
Abstract
Jugular vein aneurysm is a rare morphologic entity. This report describes a case of an asymptomatic internal jugular vein aneurysm that presented as an enlarging mass in the neck. Diagnosis was established with duplex ultrasonography and venography. No thrombus was diagnosed in the aneurysm, but since the patient was uncomfortable with having a tumor in his neck, surgery was performed with resection of the aneurysm and lateral venorrhaphy of the jugular vein.
Keywords
Venous aneurysm is a rare morphologic entity, 1 most frequently described in children. 2,3 In adults, it is described after causing pulmonary embolism when located in the lower extremity, 4 particularly the popliteal vein. 5
In upper extremity and neck veins, aneurysm is seldom reported since it remains asymptomatic and without clinical relevance. 6 Pain and tenderness have been described as symptoms associated with jugular vein aneurysm, but no serious complications have been reported.
Duplex scanning is sufficient for reliable diagnosis, but three-dimensional ultrasonography, computed tomography (CT), magnetic resonance imaging (MRI), and venography were described as improvement for morphologic evaluation. 7,8
We present a case of an asymptomatic internal jugular vein aneurysm (IJVA) that was surgically resected after being described as disturbing for the patient. This was the one-and-only case of a venous aneurysm registered in our university high-volume vascular clinic in 14 years.
A 55-year-old man was admitted to the vascular surgery clinic for a painless mass in the base of the left side of the neck. He recognized it a year before since it enlarged gradually with straining and bending forward. Sixteen years before, he had his left thyroid lobe resected for goiter, but the postoperative course was uneventful. He denied trauma of the neck or a family history. He had no symptoms or history of heart disease.
On physical examination, a 4 × 3 cm soft, rounded, fluctuating mass was seen in the left sternoclavicular fold (Figure 1), which promptly disappeared on compression and enlarged considerably on Valsalva maneuver.
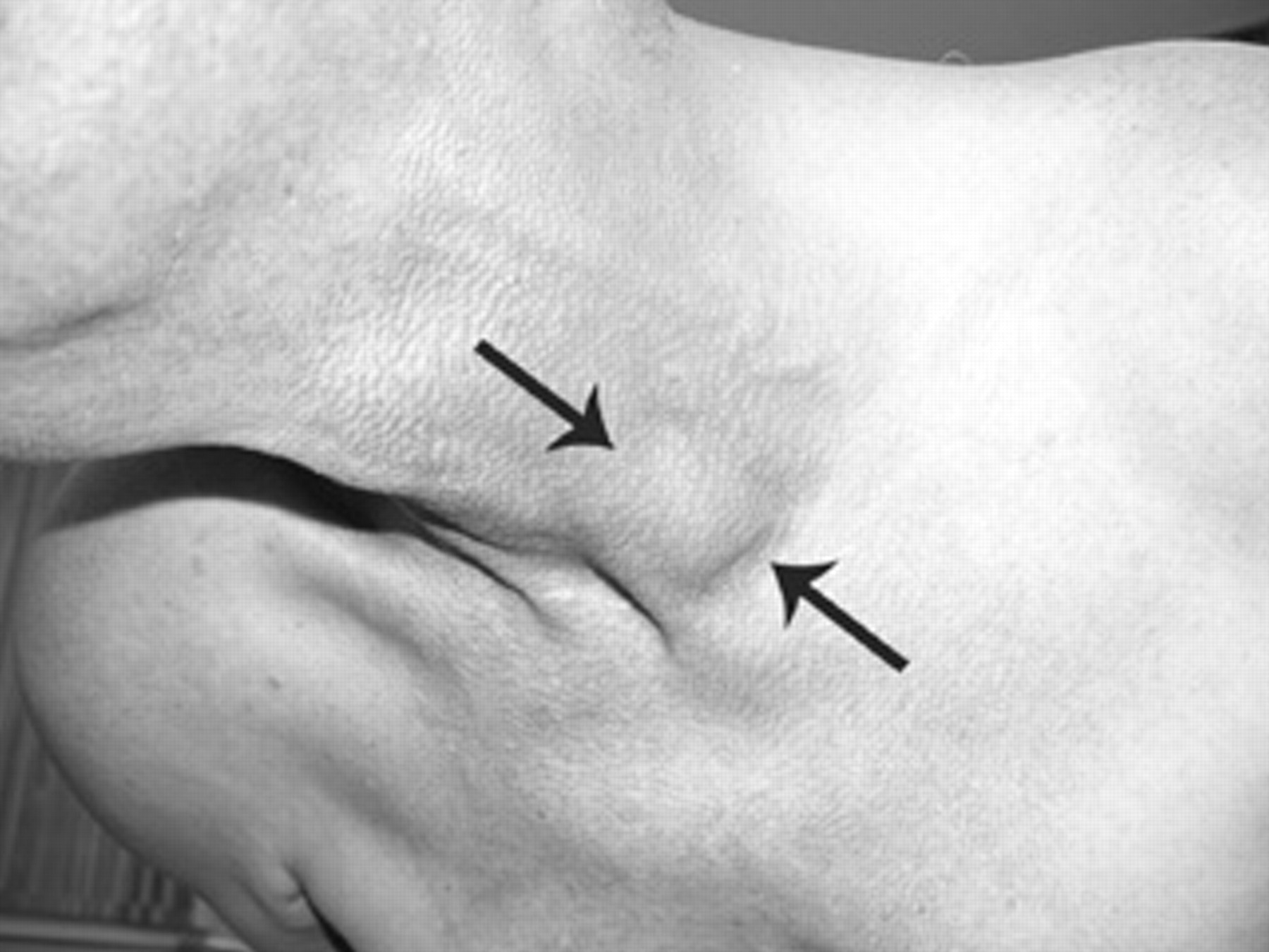
Enlargement of the aneurysm with straining and bending: arrows depict the outer limits.
Duplex ultrasonography revealed aneurysmatic formation of the internal jugular vein (Figure 2), measuring 2.82 cm by 1.14 cm in the transverse plane, with high-velocity blood flow within the central part of the aneurysm and much slower near the aneurysmal wall, with the “pseudothrombosis” effect. At venography, 6 to 7 mm communication between the aneurysm and the internal jugular vein was seen (Figure 3).

Duplex scan: Top: Size of the aneurysm and its relationship to the common carotid artery (CCA) and the internal jugular vein (IJV) in the transverse plane. Bottom: Pseudothrombosis effect (arrows) in the sagittal plane.

Venography: the aneurysmal neck is seen in the two top images.
Because the patient was very uncomfortable with having a tumor in his neck, surgery was performed through a left supraclavicular approach. After division of the clavicular head of the sternocleidomastoid and omohyoid muscles, the jugular vein and the aneurysm were dissected, and proximal and distal control was obtained (Figure 4). Reconstruction was done with resection of the aneurysm and lateral suture of the jugular vein. No thrombus was found within the aneurysm (Figure 5), and there was no reaction in the surrounding tissue to connect the previous neck surgery with the aneurysm formation. The resected aneurysmal wall was submitted for histologic examination that showed all layers of a normal vein, with fibroblastic proliferation and some mixed muscle layers, with endothelial continuity. No inflammatory infiltrate was seen.

Dissected aneurysm through the supraclavicular incision with proximal and distal control of the jugular vein.

Aneurysm opened: an opening of the aneurysmal neck is seen at the bottom of the aneurysm measuring 6 to 7 mm in diameter; no thrombus was found within the aneurysm, and the shiny inner lining of the aneurysmal wall pointed to a true aneurysm.
The operation and the postoperative course were uneventful; and the patient was discharged from the hospital on the third postoperative dayand put on aspirin 100 mg/d. Routine controls were done after 1 month, 6 months, and 1 year. Clinical and duplex scan findings during the 2-year follow-up were satisfactory.
Discussion
A venous aneurysm is a solitary area of venous dilatation that communicates with a main vein by a single channel but should not be contained within a segment of a varicose vein. 4 It should be distinguished from a pseudoaneurysm resulting from trauma 4 or infection. 9
IJVAs are rarely seen. Calligaro and colleagues found only three such aneurysms in 20 years, 1 and Gillespie and colleagues reported on five cases in 22 years. 4 The majority of papers published to date are single case reports. Our case was a single one with IJVA from 1994 to the present, registered in a high-volume university hospital that performs over 1,500 surgical procedures per year.
The etiology of IJVA was described as degeneration process, resulting in thinning of the elastic and muscular layers in the otherwise normal vein wall after prolonged mechanical stress. 1,2,5 Mechanical venous obstruction and congenital defects have been described in children 2,3,8 and neurofibromatous venous invasion in adults. 10 In our patient, there was no reaction in the surrounding tissue to connect the previous neck surgery with the aneurysm formation, and histologic examination showed all layers of a normal vein.
As in our patient, venous aneurysms in the neck are generally asymptomatic. 1,4,6 Among all, differential diagnosis of lateral cervical masses includes arteriovenous malformation, thyroglossal cysts, retention cysts, cystic hygroma, pharyngocele, laryngocele, different tumors, and cupula inflation. 1,8,11 Soft swelling in the neck that occurs during cough, straining, bending over, and with Valsalva maneuver should imply jugular vein enlargement, ecstasy, or aneurysm. However, this finding might be seen with mediastinal tumors, laryngeal malformations, and simple cupula inflation. 8 This dilemma is easily solved using duplex ultrasonography demonstrating typical venous flow patterns. 7,8 In our case, a pseudothrombosis effect of different blood flow near the aneurysm wall and in the central parts was registered. This phenomenon, seen in larger aneurysms, is important because it might prompt a surgical team to perform an urgent procedure, fearing embolic complications, without a thorough workup on the patient, thus increasing the potential for postoperative morbidity. However, duplex scanning was described as a reliable technique in the majority of reports and sufficient for surgical treatment. 1–3,9,10,12
In the vast majority of situations, there are multiple diagnostic modalities, such as venography, three- and four-dimensional ultrasonography, CT, and MRI. Using this, redundant information is gathered, particularly for delineation of venous anatomy. Potential drawbacks are the invasiveness of venography, costs, equipment unavailability, and need for highly trained personnel.
Because of the low incidence of IJVA, common treatment guidelines are not clearly established. 12 Given that IJVA remains asymptomatic in the majority of cases and mural thrombosis is infrequently encountered, conservative treatment was recommended. 1,2,4,6
None of the patients treated in such a manner developed complications during follow-up. 1 Symptomatic IJVA, enlarging masses, and cosmetic reasons were the reasons for surgical treatment in the majority of reports. No complications were encountered with patients treated surgicaly, 1,3,6,12 except for the case presented by Nopajaroonsri and Lurie of a patient with IJVA with neurofibromatosis. 10 After excision and reconstruction, repeated procedures were necessary to obtain hemostasis, but this complication was well recognized for neurofibromatosis and not for the IJVA itself. In the case of our patient, he was very uncomfortable with having a tumor in his neck, so surgical treatment was proposed. Another important indication for surgical treatment should be considered, as proposed by Sakalioĝlu and colleagues. 2 Given that civilian trauma has become very frequent nowdays, major hemorrhage might occur from IJVA if someone is incidentally injured.
Resection of the aneurysm with lateral venorrhaphy was the technique that we used. Similar experience was reported and suggested by the majority of authors. 1–4,6