
Abstract
Carotid artery stenting is gaining wider acceptance as an alternative option in the treatment of carotid artery stenosis. Conventional complications such as stroke and recurrent in-stent restenosis are well documented in the literature. However, we believe that carotid stent complications are underreported. The carotid artery segment has features that are relatively smilar to the femoropopliteal segment with respect to forces affecting the stented segment, which can contribute to stent complications such as fracture. In this article, we present a case of internal carotid artery stent fracture and thrombus formation after the patient was exposed to direct trauma to the chest and neck.
Carotid artery angioplasty and stenting (CAS) is gaining wider acceptance as an alternative to carotid endarterectomy (CEA) for the treatment of carotid artery stenosis in certain patient populations. Acceptable indications for carotid stenting include high-risk patients with multiple comorbidities, patients with an inaccessible lesion for surgery, recurrent carotid stenosis after previous CEA, and radiation-induced carotid stenosis. 1 Most studies concentrate on early and late complications of CAS related to stroke rates and restenosis while ignoring complications related to stent–artery interactions that can lead to changes in stent configuration or fracture.
Stent fracture has been reported to occur in areas with flexible arteries and in those with repetitive movements, such as the knee area. This contributes to a persistence of inflammation and a change in shear stress near the stent edges. 2–5 Stent fracture has been reported in many arterial segments, including the renal, aortic, coronary, subclavian, iliac, and venous segments, but most notably in the femoropopliteal segment, appearing in up to one-third of cases with long follow-up. 6,7 Although the carotid artery is a mobile segment with characteristics similar to the femoropopliteal segment, fractures of carotid artery stents are not frequently reported in the literature.
In this article, we describe a case of carotid artery stenting that we performed and that was subsequently complicated by stent fracture, thrombus formation, and in-stent stenosis 12 days after carotid artery stenting. The obvious cause was repeated trauma and kinking at the site of the stented artery owing to the recoil of a shotgun to the patient's neck.
Case Report
A 75-year-old male patient presented with carotid artery stenosis causing transient ischemic attacks. The patient was referred to our service for further management. An angiogram revealed 79% internal carotid stenosis. The patient was managed by internal CAS using a single Acculink 7 to 10 × 40 mm stent. The stenosis was reduced to 10% (Figure 1). There were no intraoperative or postoperative complications, and the patient was discharged and put on clopidogrel 75 mg and aspirin 325 mg daily. Duplex ultrasonography done the day after the procedure revealed a peak systolic velocity of 179 cm/s and an end-diastolic velocity of 54 cm/s.
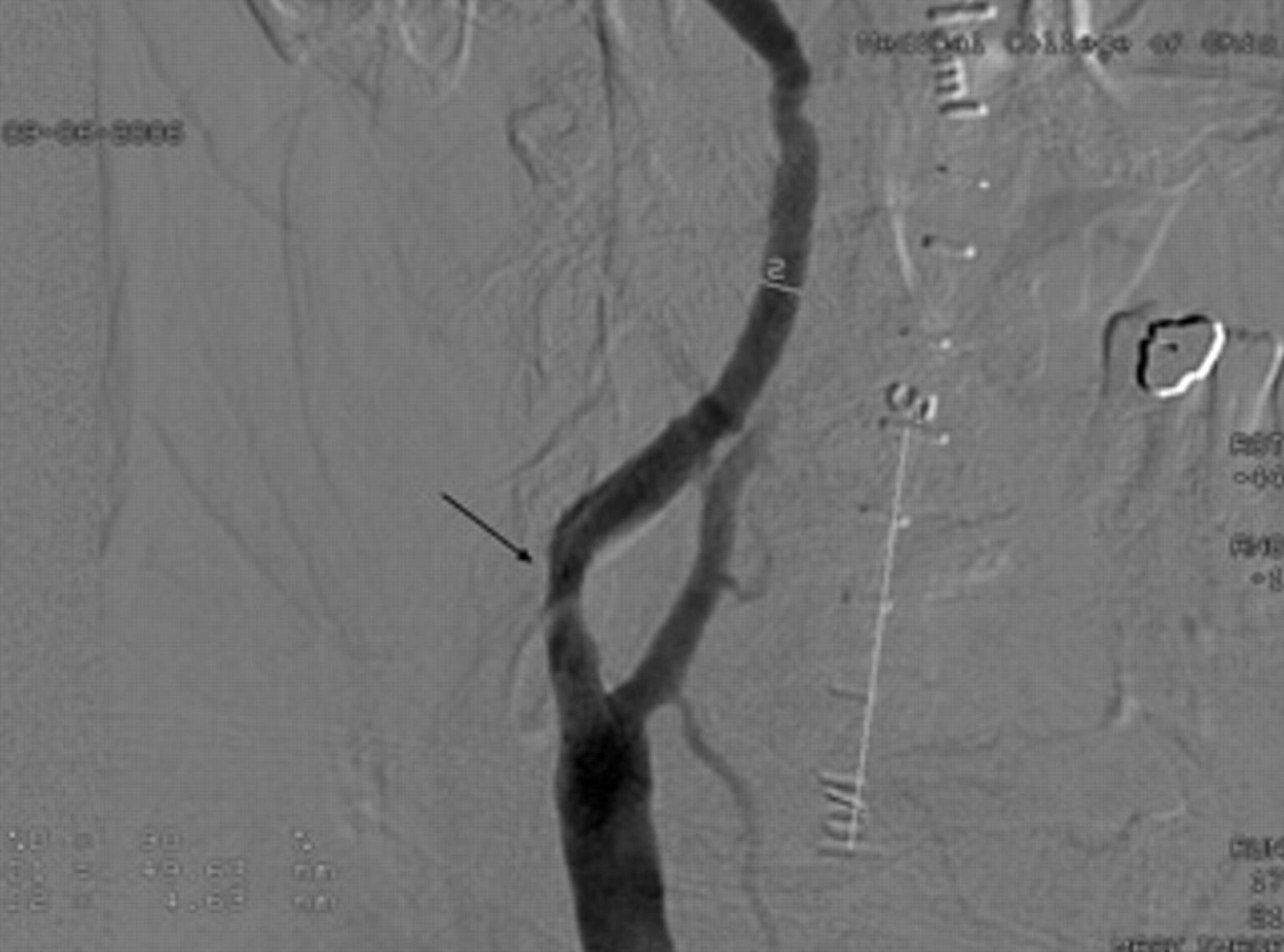
Angiogram showing the stented area; the arrow is pointing to the area of balloon angioplasty and stenting.
Twelve days later, the patient presented on the request of his spouse, who was worried about superficial bruises on his neck and chest. The day after the procedure, the patient had gone trap and skeet shooting; he shot 5,200 rounds in the week following the procedure. He complained of chest bruising and pain in the neck. He had no neurologic symptoms. He denied headache, nausea, or vomiting. Further examination showed no neurologic deficit, with normal motor power and sensory evaluation. Cranial examination was normal except for left homonymous hemianopsia, which he had had for a long time from old occipital infarcts. Cerebellar signs were negative. Mental status was normal.
A duplex sonogram was obtained and revealed increased velocities in the carotid artery with a peak systolic velocity of 435 cm/s and an end-diastolic velocity of 140 cm/s. In addition, the sonogram showed a flapping and clots within the stented segment.
The patient was admitted to the hospital and was started on full-dose heparin. A cerebral angiogram the next day showed a fractured stent with a deformity that was exaggerated by neck flexion during the angiography. In addition, he had an in-stent stenosis of 60% with a thrombus inside the stent (Figures 2 and 3).
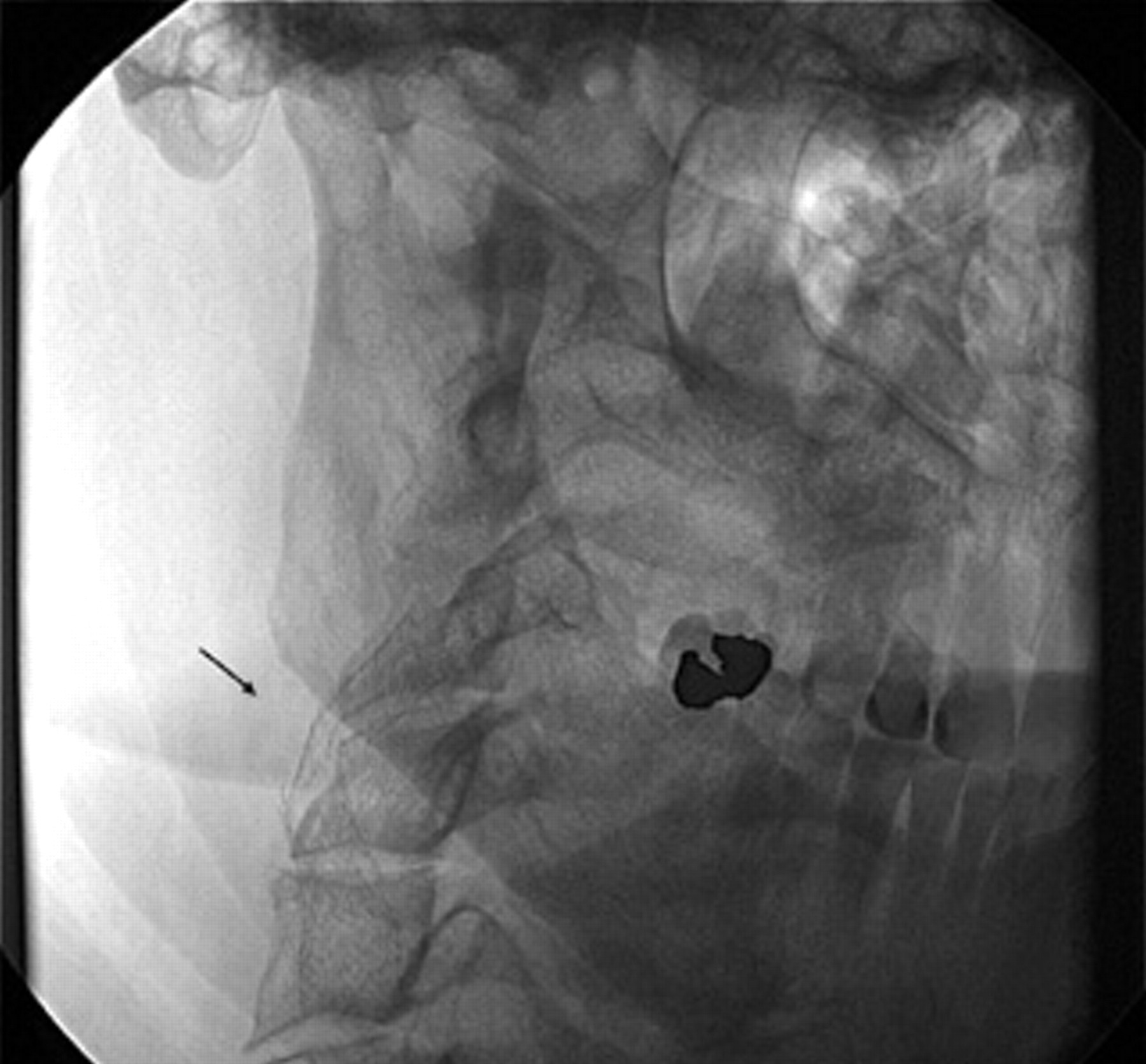
The arrow is pointing to the area of fracture in the carotid stent.
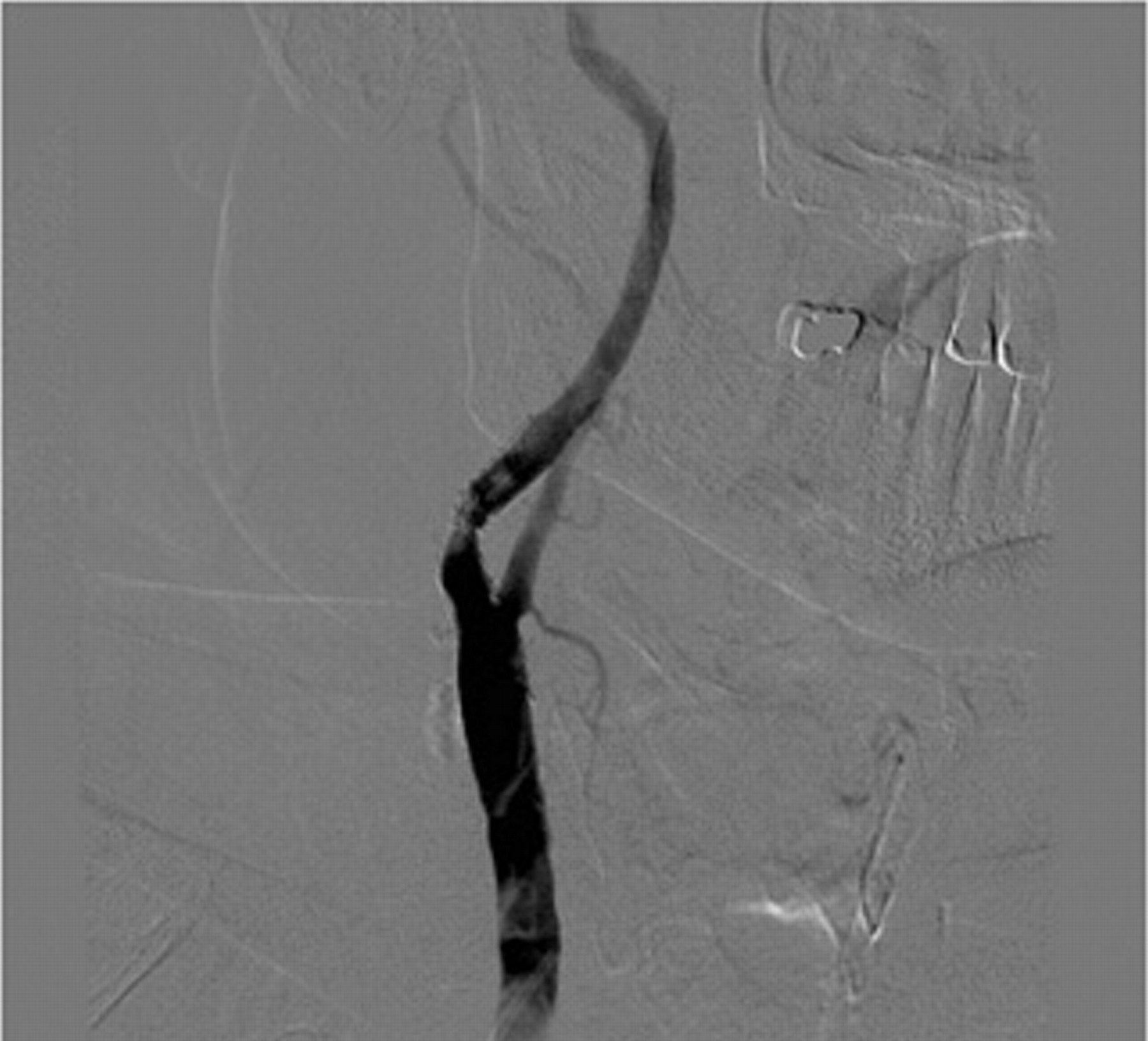
Angiogram showing thrombi and in-stent stenosis.
The patient was started on enoxaparin (Lovenox) in addition to the clopidogrel (Plavix) and aspirin and was discharged home after 1 day of observation. Follow-up studies, including a sonogram obtained 16 days after the trauma, revealed improvement in the stenosis with peak systolic velocity of 200 cm/s and an end-diastolic velocity of 50 cm/s. A repeat sonogram 23 days after the trauma showed resolution of the clot, complete adherence of the stent to the wall of the artery, and a peak systolic velocity of 165 cm/s and an end-diastolic velocity 57 cm/s. Multiple head computed tomographic scans were obtained that showed chronic changes with no evidence of acute or subacute infarction.
A repeat sonogram done at 3 months and at 9 months showed a peak systolic velocity of 140 cm/s and 148 cm/s and an end-diastolic velocity of 28 cm/s and 38 cm/s, respectively. The patient was seen 6 months after the stent fracture by a neurologist who reported no new neurologic deficits but suspected vertebrobasilar insufficiency.
Discussion
Stent fracture is one potential complication of stenting of mobile vessels. The femoropopliteal segment is peculiar for having a high incidence of stent fracture. Factors contributing to stent fracture include external mechanical forces such as arterial shortening, axial rigidity, kinking, and compression. 8 In addition, pulsatile blood flow through the stent can transmit extensive internal stress, which can contribute to stent fracture, especially near the heart or great vessels. 6,9 Moreover, the length of the stented segment has been proposed as a factor in stent fracture. The longer the stented segment and the more overlapping stents are used, the more liable the stents are to fracture. 6
Like the femoropopliteal segment, the carotid artery can be exposed to forces that might influence long-term patency and cause stent complications. In addition to the external forces mentioned above, elastic recoil owing to pharyngeal muscle contraction and external musculoskeletal compression are added forces that are expected to contribute to stent fracture in the carotid artery segment. 10 Floris and colleagues demonstrated that sharp internal carotid artery angulations were aggravated by forward bending of the head, especially at the distal stent junction. 11 Furthermore, the stented segment was found to be stiff and inflexible in all head positions in spite of the in vitro flexible nature of certain stents. The unstented segments accommodate head movements by increasing flexion and torsion, leading to friction at both ends of the stent. The authors also demonstrated considerable stent torsion shear with turning of the head to either direction. All such forces and configuration changes make the carotid artery a potential site for stent fracture. In the English literature, we found three cases of carotid stent fracture. DeVries and colleagues reported a case of carotid artery stent fracture for carotid artery pseudoaneurysm. 12 Another case of carotid stent fracture causing in-stent stenosis was described by N'Dandu and colleagues. 10 A third case was described by Valibhoy and colleagues with stent fracture 6 months after the original procedure. 13
Stent fracture could be complicated by stent migration, stent penetration, and thrombus formation with or without impedance to cerebral blood flow. All complications can be associated with distal embolization and potential neurologic deficit. Furthermore, stent fracture may contribute to myointimal hyperplasia and eventually in-stent restenosis in the long run. 10,12
The management of fractured carotid stents is controversial because of the limited number of cases reported in the literature. We successfully managed our patient with low-molecular-weight heparin and antiplatelet medications, including clopidogrel and aspirin. The low-molecular-weight heparin was continued for about 3 weeks. The patient's progress was monitored by repeated duplex sonograms. We stopped the enoxaparin once we documented resolution of the thrombi and improvement in the blood flow and when we anticipated the incorporation of the stent in the carotid artery wall. Response to our treatment was shown by the reduction in velocities by Doppler ultrasonography to those of baseline after the first procedure and the resolution of the thrombi. A more aggressive approach is in the form of restenting of the lesion by a bridging nitinol self-expanding stent in the case of the presence of neurologic symptoms or in case of severe in-stent restenosis. 10,14 This might be an acceptable approach for long-term restenosis rather than early stent fracture with thrombus formation. In patients with early stent fracture and thrombus formation, attempting restenting might be complicated by distal embolization.
In the presence of impedance to the blood flow, neurologic deficit, stent penetrating the wall of the blood vessel, or dissection of the carotid artery, open surgery with stent removal is an alternative option.
In summary, carotid stent fracture is mainly due to external forces in the form of musculoskeletal compression, stress of movements of the neck, and elastic recoil owing to pharyngeal muscle movement, or, less commonly, as in our case, owing to external trauma.
The management of such complications is dependent on the timing of stent fracture from the original procedure, the presence of stenosis, clot formation, and associated symptoms. The risk of a salvage endovascular procedure should always be weighed against the potential harm of such a procedure.