patients
The prevalence of SCAD was relatively high in symptomatic patients (16.49%). This justifies routine screening in all symptomatic patients, regardless of age and the presence of other risk factors. This is in accordance with current practice for Western populations 41 and should be implemented in our population.
The prevalence of SCAD in symptomatic patients increased with the increase in the number of risk factors present (see Figure 1). Therefore, it appears prudent to screen all patients who present with specific carotid territory symptoms, in particular those whose age is ≥ 60 years and/or those who have one or more associated risk factors.
Screening of Asymptomatic Patients
In a review of current evidence regarding cost effectiveness, it was concluded that if screening for asymptomatic carotid artery stenosis is conducted in a subpopulation with a prevalence of SCAD of 20% or greater, screening can reduce the risk of stroke in a cost-effective manner. 42
In a recent publication of guidelines for screening of extracranial carotid artery disease sponsored by the American Society of Neuroimaging and the Society for Vascular and Interventional Neurology, it was recommended that although “screening of the general population or a selected group based on age, gender, or any other variable alone is not recommended, screening of selected subpopulation aged ≥ 65 years with at least 3 cardiovascular risk factors needs to be considered.” 42
The prevalence of SCAD in our group of asymptomatic patients was low (6.32%). However, the prevalence increased with the increase in the number of risk factors present. The prevalence was 25% if age was ≥ 60 years and in the presence of three risk factors (see Figure 1). Therefore, it appears appropriate to apply practice guidelines for screening of asymptomatic patients in Western populations to our population.
Our study is not a community-based study but rather a study of a cohort of 1,000 consecutive patients referred to have CFD. The prevalence of SCAD in the general community is very low; therefore, studying a sample of the community has been shown not to be cost effective. Previous authors who studied the prevalence of SCAD put inclusion criteria to enhance the cost effectiveness of their studies, most importantly minimum age and the presence of one or more risk factors. 37,38 In our study, all consecutive patients referred for CFD were included; there were no exclusion criteria. It therefore allowed for the study of subgroups of patients with various characteristics and for the comparison of subgroups of patients in our study with matched patients in Western studies who had similar age and risk factors.
Conclusions
Our data suggest that the prevalence of SCAD in our patients is similar to that of Western groups of patients with comparable age and risk factors, therefore showing no obvious racial difference. The prevalence of SCAD showed a significant association with age, specific carotid territory symptoms, IHD, DM, hypertension, and dyslipidemia. Screening for SCAD in patients with specific carotid territory symptoms is recommended in Middle Eastern populations, much like Western populations. Screening of asymptomatic subjects may be considered if they are ≥ 60 years of age and have three or more associated risk factors.
Footnotes
Acknowledgment
We acknowledge Amal S. Ibrahim, MD, DrPh, professor of epidemiology at the National Cancer Institute, for conducting the statistical analysis.