
Abstract

SESSION I: Bioengineering: The Latest Innovation in Vascular Disease
Moderators: Dusan Pavcnik, MD, David L. Gillespie, MD
Nicholas J. Cheshire
Alan Dardik, MD, PhD
Yale University School of Medicine, New Haven, CT, USA
John P. Fletcher, A.K. Guiffre, M.W.Y. Williams, M. Vicaretti, H. Medbury
Vascular Biology Research Centre, University of Sydney and Westmead Hospital, Sydney, New South Wales, Australia
The stability of an atherosclerotic plaque is a key determining factor in the clinical outcome in cardiovascular disease. Alpha smooth muscle cell (SMC) actin-positive cells play an important role in maintaining plaque stability through the formation of a fibrous cap. Evidence suggests that circulating progenitors may be a source of these cells, and our aim was to determine whether these cells may be fibrocytes, which are bone marrow-derived cells that acquire SMC characteristics. Carotid endarterectomy specimens were examined for the presence of fibrocytes by double immunohistochemistry staining for vimentin and CD34. Fibrocytes were found in the cap, predominantly in regions of healing of recent plaque rupture. They possessed the typical SMC spindle shape, and their contribution to the alpha SMC actin population was confirmed by co-staining of CD34 with alpha SMC actin. Consistent with being fibrocytes, they colocalized with transforming growth factor β, a factor known to promote fibrocyte formation that is also associated with stable plaque. By double-staining with Ham56, evidence was provided for the monocyte origin of these cells. In addition, we showed in vitro that platelets can induce monocyte transformation into fibrocytes. Monocytes may play a more crucial role in the clinical outcome of atherosclerotic plaque than previously realized as they contribute directly, not only to foam cell formation and therefore plaque instability but also to fibrocyte formation promoting plaque stability.
Dusan Pavcnik, MD
Dotter Interventional Institute, Oregon Health & Science University, Portland, Oregon, USA
Michel Perrin, MD Lyon, France
Options for tissue engineering of venous valves fall into two categories: scaffolds seeking incorporation as self and scaffolds identified as self
In the first category, valve cusp nonautogenous off-the-shelf valve substitutes have either failed initial clinical evaluation or remain under development.1–3
In the second group, the results provided by valves created in animal and experimental studies by intussuscepting an autogenous vein into itself have been more successful.
Several clinical studies have also evaluated the use of autogenous venous tissue to create venous valves.
Raju and Hardy reported good results in a small series 4 ; Plagnol and colleagues, by invaginating a stump of the great saphenous vein, published a good outcome in a 20-patient series but with a short follow-up (mean 10 months). 5
Maleti described the most promising technique; he created a bicuspid or monocusp valve by dissecting the intimal/medial wall of the thickened postthrombotic vein to form cusps. 6 Neovalve construction was performed in 18 limbs, and ulcer healed in 89%. In 17 limbs (95%), the treated segments remained patent (95%) at a median follow-up of 22 months with no ulcer recurrence. 7
Currently, he has a larger series (39 limbs) with a longer follow-up (median 33 months) with the same good outcome (personal communication).
Marto Hoary, Sherif Sultan Embricon, Galway, Ireland
Varicose vein surgery is currently one of the most frequently performed procedures in many countries. There has been relatively little innovation in this field over the past 50 years. The ball and chain method has been the gold standard for about the past 100 years. In 2000, two new ablation technologies were introduced. None of these procedures provide optimum results. They are associated with postprocedural pain, paresthesia, induration, and recanalization.
There is a lack of robust evidence, longer operating times, and greater expense associated with the management of varicose veins recently. Publications have generated considerable interest in new techniques for treating varicose veins, claiming major advantages over conventional surgery. The main objective of these new techniques is to reduce postoperative trauma and bruising, leading to faster postoperative recovery. All of these methods are dependent on the use of duplex ultrasound. Evidence of the success of the new techniques is limited to serious cases and registry data largely in private practice. However, vascular surgeons have some skepticism especially when conventional surgery is portrayed in a falsely unfavorable light.
Radiofrequency, laser, and foam therapy are used in the management of varicose veins. However, the 5-year outcome of laser and radiofrequency therapies is not yet available. Their recurrence rate following foam sclerotherapy is 80% after 5 years, with a high incidence of TIAs and stroke. Complete upward stripping has an incidence of pretibial and infrapatellar saphenous nerve branch injury of 70%. Complete downward stripping has an incidence of 40% of saphenous nerve injury. Inverted stripping can reduce preoperative blood loss, postoperative bruising, pain, and saphenous nerve injury compared with conventional telescopic stripping with the aid of an acorn-shaped tip stripper. Perforate-invaginate stripping (PIN stripping) employed the same concept as inverted stripping. However, the PIN stripper is too rigid to pass from the groin to below the knee; thus, a two-step maneuver is required. Inverted downward stripping has good cosmetic results and avoids postoperative morbidity.
We offer a unique process and device for this procedure that we believe can become the gold standard because it meets all of the criteria of best medical practice. Surgeons can be trained in this new and simplified endovenous upward PIN stripping process, which offers reduced incidence of nerve damage, bruising, ecchymosis, and faster recovery time.
Caitríona Lally, Vittoria Flamini, Christian Kerskens, Arthur Creane, Daniel Kelly, Niamh Hynes, Sherif Sultan, School of Mechanical and Manufacturing Engineering, Dublin City University, Glasnevin, Dublin, Ireland; Western Vascular Institute, Department of Vascular and Endovascular Surgery, University College Hospital, Galway; The Galway Clinic, Doughiska, Galway, Ireland; Department of Bioengeering, Trinity College, Dublin, Ireland
The objective of this study is to noninvasively determine the mechanical properties of arterial tissue using suitable imaging techniques.
Arterial tissue has been found to be a fiber-reinforced material; therefore, two approaches have been taken: (i) fiber orientations have been characterized within aortic tissue using magnetic resonance imaging (MRI) and in particular diffusion tensor imaging (DTI), and (ii) carotid plaque properties have been determined using duplex ultrasound (US) scans.
Porcine aortas were harvested and housed in a custom-designed chamber, which was inserted into a phased array coil inside a 7 T magnet (BrUnited Kingdomer Biospin). DTI was performed, and the images were postprocessed using the DTI track module from MedINRIA (INRIA, Sophia Antipolis). The aortic boundaries were tracked manually and the fiber patterns were exported to MatLAB, where a custom routine was developed to analyze the fiber angles.
Duplex images were obtained of atherosclerotic carotid vessels prior to endarterectomy procedures being carried out. The images were analyzed to determine grayscale median (GSM) values for the plaques in the vessel. These plaques were harvested from the vessel, and postendarterectomy mechanical tests were conducted to determine the uniaxial properties of these tissues and their relationship to the duplex GSM values.
DTI MRI proved successful as a technique to non-invasively determine the fiber pattern in an aorta. Fiber angles were found to align longitudinally in the vessel intima and to range between 65þ and 70þ, relative to the longitudinal axis of the vessel, within the vessel media.
Carotid plaques are currently being mechanically characterized based on the duplex GSM values, and the values of stress/strain obtained at plaque rupture will be used to assess the probability of plaque rupture in finite element models of realistic carotid arteries.
The determination of in vivo fiber orientations and mechanical properties of arterial tissue using noninvasive imaging can enable earlier diagnosis of degenerative tissue diseases such as abdominal aortic aneurysms or potentially vulnerable plaques. In addition, numerical models using realistic patient-specific mechanical properties can be used to improve intravascular device designs and preclinically test new innovative patient-specific devices.
Eamon Brady
R&D New Ventures, Abbott Vascular, Galway, Ireland
Endovascular technology has advanced at a tremendous pace over the last 20 years, and the momentum of innovation in the field looks set to continue for many years to come. Over this same period, the regulatory barriers to device approval have grown progressively higher. Similarly, the complexity of the patent landscape has increased, so that although innovation may be the key to developing new lifesaving therapies, the path to realizing the fruits of this innovation can be lengthy and expensive.
Although the rewards for both patient and innovator can be huge, the probability of failure is extremely high, and mistakes in the management of new innovations can be very costly. In fact, over 90% of patent filings fail to generate enough revenue to cover their costs. If investment made at the start of such projects is not focused appropriately, the value of the innovators holding becomes quickly diluted or disappears entirely.
Capturing the value of new innovations is therefore not a simple challenge, but the likelihood of success of this endeavor can be greatly influenced by the approaches taken at the earliest stages of development. This presentation will focus on steps to maximize value and minimize risk in the early phase of the development of new medical innovations.
Rodney A. White
Michael Drues, PhD
Grafton, Massachusetts, USA
The focus of this session will be on one of the most commonly used and controversial products in medicine today: the drug-eluting stent. This session will provide a critical look at the drug-eluting stent as it exists today. What are they supposed to do? What do they really do? Does what we do today make sense? Are problems like chronic in-stent thrombosis “unexpected”? The better we understand the advantages and limitations of current technologies, the better poised we will be to move intelligently into the future.
This session will provide a view into the future of the drug-eluting stent. What we have today is child's play by comparison! Why do we think of a drug-eluting stent as a stent? By incorporating multiple drugs, biologics, and a wide range of biotherapeutics into a single device, a.k.a. a multiple biotherapeutic carrying vehicle, we can use a drug-eluting stent as a syringe to treat far more than simple arthrosclerosis. Potential applications include diabetes, cancer, Alzheimer disease, gene therapy, and angiogenesis, just to name a few!
SESSION II: Carotid Disease I: Endovascular Management: Lessons from the Past We Can Bring to the Future
Moderators: Piergiorgio Cao, MD, FRCS, Rodney A. White, MD
Piergiorgio Cao, MD, FRCS
Division of Vascular and Endovascular Surgery, University of Perugia, Ospedale S. Maria della Misericordia, Perugia, Italy
Max Amor, MD, G. Ethevenot, C. Breton, J.P.S. Simon, Z. Chati
Cardiovascular Department, Clinic Louis Pasteur, Essey les Nancy, France
At the present time, guidelines for adequate treatment of both symptomatic and asymptomatic carotid artery stenoses are vague for patients with symptomatic CAD: ignoring carotid or coronary lesions, performing staged operations with delay of one of the procedures (or reverse staged: CABG ▸ CEA), combining coronary grafting and CEA during the same anesthesia, performing only carotid stenting and coronary angioplasty.
Prospective studies have shown that 8 to 14% of CABG patients have significant carotid stenosis, whereas it has been estimated that up to 28% of patients undergoing exploration for CEA have severe correctable CAD. Furthermore, CAD is the leading cause of both early and late mortality after CEA. Although the overall incidence of complications after CABG has decreased, the incidence of neurologic complications (neuropsychological, stroke) remains unchanged, being reported from 0.8 to 3.2% in retrospective studies and from 1.5 to 6% in prospective studies.
A recent systematic review of outcomes following staged (CEA then CABG), reverse staged (CABG then CEA), and synchronous CEA and CABG (Naylor AR. Eur J Vasc Endovasc Surg 2003;25:380–9) has shown that mortality was highest with synchronous (4.6%), whereas reverse staged has the highest risk of ipsilateral stroke (5.8%). Perioperative MI was lowest following the reverse staged procedure (0.9%) and highest in the staged procedure (3.2%). The risk of death/stroke/MI was 11.5% after synchronous and 10.2% after staged CEA-CABG (not significant).
The recent US randomized trial comparing CEA to carotid artery stenting in high-risk patients for surgery (Sapphire Trial) have shown the superiority of CAS over CEA in reducing ischemic myocardial complications. These data have been confirmed by other trials or registries (SPACE, ARCHER, BEACH…) and are considered nowadays as favorable factors for CAS in severe insufficient coronary patients. These results indicate that CAS in patients with concomitant severe coronary artery disease is feasible and safe and may be an alternative to combined carotid and coronary surgery.
Several modalities have been explored: CAS following or preceding PTCA (coronary angioplasty), CAS and PTCA in the same session, CAS followed by CABG and/or valvular aortic replacement.
The proposed indications for CAS in the presence of symptomatic coronary artery disease are patients with carotid lesions not recommended for CEA (neck radiation, hostile neck, recurrent stenosis, contralateral occlusion), patients accessible to PTCA (PTCA and CAS could be performed during the same hospitalization), patients with bilateral carotid artery lesions (both carotid lesions are treated; we know from surgical series that stroke occurs more frequently in the neglected side), patients with tandem lesions, patients with comorbidity, old patients, respiratory disease, patients with a past thoracic or cardiac surgery, redo cardiac surgery.
The patients with carotid artery lesions not accessible to CAS or not treatable with antiplatelet therapy are candidates for CEA.
Our experience indicates that high-risk patients with severe coronary artery disease, three-vessel disease, and poor ventricular function can be successfully treated for carotid artery stenosis. Nevertheless, the complexity of these patients requires excellent multi-disciplinary teams with good understanding of these intricate diseases and excellent experience of carotid stenting and carotid protection. A cooperative study is indispensable to help us most clinically and increase our patchy knowledge.
Carlos H. Timaran, Eric B. Rosero, MD, J. Gregory Modrall, MD, James Valentine, MD, Patrick Clagett, MD
University of Texas Southwestern Medical Center, Plano, Texas, USA
Nicholas J. Cheshire
Anthony J. Comerota, MD, FACS, FACC Jobst Vascular Center, Toledo, Ohio, USA
Octogenarians are an increasing percentage of patients being treated for carotid artery disease. Enthusiasts of carotid angioplasty and stenting (CAS) frequently refer to patients 80 years of age as being “high risk” because they were excluded from the North American Symptomatic Carotid Endarterectomy Trial (NASCET) and the Asymptomatic Carotid Endarterectomy Study (ACAS). However, octogenarians were excluded because they were less likely to survive the 5-year minimum projected study period independent of their treatment for carotid disease, not because investigators feared higher procedure-related events.
Interestingly, a paradox has occurred with CAS in octogenarians. CAS has resulted in procedure-related stroke and death rates of 13 to 25%.1–3 Although carotid endarterectomy (CEA) is associated with slightly higher procedure-related risk in octogenarians, the reported procedure-related stroke/death rate is well within outcome recommendations of large multi-disciplinary consensus committees (3.2–3.5%). 4 Until data are available indicating otherwise, it is clear that octogenarians should not be offered CAS for any indication unless they are part of a randomized trial.
Mark K. Eskandari, MD, Division of Vascular Surgery
Northwestern University, Feinberg School of Medicine, Chicago, Illinois, USA
Niamh Hynes, Sherif Sultan
Western Vascular Institute, Department of Vascular and Endovascular Surgery, University College Hospital, Galway, Ireland; The Galway Clinic, Doughiska, Galway, Ireland
CEA is the gold standard in stroke preclusion. Although CAS showed initial promise in high-risk patients, recent trials have cast doubt on safety and efficacy. Our aim is to conciliate CAS with CEA and BMT in high-risk patients regarding clinical success, efficacy in plummeting morbidity and mortality, and recuperating cost-effectiveness. Primary end points were stroke, myocardial infarction, or death. Secondary end points were patency rate, cost-effectiveness, length of hospital stay, and reintervention rate. From 2002 to 2007, 612 patients with carotid artery disease were managed; 198 had intervention. Ninety-eight were high risk and symptomatic with low GSM on preoperative duplex ultrasound. Patients were assigned to CEA (n = 31), CAS (n = 29), or BMT (n = 38). Ten had bilateral interventions. Follow-up data at 6 weeks and at 3, 6, and 12 months and yearly thereafter were scrutinized.
Mean age was similar between groups (CEA, 73 years; CAS, 71 years; BMT, 74 years; p = .373). Male to female ratios were 2:1 for CEA and CAS and 1:1 for BMT. Comorbidity severity scores were similar between groups (p > .05). Lengths of HDU/hospital stay were lower in CAS, p = .0001 and p = .025, respectively. Mean cost per patient was reduced with CAS at €3,500 versus €4,650 for CEA with p < .05. Thirty-day stroke and death rates were 3% for CEA and zero for CAST.
Overall 2-year survival for BMT was 70.7% (± SE 10%). Two-year stroke-free survival for BMT (62% ± SE 11%) was significantly reduced when compared to CAS (92% ± SE 6.3%, p = .01, hazard ratio = 0.17, 95% CI 0.06–0.48) and CEA (96.7% ± SE 3.38%, p = .0021, hazard ratio = 0.08, 95% CI 0.03–4.11). Four patients in the CAS group required on-table tPA. Three of these recovered fully by the end of the procedure, and the fourth, an 84-year-old lady, had a postoperative hyperperfusion reaction and required overnight care in the HDU. There was no significant difference in 2-year stroke-free survival between CAS and CEA (p = .493, hazards ratio = 2.26, 95% CI 0.045–4.26).
CEA is still the gold standard in management of carotid artery disease with superior stroke-free survival rates at 2 years when compared to CAS or BMT. CAS significantly improves stroke-free survival compared to BMT. However, strict selection criteria apply and outcome is adversely affected by serpentine internal carotid arteries, echolucent materials, and age greater than 80 years.
DEBATE
14.44 Carotid Artery Stenting Has Been Firmly Established as a Treatment for All Forms of Carotid Artery Disease
Piergiorgio Cao, MD, FRCS
14.51 Contemporary Trends in Carotid Intervention: the 21st Century Approach to Carotid Endarterectomy, Carotid Artery Stenting under Neuro Protection and Optimal Medical Treatment
Sherif Sultan
Advances in Carotid Artery Stenting, although initially promising, have so far failed to live up to expectations. The randomized trials have been far from flawless and as such have been unconvincing in their conclusions on either superiority or even non-inferiority of Carotid stenting over Carotid Endarterectomy. However there are now new contestants in the game and the goal posts have shifted. While Carotid Endarterectomy was once shown to be superior to optimal medical therapy alone, advances in both pharmacotherapy and nanotechnology mean that the focus is now on plaque vulnerability and patient specific therapy rather than just mode of intervention.
14.58–15.08 Voting and Panel Discussion
SESSION III: Peripheral Vascular Disease I: The Current Status of Endovascular Management: Is It Now the Gold Standard?
Moderators: Peter R.F. Bell, MD, FRCS, DSC KBE, Anil P. Hingorani, MD
15.08 Subintimal Angioplasty (SIA) versus Bypass Surgery (BS) in TASC C and D Lesions in the Femoropopliteal Segment: Randomization of CLI Patients according to Plaque Echolucency: A 5-Year Prospective Study
Sherif Sultan, Niamh Hynes
Western Vascular Institute, Department of Vascular and Endovascular Surgery, University College Hospital, Galway, Ireland; The Galway Clinic, Doughiska, Galway, Ireland
Our primary aim is to equate the effectiveness of SIA with BS in sustaining amputation-free survival (AFS). Secondary end points are risk of major adverse events (MAE), quality time without symptoms of disease or toxicity of treatment (Q-TWiST), and cost-effectiveness.
From 2002 to 2007, 1,076 patients were referred with PVD. We prospectively compared 334 primary procedures (SIA = 206, BS = 128) in 309 patients (NSIA = 190, NBS = 119) with TASC C and D lesions. Mean age (SIA 73 ± 13 years versus BS 70 ±14 years, p = .127) and comorbidity severity scores (p > .05) were similar between groups. Fifty-five percent were females in the SIA group versus 35% in BS, p = .0005.
Five-year primary patency for SIA was improved (SIA 72.8% vs BS65.3%, p = .7001). Five-year assisted-primary patency and secondary patency rates were enhanced with SIA (82.8% vs 68.2%, p = .1061) and (85.9% vs 72.1%, p = .2624), respectively.
Patency was not influenced by homocysteine (pSIA = 0.841, pBS = 0.198), CRP (pSIA = 0.629, pBS = 0.408), fibrinogen (pSIA = 0.594, pBS = 0.101), or HbA1C (pSIA = 0.446, pBS = 0.208). Results were not impinged on by stent use (35%, p = .780) or mean number of stents used (1.3, p = .330).
Hyperfibrinogenemia had a significant adverse effect on 5-year AFS for SIA (p = .009, RR 2.4, 95% CI = 1.2–4.6) with baseline survivor functions of 0.929 if above 4 μmol/L. Elevated CRP had an adverse effect (p = .019, RR 1.02, 95% CI = 1.01–1.04), with a baseline survivor function of 0.833 if above 12 mg/L.
Five-year all-cause survival was similar for SIA (78.6%) and BS (80.1%), p = .7343. Five-year AFS was comparable (SIA 72.9% vs BS 71.2%, p = .9765).
Risk of MAE (p < .002) and length of hospital stay (LOSSIA. 14 ± 16 days vs LOSBS 24 ± 23 days, p < .0001) were significantly reduced with SIA. Q-TWiST significantly improved (p < .001), and cost per QALY (SIA: €5,663 vs BS: €9,172, p < .05) was reduced with SIA. Five-year risk of reintervention (p > .05) and mean number of procedures (SIA 1.19 vs BS 1.10, p = .078) were similar.
SIA enhances patient-specific Q-TWiST with substantial cost reduction. SIA augments symptom-free survival, is minimally invasive, and allows for a high patient turnover without compromising limb salvage.
Anil P. Hingorani, MD
College of Medicine, SUNY Brooklyn and Maimonides Medical Center, Brooklyn, New York
This study assessed whether the duplex ultrasound (DUS)-derived grayscale median (GSM) of the most six distal portion of the occluded femoropopliteal arterial segment can predict success of lumen reentry for subintimal angioplasty. In addition, we will review the clinical utility and application of reentry devices in our experience.
Ali Amin, MD, RVT, FACS, FACC
There is little controversy regarding the potential benefit of endovascular intervention in a hemodynamically significant symptomatic arterial stenosis. However, the definition of a hemodynamically significant stenosis based on an angiogram is difficult to establish. This is especially true in the management of renal artery stenosis. Renal artery stenosis is often an incidental finding in patients with arterial hypertension and atherosclerosis. Therefore, the finding of a renal artery stenosis in patients with hypertension is frequent but often leaves the physician with the question of whether the renal artery stenosis is the main cause of arterial hypertension or renal insufficiency. Also, the definition of a hemodynamically severe stenosis is lacking. Catheter angiography remains the “gold standard” for the evaluation of renal artery stenosis. Interventionalists generally define the minimal threshold for an angiographically significant stenosis to be a > 50% luminal diameter reduction, translating to a > 75% cross-sectional narrowing. To cause hypertension, a renal artery stenosis should produce a significant pressure gradient between the aorta and glomerular afferent arterioles. Although a pressure wire can be used to measure gradient, it is expensive. Another novel approach involves measuring the gradient using a 4F catheter over a 0.014 wire and a Y connector. A peak systolic pressure gradient larger than 20 mm or 10% of aortic pressure may represent a hemodynamically significant lesion. This measurement can be used for other arterial beds, including femoral, iliac arteries. In the lower extremity, NTG bolus can be used to vasodilate the arterial bed distal to the lesion.
Anil P. Hingorani, MD
College of Medicine, SUNY Brooklyn and Maimonides Medical Center, Brooklyn, New York
Helen M. Heneghan, Sherif Sultan
Western Vascular Institute, Department of Vascular and Endovascular Surgery, University College Hospital, Galway, Ireland; The Galway Clinic, Doughiska, Galway, Ireland
Wael Tawfick, H. Nashat, Helen Heneghan, Sherif Sultan
Western Vascular Institute, Department of Vascular and Endovascular Surgery, University College Hospital, Galway, Ireland; The Galway Clinic, Doughiska, Galway, Ireland
Endovascular revascularization (EvR) for critical limb ischemia (CLI) is increasingly becoming an alternative to distal bypass arterial reconstructive surgery. Despite the advent of EvR in tibial vessels, there is still concern about some complex lesions, as fibrocalcific disease, small vessel disease, and no target vessel runoff.
The aim of this study is to compare the outcome of TBA with that of CELA in tibial vessel occlusion. The composite primary end point is primary and secondary continued anatomic success, limb salvage, and amputation-free survival. The secondary end point is survival free from major adverse events.
Between June 2004 and June 2007, 35 EvRs were performed on tibial vessels for CLI. All patients were Rutherford category 5. All patients were commenced on clopidogrel postoperatively.
The mean age was 69 years (48–96 years). Twenty-one angioplasties were performed using TBA; 14 were performed using CELA. The two groups were comparable regarding demographics, vascular-related risk factors, and runoff grading. Twelve angioplasties of the posterior tibial vessels were performed, 15 of the anterior tibial vessels, and 8 of the peroneal vessels.

Survival free of major adverse events was comparable in both groups.
Tibial EvR provides an outstanding outcome in CLI. Cool eximer laser-assisted angioplasty softens calcific plaque, providing improved anatomical success rates and clinical outcome over TBA in complex calcific tibial vessel occlusions.
DEBATE
15.46 Endovascular Treatment Is Now the Gold Standard for Lower Limb Revascularization
Peter R.F. Bell, MD, FRCS, DSC, KBE
15.53 Bypass Surgery Will Always Have a Secure Place in the Management of Lower Limb Occlusive Disease
Martin Feeley
Department of Vascular Surgery, The Adelaide and Meath Hospital incorporating the National Children's Hospital, Tallaght, Dublin, Ireland
The evolution of vascular surgery is well recognized in the treatment of AAA and carotid disease. However, the endovascular treatment of lower limb occlusive arterial disease precedes these exciting developments by a number of years and has continued to evolve/develop/improve steadily.
There have been many exciting technological innovations that failed to deliver, for example, the Smart Laser and the Kensey atherectomy device. Nevertheless, endovascular treatment of lower limb occlusive disease continues to increase to the point where endovascular is first-option treatment for critical ischemia in many centers, with acceptable results.
The results of infrainguinal balloon angioplasty for complex disease have been disappointing. A host of newer technologies, including cryoplasty, rotational atherectomy, drug-eluting stents, and ongoing improvement in guidewire and catheter technology, will lead to better results.
The bailout mechanism available to endovascular therapies is most frequently a bypass procedure. The first-line therapy is still, in many situations, a bypass procedure.
The best results will be obtained if you have both tools in the toolbox.
16.00–16.10: Voting and Discussion Panel
16.10–16.30 COFFEE BREAK
SESSION IV: Vascular Training: How to Train the Endovascular Specialist of the Future: International Perspectives
Moderators: K. Craig Kent, MD, John P. Fletcher, MD, MS, FRACS, FRCS, DDU
Sherif Sultan, Niamh Hynes Western Vascular Institute, University College Hospital, Galway, Ireland; Department of Vascular and Endovascular Surgery, Galway Clinic, Doughiska, Galway, Ireland
Higher DPV of select procedures augments surgical proficiency. Systemic review shows that high surgeon volume and specialization are independently associated with improved patient outcome.
The primary aim is to gauge whether high DPV during the endovascular revolution has influenced surgical training. The secondary aim is to estimate impact on patient outcome.
We assessed a prospectively maintained Vascubase for influence of endovascular specialization, treatment modality, and surgical volume on clinical and technical outcome, long-term survival, and vascular training.
From 1990 to 2000, all AAA were done by open repair. Since 2001, the total number of AAA repairs increased by 65%, but the absolute number of open repairs has not dropped (mean 20th 17 vs mean 21st 28, p = .140). Perioperative mortality for open repair dropped to 1.8% from 15% (p < .0001, HR = 0.12, 95% CI 0.05–0.30) for elective and from 64.3% to 34.4% (p = .0172, HR = 0.45, 95% CI 0.26–0.79) for emergency.
From 1990 to 2000, 98% of revascularizations for CLI were surgical and 2% were endovascular. Since 2001, 52% were performed endovascularly and 48% by surgery (p < .00001, z = 17.15, Pbypass20th-Pbypass21st = 0.49, 95% CI = 0.45–0.54). The number of endovascular revascularizations increased, but surgery numbers have not dropped (mean 20th 46 vs mean 21st 35, p = .124). Overall perioperative mortality fell from 16 to 2.3%. The primary amputation rate decreased from 33 to 21% (p < .00001, z = 5.041, P20th-P21st = 0.12, 95% CI = 0.073–0.168). One-year amputation-free survival is 87.4%.
Since 2001, annual mean number of carotid procedures increased 28-fold, from 2.3 to 64.3 (p < .001), with 15% now done by endovascular intervention. This led to significant gains in perioperative stroke rates (< 0.4%, 95% CI 0–3.8%), 5-year stroke-free survival (75.9%, 95% CI 69.7–81.2%), 5-year primary patency (94.6%, 95% CI 90.5–97.0).
High DPVs in specialized centers enhance aneurysm-related, stroke-free, and amputation-free survival, with a significant decrease in major adverse events (p < .001), length of hospital stay (p <.0001), and cost per procedure (p <.05).
The endovascular revolution has not instigated any fall in the number of open procedures. In specialized vascular units, trainees’ open, endovascular, and hybrid exposure is significant, with increased quality and quantity and no requirement for time wasting in general surgery training.
Anil P. Hingorani, MD
College of Medicine, SUNY Brooklyn and Maimonides Medical Center, Brooklyn, New York
Cliff P. Shearman
Department of Vascular Surgery, Southampton General Hospital, Southampton, United Kingdom
In the last decade, there have been vast changes in the delivery of vascular services. Patients’ expectations have increased, many vascular patients present acutely and need immediate treatment, and, finally, advances in endovascular and medical treatment have changed practice. At present in the United Kingdom, surgeons wishing to undertake vascular surgical training have to complete a general surgical training program and sub-specialize in vascular surgery for 2 years.
This system is no longer tenable. To acquire the open and endovascular skills required of a future vascular specialist is not possible in 2 years. Also, as the final exit examination includes general surgery, candidates do not wish to jeopardize their chances of passing by dropping general surgery too early in training and so cannot gain the vascular skills they need. However, few, if any, posts for general surgeons are being advertised, so, ironically, very few of these trainees will ever use their general surgical skills.
There are three stages to dealing with this problem. Newly appointed surgeons and current senior trainees urgently need training in endovascular surgery. Second, a program needs to be developed for trainees about to commence training, and, finally, we need to plan future training programs for clinicians responsible for delivery of vascular services in the future, the vascular specialist.
There has been considerable work undertaken by the United Kingdom Royal Colleges of Surgeons, together with the Royal College of Radiology, to develop high-quality training programs that will fulfill the needs of the vascular specialist both in the short term and, more importantly, in the longer term. This approach will not only prepare trainees for the future but will also focus and improve care for patients with peripheral arterial disease.
K. Craig Kent, MD
Weill Cornell Medical College and College of Physicians and Surgeons of Columbia University and Division of Vascular Surgery, New York Presbyterian Hospital, New York, New York
The training of vascular surgeons in the United States has evolved over the past 10 years. Although the specialty of vascular surgery has existed for decades, for many years, the majority of vascular procedures in this country were performed by general and/or cardiac surgeons. Trainees in most general surgical programs gained significant exposure to vascular procedures, allowing general surgeons to eventually perform vascular operations in practice. In 1982, however, the specialty of vascular surgery was recognized by the American Board of Surgery by the creation of a certificate of special qualifications in vascular surgery. This certificate is currently awarded to individuals who have gained additional exposure to vascular surgery through fellowship training. Requirements for receiving this certificate include participation in an approved vascular surgery fellowship and successful completion of a written and oral examination. Until recently, completion of a general surgery residency was a prerequisite for applying for vascular surgery fellowship.
As is the case in many areas of medicine, specialization has become the trend. There is a substantial amount of data particularly in the surgical realm that equates higher volume with improved outcome. In vascular surgery, a relationship between surgeon volume and outcome has been demonstrated with carotid endarterectomy as well as aneurysm repair. This relationship will likely become more profound as the complexity of our technology increases. No longer is an operation just “cutting and sewing.” Our procedures often involve complex technology that requires additional training and experience. In no specialty have techniques changed over the past several years as rapidly as vascular surgery. Treatments have evolved from complex open surgical procedures to catheter-based interventions. In the United States, this has required retraining of the entire vascular surgery workforce and the introduction into fellowship training programs of curriculum to teach catheter intervention.
This evolution has, as one might expect, profoundly influenced who performs vascular surgery. No longer is it possible for individuals who are primarily general or cardiac surgeons to perform the full array of vascular interventions. The evolution to catheter techniques has truly defined the specialty of vascular surgery. It is difficult for vascular surgeons to keep up with the new technology let alone surgeons who have as their major focus another type of surgery. As might be anticipated, the impact of this evolution on training has been substantial.
In response to this evolution and in 2006, vascular surgery training was completely revamped. This began with approval by the American Board of Medical Specialties in March of 2006 of a primary certificate in vascular surgery. The primary certificate now allows vascular surgeons in the United States to be trained by a number of innovative and diverse paradigms. The traditional program of 5 years of general surgery residency and 2 years of vascular surgery fellowship is still available. However, trainees can also choose from the following programs:
4 years general surgery/2 years vascular
3 years general surgery/3 years vascular
0 years general surgery/5 years vascular
Although we are early in the adoption of these new training paradigms, the 0/5 program appears to be the most popular. This mechanism for training enables medical students to choose a career in vascular surgery. Moreover, with this training program, one can become a vascular surgeon after only 5 years in training rather than the traditional 7. For the younger generation, these shorter periods of training have significant appeal.
Retraining of vascular surgeons already in practice in catheter-based intervention has also been a challenge. The majority of vascular surgeons in the United States have had to completely retool to accommodate the transition to catheter-based procedures. This has occurred at a reasonably rapid pace; however, there are challenges that still lie ahead. These will be discussed in detail in this presentation.
Giorgio M. Biasi, MD
John P. Fletcher, MD, MS, FRACS, FRCS, DDU
University of Sydney and Westmead Hospital, Sydney, New South Wales, Australia
The Royal Australasian College of Surgeons (RACS) provides training and education in nine surgical specialties with the recently introduced Surgical Education and Training (SET) program designed to improve quality and efficiency by early selection and streamlining of specialty training. Trainees apply directly into their specialty of choice and must fulfill eligibility criteria comprising (1) permanent residency or citizenship status of Australia or New Zealand, (2) graduation from a medical school recognized by Australian or New Zealand Medical Councils, (3) unconditional registration to practice in Australia or New Zealand, (4) a satisfactorily completed internship, and (5) clear criminal history check.
Vascular trainees are allocated to 1 or 2 years of general surgery followed by 3 to 4 years in an accredited vascular unit in Australia or New Zealand (rotating to a different unit each year).
The areas of study in vascular surgery are divided into two levels. Level 1 includes basic sciences, diagnosis and diagnostic tools, and professional matters, with these topics needing to be covered prior to completion of the first vascular year of training. Level 2 is more clinically based and consists of modules relating specifically to vascular diseases by body region, venous disease, graft infections, and vascular medicine, including the role of cardiovascular drugs in vascular surgery.
Trainees can sit the RACS final fellowship examination after demonstrating completion of training modules, fulfilling the requisite caseload for open surgery, endovascular interventions, and ultrasound examinations, together with satisfactory progress reports from their supervisors of training.
DEBATE: The Future of Vascular Surgery Training
17.12 Combined Cardiac and Vascular Training Pathways
Mark G. Davies, MD, PhD
Department of Surgery, University of Rochester, Rochester, New York, USA
17.19 Combined Interventional and Radiology Training in the United Kingdom
Cliff P. Shearman
Department of Vascular Surgery, Southampton
General Hospital, Southampton, United Kingdom
The development of endovascular interventional techniques, together with a greater understanding of the importance of the medical therapies, has transformed the treatment of patients with peripheral arterial disease.1,2 Clinicians treating this high-risk group of patients need to be able to offer a complete range of medical and interventional treatment. This service also needs to be available 24 hours a day. Currently, care is delivered in a fragmented way by primary and secondary care and is not available out of hours in up to 25% of UK units. Diagnostic and interventional treatments are delivered by interventional radiologists and vascular surgeons. The majority of surgical trainees want exposure to endovascular surgical techniques, but radiologists have to provide a large range of interventional services and potentially see surgeons taking on endovascular surgery as cherry picking. There is also concern about the level and quality of training surgeons are receiving.
Current training in the United Kingdom requires radiologists and surgeons to complete training in general radiology and surgery, respectively, limiting the opportunity to fully develop the skills they will need in the future to provide a modern vascular service. There is considerable overlap in the knowledge base, clinical skills, and attitudes required by vascular surgeons and interventional vascular radiologists. In the United Kingdom, there has been considerable progress in collaborating to produce a syllabus and curriculum for radiology and vascular surgical trainees. This has been fostered by a working group from the Royal Colleges of Surgeons of England, Edinburgh, and Glasgow and the Royal College of Radiologists. Much of the training program overlaps. It is envisaged that, initially, radiology trainees will gain some clinical competencies in surgical areas such as wards, and outpatients and surgical trainees will gain experience in basic radiology techniques. The trainees can then build on this experience as their training progresses, allowing them to select areas for which they appear to be best suited as well as what future services require.
As training in this program is mapped by the curriculum and objective tools to assess a trainee's competence and progress, it removes concerns about variability in quality of training. All trainees will have both a radiologic and a surgical trainer. This approach will allow the development of specialist teams to deliver high-quality vascular care and will also allow adaptation of the role of specialist training for the future to meet service needs.
Although peripheral arterial disease is very common, it tends to be treated by a range of different clinical groups, and there is wide variation in therapies and interventions available in different hospitals. Up to 30% of admissions for arterial disease are emergencies, and the provision of services for these is even less predictable, with large variations in access to vascular specialists. Partly because of these problems, the needs of patients with PAD tend to be underrepresented compared with other groups, such as those with coronary artery disease, which results in fewer resources to treat PAD. Specialist teams with strong links to primary care would raise the profile of PAD and address many of these problems.
Training specialists is expensive, so the training must be focused on producing an individual who is trained to be fit for purpose–-in other words, who will be equipped to provide a modern vascular service in the future and, from the trainee's point of view, must be employable. Medical unemployment due to overproduction of specialists in some area has become a reality. It is essential to plan the future workforce and train the correct number of vascular specialists
Talks between the Royal College of Radiologists and the Royal Colleges of Surgeons of England, Edinburgh, and Glasgow have been ongoing for several years. The incentive for these discussions was the recognition of the above factors and a desire to strengthen the future of both specialties on the basis of provision of high-quality service through the development of a joint training scheme. In the United Kingdom, vascular surgeons and interventional radiologists need to complete general surgical or radiologic training before pursuing their true career interest. Few then take part in delivering general surgery or radiology services and, even if they do, quickly lose their competencies in these areas due to low volume of cases. Although there are a number of generic skills and knowledge that are essential, evidence suggests that these should be gained early on in training. This allows more time for trainees to focus on specialist training relevant to their chosen career pathway. This concept fits well with the proposals following recent review of medical training in the United Kingdom. 6 This has the potential attraction of producing doctors with higher levels of competence at the time of completion of specialist training and reducing the need to “learn on the job.” Such changes can only benefit patients!
The starting point for planning a new training pathway was to consider the optimal end point of training from the patient perspective. Patients want high-quality care from initial presentation and diagnosis through to the discussion and provision of potential treatment options. Patients are not interested in whether the doctor providing their care is called a surgeon or a radiologist or a “vascular specialist.” As results with a particular technique are usually related to the caseload, it is unlikely that any individual would be equally proficient in “all” treatment options. Hence, training should produce teams of “vascular specialists” who between them possess all of the skills necessary to provide this care. These teams should include appropriate numbers of doctors capable of providing open surgery and interventional therapy but also able to adapt to future changes in delivery of service.
When viewed from the perspective of vascular surgery, this ensures both the future and the quality of the specialty. Removing obligations to spend time and be examined in specialties that they will never practice will allow doctors opting to take the vascular surgical training modules to have more time to develop vascular surgical skills. Some vascular surgeons worry that modern medical therapy and minimally invasive techniques will reduce their workload and threaten their professional future, as has happened in cardiac surgery. In reality, medical therapy will not in the foreseeable future prevent all vascular disease and endovascular techniques will not be suitable or possible in all patients. Hence, as the population becomes older, more obese, and diabetic, there will be a need for more doctors who are able to perform what will be increasingly complex vascular surgery.
From the radiology point of view, this increases the number of doctors gaining exposure to interventional radiology and is likely to increase recruitment. More importantly, increased training in interventional techniques is essential to ensure provision of the emergency safe interventional radiology, including interventional management of urologic and hepatobiliary emergencies. Vascular specialist training will ensure that the endovascular practitioner of the future is competent across the full spectrum of complex vascular interventions. In this respect, we must recognize that although peripheral vascular intervention is the core activity of the vascular radiologist, the elective workload has grown to encompass many other specialties. At the same time, the nature of emergent endovascular work now mainly relates to the management of hemorrhage in the context of gastrointestinal bleeding and trauma.
We believe the most attractive aspect of such a joint training program is that it will bring together trainees in surgery and radiology who will be providing vascular services together in the future and evolve into vascular specialists.

Potential training pathways for surgery, radiology, and the vascular specialist. Arrows indicate potential routes that can be followed (for clarity, the link between core ST and radiology has been omitted). CCT = certificate of completion of training; MT = medical training; ST = surgical training.

Example of a 3D Road Map.
Workplace-Based Assessments to Be Used for Formative and Summative Assessment during Joint Training
Competence, knowledge, and professional skills will also be assessed by a combination of workplace assessments, taught courses, and examinations. This means that on completion of a successful training program, the trainee could clearly demonstrate that they had acquired the appropriate competencies to treat a specific condition, for example, carotid artery disease.
Improved patient care is the driving force behind
Changes in training
Changes in service delivery
“Cross-specialty” training schemes will
Encourage focused but flexible training
Allow the final career path to be influenced by individual aptitude, preference, and workforce planning
Deliver teams of experts to provide comprehensive patient care
17.26–17.36 Voting and Panel Discussion
SESSION V: The Future of Vascular Surgery
Moderators: Frank J. Veith, MD, Jerry Goldstone, MD, FACS, FRCSE, James C. Stanley, MD
James C. Stanley, MD
University of Michigan, Ann Arbor, Michigan, USA
Specialty-centric competition and conflict in the care of vascular disease are common causes of dysfunctional professional efforts and a source of increasing health care costs in the United States. The University of Michigan recently created a broad-reaching practice and business model of cardiovascular care that disfavors turf battles and silo practices.
The University of Michigan Cardiovascular Center encompasses more than 120 full-time physicians from the disciplines of vascular surgery, cardiac surgery, cardiology, interventional radiology, stroke neurology, and anesthesiology. To facilitate a global change in practice, these clinicians were presented with a new 350,000 square foot freestanding building in 2007. This facility includes physician offices and conference rooms, 36 clinics, 14 invasive laboratories, 10 surgical suites, 24 intensive care unit beds, and 24 inpatient beds for vascular surgery patients. The annual activity encompasses nearly 50,000 outpatient visits, 6,000 admissions, 130,000 noninvasive procedures, 1,400 open heart procedures, and close to 4,000 vascular surgery and endovascular interventions, all of which generate more than $190 million in revenue, with a $63 million margin (USD).
The Cardiovascular Center business plan is such that the hospital's profit margin and professional revenue margin are pooled and redistributed to the various constituencies, including clinicians, to develop new treatment paradigms as well as scholarly investigative programs. Seven collaborative teams, with individuals from all specialties involved with a given patient's illness, have been established. Funding for innovative projects to these teams will be distributed by the Cardiovascular Center directors (two cardiologists, one vascular surgeon, and one cardiac surgeon) from a $50 million (USD) philanthropic fund. The latter monies were given by a benefactor wishing to see elimination of competing practice patterns. These funds are solely controlled by the members of the Cardiovascular Center, without interference from the hospital or medical school.
The physicians of the Cardiovascular Center have accepted the basic tenet that financial issues separating specialty practices are often a source of contention. The ability to incent practitioners across disciplines to benefit from their joint expertise has provided an impetus for seamless patient-centric care.
K. Craig Kent, MD
Weill Cornell Medical College and College of Physicians and Surgeons of Columbia University and Division of Vascular Surgery, New York Presbyterian Hospital, New York, New York
The number of people with peripheral vascular disease has grown exponentially, from 1980 to 2000; interventions for vascular disease have more than doubled. With our aging population and the availability of minimally invasive therapies, it is anticipated that this rate of growth will continue. Technological advances have made the treatment of patients with vascular disease one of the fastest moving and most exciting areas of medicine. We now have the ability to treat more patients with less risk. The foregoing would suggest that our specialty should be at its pinnacle.
However, the outlook is not all positive. We are being paid less for our services despite working harder. Malpractice rates are out of control. Treatment paradigms are changing, and it has become necessary for surgeons to learn an entirely new set of skills. Despite the fact that vascular surgeons have been the sole providers of vascular care for almost 50 years, other specialists have learned and mastered techniques that are now used to treat our patients. Thus, it is no surprise that today's vascular surgeon is consumed with the task of just keeping up. Retraining has become paramount for those who had not yet learned catheter techniques. The political issues related to access to catheter-based intervention can be all-consuming. Then there is the simple issue of just doing enough cases to maintain one's economic viability. With all of these issues facing vascular surgeons, it seems that the motivation for research has waned. How can one think about something as remote as research at a time when it seems that the sky is falling?
Perhaps it may be worth reflecting on the reasons why we are in this predicament. During the first 40 years of the existence of our specialty, we led the way. Voorhees’ prosthetic vascular graft was a novel concept in the 1950s. I am certain that using a piece of clot to replace a patient's aorta was initially troubling to many (perhaps as concerning as was carotid stenting when this technique was first introduced). However, from the invention of operations such as carotid endarterectomy and aneurysm repair to the perfection of these and many other procedures, vascular surgeons during these early years were the only force in vascular innovation and research. Although we continue to play a dominant role in the treatment of patients with peripheral vascular disease, over the past few years, we have relegated the research and development of many new techniques to other specialists. Recall that the vascular stent (an invention that has now worked its way into our daily practices) was conceived in the mid-1980s by an interventional radiologist. Studies reporting the outcome of renal stenting were and still are dominated by interventional radiologists and cardiologists. There are over 200 manuscripts in the literature on carotid stenting, and only a handful are primarily authored by vascular surgeons. Although angiogenesis has not yet come of age, cardiologists have pioneered its use in the peripheral circulation. There are reasonable excuses for our not participating in the initial development of many of these techniques. For example, some of the devices and treatments that we currently use were initially designed for coronary circulation. Alternatively, if our specialty had led the exploration of innovative minimally invasive treatments for peripheral vascular disease, there would be no need to retrain. The moral of the story is that research in vascular disease will continue, with or without vascular surgeons.
DEBATE: Vascular Surgery Independence
17.50 We Have More in Common with Cardiologists, Cardiac Surgeons, and Interventionalists. Our Differences with General Surgery are Too Great to Sustain a Meaningful Relationship.
Frank J. Veith, MD
17.57 We Must Not Cut Our Ties and Become Extinct before We Exist: There is Room for Self-governance under the Watchful Eye of General Surgery.
Martin Feeley
18.04–18.15: Voting and Panel Discussion
Honorary Address and Life Achievement Award
Peter R.F. Bell, MD, FRCS, DSC, KBE
Honorary Award
Western Vascular Institute is proud to honor
Sir Peter R.F. Bell, MD, FRCS, DSC, KBE
with
The Award will be presented to Sir Peter by the distinguished Professor Frank J. Veith.
Sir Peter's distinguished career has been full of achievements that are testament to his commitment to the development of vascular surgery. He was quick to recognize the advances in medical treatments and the need for minimally invasive techniques, which allow us to broaden our indications for intervention and facilitate definitive management of high-risk patients. He is indeed one of the forefathers of modern endovascular therapy and a true champion of endovascular techniques, most notably subintimal angioplasty.
In his capacity as ISVS president, he has been dedicated to the promotion of vascular surgery as a defined specialty, separate and distinct from general surgery. Under his leadership, the ISVS has forged international ties, which serve to strengthen the global vascular community. With our combined forces, we are better placed to establish independence and to arrange our own training.
His commitment to the provision of training programs that provide adequate training in open surgery, endovascular surgery, and medical therapy and his acknowledgment of the need for self-governance with credentialing standards and practice guidelines will ensure that all vascular surgeons are able to provide a comprehensive range of safe vascular treatments. Thanks to his visionary thinking, vascular surgeons will now be able to publicize the fact that we are the doctors who can best deal with vascular disease.
7.00–8.00 Breakfast Symposium in conjunction with Smith & Nephew
Georgina Gethin, PhD, RGN, HE Dip wound healing, Dip Anatomy, Dip Applied Physiology. Research Centre, Faculty of Nursing and Midwifery, Royal College of Surgeons in Ireland, Dublin, Ireland
The prevalence of chronic wounds is set to increase, due in part to increase life expectancy, increased incidence of diabetes, survival from major surgical interventions together with other injuries such as burns and trauma wounds. The main contributor to the challenges in managing such wounds is that they are all characterized by varying underlying etiology and many exhibit inability for clousure with standard wound management modalities.
Chronic wounds fail to heal in an orderly timely fashion. They are highly alkaline, are noted for the presence of cellular senescence, and many are hypoxic and have high rates of infection. Assessment of these wounds is often based on subjective interpretation of the wound bed with little recourse to objective analysis. The ability to measure the healing progress is of great importance and objective methods are required for comparative results and analysis of treatment efficacy. Measurement of wound area aids objective analysis but, there is a lack of other diagnostic instrumentation that can lend itself to routine use in the clinical setting. The monitoring of surface pH of the wound may potentially contribute to such analysis as failure of both acute and chronic wounds to heal has been demonstrated to be almost invariably correlated with alkaline pH.
Chronic non-healing wounds have pH values of 7.8 to 8.9. Many studies have reported reduction in pH with the application of topical agents and appropriate dressing selection. Further studies have demonstrated significant reduction in wound size of up to 39% in 2 weeks when pH is < 7.6 with the wound increasing in size when pH is > 8.0. Other research has demonstrated that a 0.1 unit reduction in pH is associated with an 8.1% reduction in wound size over a 2-week period.
Movement of pH from alkaline toward acidic has many effects including a shift to the right of the oxygen-hemoglobin dissociation curve; reduced histotoxicity of bacterial end products including ammonia; enhanced destruction of abnormal wound collages; decreased protease activity; promotion of angiogenesis; increased macrophage and fibroblast activity and control of enzyme activity.
Current research data show evidence of a scientific basis to topical application of pH modulating agents in promoting wound healing, particularly in wounds previously unresponsive to standard care. This paper will explore the challenges in using pH to monitor wound healing and outline the research work completed to date in this area.
Mo Baguneid, MB ChB, FRCS(Gen) University Hospital South Manchester NHS Foundation Trust
The Versajet hydroscalpel (Smith & Nephew) has been described as a useful tool in the management of diabetic foot ulcers. Arterial ulceration is usually considered painful and often has significant slough and necrotic tissue at its base. We will describe cases in which patients with revascularized arterial ulceration have subsequent débridement using the Versajet hydroscalpel (Smith & Nephew). This ward-based treatment involved no anesthetic and was well tolerated. Wound healing was accelerated by application of a VAC system (KCI). Alternative treatment options would have included larval therapy, standard desloughing dressings, or surgical débridement in theater. Many patients who present with critical limb ischemia and ulceration require distal angioplasty. Revascularization may only be of short-term benefit; therefore, it is crucial that early epithelialization occurs. Delayed ulcer healing and skin maceration while using alternative forms of ulcer treatment can result in failure of complete ulcer healing before the effect of elastic recoil and restenosis of tibial vessels results in further ischemia ensuing.
SESSION VI: Vascular Screening and Imaging Techniques: The Benefits of Early Detection and the Latest Imaging Modalities for Optimal Management
Moderators: Mark G. Davies, MD, PhD, DieterRaithel, MD, PhD
Mark G. Davies, MD, PhD Department of Surgery, University of Rochester, Rochester, New York, USA
Access to a portable C-arm was a transforming technology, which provided vascular surgeons with realtime fluoroscopy, digital subtraction angiography, and road mapping. These were the platforms that permitted the specialty to transform into performing endovascular procedures. The establishment of high-volume endovascular activities also propelled vascular surgeons toward the acquisition of fixed imaging systems, which provide an excellent image quality, with their capability of performing rotational angiography and 3D reconstruction. These capabilities have in turn led the imaging companies to develop even more remarkable image acquisition sequences:
3D reconstruction and 3D road mapping
3D road map that autocorrects based on image intensifier movement
Fluoro-CT
Registration and overlay of previously acquired 3D reconstructed CT scans
These are remarkable new capabilities that the vascular surgeon will need to understand. Not only are these new imaging modalities useful at the present and being incorporated into all new fixed imaging systems, they also form the core platform, which will permit complex navigation systems to be developed. The process for this is as follows:
A 64-slice CT angiogram is performed preprocedure.
The patient is placed on an angio table and a fluoro-CT scan is performed.
Fluoro-CT is used to register the previously acquired (high resolution) CT on the patient.
The CT angio is overlaid on the fluoro image and used to guide the intervention.
This capability is what is driving many current developmental efforts to permit remote navigation of catheters. This includes magnetic navigation (Stereotaxis) and robotic navigation (Hansen Medical). Both of these systems have received FDA approval for use in electrophysiology and are currently being evaluated for use in the peripheral vasculature. Both systems can be used with current fluoroscopic imaging. However, the true capability promises minimal wall contact navigation and remote steering of wires and catheters by an operator removed from the radiation field.
Max Amor, G. Ethevenot, C. Breton, J.P.S. Simon, Z. Chati Cardiovascular Department, Clinic Louis Pasteur, Essey les Nancy, France
One of the most interesting developments introduced in last-generation angiography systems is rotational angiography, which involves a high-speed rotation of the tube intensifier complex (4.0 seconds for 220þ and a collection of 120 views) simultaneously to the injection of contrast medium (usually 20 to 30% more than a standard view of biplane angiography). This enables visualization of the vessel from numerous angles in less than 20 seconds, as well as 3D quantification of stenosis and aneurysm without calcium interferences (Figures 1 and 2).

External Steering Magnets which adjust a magnetic field to deflect a magnetically enhanced guide wire (Stereotaxis).
The speed of the acquisition and of the processing as well as the analysis (length, diameter, distance, and superposition) not only allows a better description of the lesion(s) but also prepares accurately the endovascular time that could follow the diagnostic rotation using 3D road mapping.
The determination of the working projection has become essential in our practice for several conditions: best view: to avoid superposition, to visualize a stump, and to follow a recanalization.
The precision of the measurement with a resolution of less than 0.1 mm is providing the most accurate tool to measure the diameter and the length of the stent required as well as to assess the results (Figures 3 and 4).

The joy stick controller of The Hansen system is used to control a catheter which is moved by a robotic catheter control system. A virtual catheter is overlaid on to the fluoroscopic image
This system was mainly developed for the study of the intracranial artery circulation, but there have also been preliminary experiences at the extracranial level. At the neck, thoracic, abdominal, and pelvic levels, the worldwide experience is limited, and the protocol of uses varies from center to center.
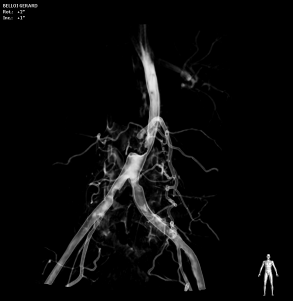
Severe abdominal aortic stenosis.

Posterior false aneurysm of abdominal aorta.

Severe abdominal aortic stenosis before and after implantation of a S-E stent.
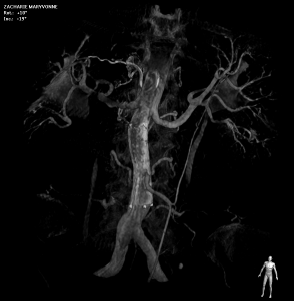
Severe abdominal aortic stenosis before and after implantation of a S-E stent.
During the 9 months we have been using the system, we have not encountered significant false-positives or false-negatives in term of diagnosis. We have found the technology very helpful during carotid stenting, abdominal aorta stenting, aortoiliac recanalization, ostial common iliac stenting, internal iliac angioplasty, common femoral angioplasty, and proximal SFA.
The mentally reconstructed images are different from the anatomic reality. Day by day, in our department, where two Philips systems have been installed, we perform more and more–-at first the 3D RA to assess the complex anatomies. This allows us, in less than 5 minutes and with less than 100 cc of contrast medium, to recognize quickly the culprit lesions, to measure the severity of the stenosis, to determine the parameters of the stent, and to choose the access way and the working projection.
3D RA is already considered a major breakthrough in neuroradiologic interventions. Its role for peripheral interventions is very promising and could become essential in the very near future.
Rodney A. White
K. Craig Kent, MD
Weill Cornell Medical College and College of Physicians and Surgeons of Columbia University and Division of Vascular Surgery, New York Presbyterian Hospital, New York, New York
Aneurysmal disease is a devastating problem that each year produces tremendous mortality and morbidity worldwide. In the United States alone, large data sets have shown that over 15,000 people die of ruptured aneurysms each year. However, this is likely an underestimate of the extent of the problem since, each year, an additional 200,000 individuals in the United States die suddenly. Although a cardiac etiology is the culprit in the majority of these patients, autopsy studies have shown that approximately 5 to 7% of individuals with sudden death die of a ruptured aneurysm. Thus, the total number of deaths in the United States from ruptured aneurysms likely approaches 30,000 per year. This number can be compared with a death rate of 40,000 per year for breast cancer or prostate cancer. Thus, aneurysmal disease represents a significant health problem, and effective screening for aneurysms has the potential to save many lives.
Death from AAA is preventable. In fact, all that is required to diagnose this problem is a simple sonogram. Albeit ultrasound has been used in the diagnosis and evaluation of AAA for many years, a conventional sonogram for AAA requires 30 to 40 minutes of scanning time, and the cost ranges from $150 to over $250. A few years ago, the concept of a quick screen was popularized. The ultrasonographer answers yes or no to the question of whether an aortic dilation greater than 3 cm is present. With an experienced ultrasonographer and a cooperative patient of appropriate habitus, this question can often be answered in just a few minutes, with minor cost and minimal patient discomfort.
When evaluating the utility of a screening test, a number of factors are important. These include (1) the cost of the test, (2) the morbidity associated with the test, (3) the prevalence of disease in the population to be screened, (4) the cost and mortality of the disease if left undiscovered, and (5) the cost and mortality if the disease is diagnosed and appropriately treated. If one applies these criteria to screening for AAA, the analysis is quite favorable. A quick screen sonogram is a convenient study that is inexpensive. The prevalence of aneurysmal disease varies with the population chosen for screening. However, in select populations, prevalence is high. If aneurysms rupture, the mortality is greater than 85%, and the morbidity and cost are tremendous for those who survive. Alternatively, elective repair of aneurysms, either by open or endovascular techniques, is now associated with low early and late mortalities and morbidities. Thus, aneurysmal disease, by all measures, is ideally suited to screening.
Cost-effective analyses have been used to evaluate the appropriateness of screening for aneurysmal disease. A number of investigators have incorporated the previously mentioned factors into Markov models, a methodology used to evaluate the cost-effectiveness of interventions. In one such analysis, screening for aneurysmal disease was associated with a cost per quality-adjusted life-year saved of $11,285; the cost per quality-adjusted life-year saved is the cost required for an intervention to extend a person's life 1 year. For comparison, the cost-effective ratio for coronary artery bypass for left main disease is $9,500. The cost-effectiveness ratios for screening for prostate or breast cancers are $100,000 and $20,000, respectively. Alternatively, the cost-effective ratio for liver transplant, a commonly performed and well-accepted intervention, is $136,900. Thus, in terms of life-years saved integrated with cost, AAA screening is an intervention that compares favorably with other common procedures currently reimbursed by our medical care system.
Additional compelling evidence of the value of AAA screening can be derived from the Multicenter Aneurysm Screening Study (MASS). MASS was a prospective randomized study conducted in England in the late 1990s in which male patients, ages 65 to 74, were randomized to screening or not. Of approximately 70,000 patients identified, 2,500 were excluded because they were unfit for surgery; even if an aneurysm were to be found, repair would not be recommended. Approximately 34,000 patients were invited for screening, and another 34,000 were not. The acceptance rate for the invitation for screening was approximately 80%, highlighting that compliance is an important factor when determining the effectiveness of screening tests. In the patients screened, 1,333 aneurysms were identified. Nine hundred forty-four were 3.0 to 4.4 cm in size, 223 were 4.5 to 5.4 cm in size, and 166 were greater than 5.5 cm in diameter. The mortality associated with elective aneurysm repair was approximately 6%, higher than what might be encountered in current practice. Nevertheless, even with the high mortality associated with repair, over a 4-year period, the authors found a 42% reduction in aneurysm-related mortality in patients screened for AAA.
Despite the seemingly compelling evidence of the effectiveness of screening for AAA provided by these and many other studies, insurers, including Medicare, until recently did not reimburse for screening of aneurysms or, for that matter, any form of vascular disease. In the absence of reimbursement, a number of “for profit” companies were formed that offered screening for AAA as well as carotid artery and lower extremity vascular disease. These companies have been quite successful and have screened millions of patients at a cost of just over $100 for all three tests. The most successful of these companies is Life Line Screening, which has screened over 6 million individuals for vascular disease since 1993. Despite the success of Life Line and other companies, this is still a fraction of the individuals at risk. Moreover, those patients with advanced cardiovascular disease may be less likely to be aware that they are at risk and thus unlikely to personally pay for screening. Widespread screening for AAA is unlikely to occur without the availability of reimbursement from insurers.
Consequently, in 2004, the National Aneurysm Alliance was organized by the Society for Vascular Surgery (SVS) with the coparticipation of multiple professional and private organizations as well as industry. What subsequently ensued was an aggressive lobbying campaign that resulted in the introduction of a bill in Congress to provide Medicare-funded screening for aneurysms in appropriately targeted beneficiaries. One of the important steps in encouraging Congress to consider payment for AAA screening was the favorable assessment rendered by the United States Preventive Services Task Force (USPSTF). After an extensive evaluation, the Task Force recommended screening for the subpopulation of patients that includes ever-smoking males age 65 to 74. With the Task Force recommendations in hand, the SVS led its coalition members in an aggressive targeted lobbying campaign throughout 2005. As a result of these efforts, and in recognition of the obvious beneficial impact of AAA screening in at-risk beneficiaries, Congress passed the SAAAVE Act (Screen Abdominal Aortic Aneurysms Very Efficiently) late in 2005 with implementation targeted for 2007. Ironically, this measure was included as a provision within the much larger Deficit Reduction Act of 2005 (DRA). Since Congress was not in a spending mood when it passed the DRA, there are tight restrictions associated with SAAAVE. Medicare-funded AAA screening is limited to male ever-smokers. Unfortunately, the physical is available to beneficiaries only during their first 6 months in the Medicare program. The AAA screening benefit was implemented in January 2007, and we will have the initial year's uptake numbers by mid-2008. In addition to the CMS benefit, several private insurers have followed suit with creation of AAA screening programs for targeted policy holders.
Some advocates of screening, the authors of this article inclusive, feel that the ruling by the USPSTF was too conservative. The Task Force rejected screening males under 65 or older than 75. Additionally, the Task Force did not recommend AAA screening for any women, for any male nonsmokers, or for individuals with a family history of AAA. Admittedly, studies have shown that the vast majority of patients who develop aneurysmal disease have a history of smoking, although this is not exclusively the case. Somewhat surprisingly, the task forces assigned screening for AAAs in women a D rating, meaning that they believe that the potential harms of AAA screening exceed potential benefits.
Although the ruling by the USPSTF and the bill passed by Congress were victories for advocates of AAA screening, several issues have limited the success of this effort. As noted, Congress limited screening to new beneficiaries, effectively reducing the window of opportunity to those individuals who are just turning 65. Consequently, hundreds of thousands of at-risk individuals who are currently older than 65 have not been allowed to participate in this benefit. Equally important, the newness of the welcome to Medicare physical has very much dampened participation. For example, in 2005, the year of introduction of the Welcome to Medicare Physical, only 30,000 patients participated in this program, which is less than 5% of those individuals in this country turning 65 and eligible for Medicare. The frequency increased to 72,000 in 2006, about 15% of new beneficiaries. However, it is clear that large numbers of patients at risk for aneurysmal disease remain unscreened.
The issue of screening for AAA in women is complex. Without doubt, the prevalence of AAA in women is lower than in males, with an approximately 4 to 1 ratio. However, rupture of aneurysms in women is not a remote event, and the likelihood exists that subsets of women are at high risk for the development of aneurysms. The epidemiology and behavior of AAAs in women clearly vary from those of men. Women develop aneurysms at an older age than men, albeit women, on average, live 5.7 years longer than men. Thus, because of their increased longevity, perhaps women should be considered for aneurysm repair at an age greater than what would seem appropriate in men. Women also suffer AAA rupture at a size smaller than men; it has therefore been suggested that repair be considered in women at a size of up to 0.5 cm less than what is considered appropriate for men. Two recent studies have shed further light on this issue. Anders Wanhainen and colleagues recently published an elegant cost-effectiveness analysis related to aneurysmal screening in women. Considering these and other factors, these authors found that screening indeed was cost-effective in women. A recent study of over 10,000 women screened for AAA also demonstrated that a cohort of women with multiple cardiovascular risk factors is at high risk for the development of aneurysmal disease. Although more data are necessary, it seems reasonable to assume that AAA screening will be applicable to a subset of women. The specific identification of this cohort will need to be the focus of future investigations.
It could be argued that since AAA screening is inexpensive, it might not matter if it is reimbursed by insurance. The cost of an AAA screening sonogram is somewhere in the range of the cost of a large family meal at McDonalds. Evidenced by the success of Line Line Screening, there are many individuals willing to pay to be screened. However, without reimbursement, it is likely that only those individuals who are motivated and aware of their health issues will search out screening for AAA disease. Unfortunately, these individuals may be the ones who are least likely to be at risk.
Although tremendous progress has been made over the past several years regarding screening for AAA, there is still a great amount to be learned. Is there a subset of women who should be screened? Can we better define the population of nonsmoking males whose AAA risk is sufficient to merit screening? Should screening be expanded to other forms of vascular disease? Despite recent progress, patient access to screening remains limited. All ever-smoking men in the Medicare program greater than age 65 should have coverage for aneurysm screening, not just those who have turned 65. At a minimum, AAA screening should be uncoupled from the Welcome to Medicare physical examination until that benefit achieves wider acceptance.
There is little doubt that more research is necessary. Recently, the SVS developed a partnership with Life Line Screening that will allow the analysis of screening data from over 5 million individuals. All of these people were screened for AAA, carotid artery disease, and lower extremity vascular disease. It is likely that the findings of this analysis will allow a clearer definition of the cohort that will achieve greatest benefit from screening for each of the forms of vascular disease.
It is important to note that the mere availability of the test does not ensure that patients at risk will be screened. In MASS, only 80% of patients were eventually evaluated for AAA despite being contacted twice by their physicians. Screening, even if reimbursed, will not be widely performed unless there is increased awareness of AAA and the benefit of screening among patients and their primary care physicians. Whereas most individuals in this country are aware of the risks of breast and prostate cancer, few know what an aneurysm is, let alone who needs to be screened for AAA. Thus, public awareness is a necessary component of any effort to increase the number of individuals screened. All of these issues aside, there is little doubt that the efforts of the SVS and other interested organizations have yielded significant progress in screening for vascular disease. There is more to come!
8.28–8.38: Discussion
SESSION VII: Contemporary Management of Thoracoabdominal Aortic Aneurysms: Can Endovascular Technology Give Sustainable Results?
Moderators: Jacob Buth, MD, Rodney A. White, MD
Sean O'Neill
Carlos H. Timaran, Eric B. Rosero, MD, J. Gregory Modrall, MD, James Valentine, MD, Patrick Clagett, MD University of Texas Southwestern Medical Center, Plano, Texas, USA
DEBATE: Modern Management of Thoracoabdominal Aortic Aneurysms
Jaap Buth for the Dutch Collaborators
Not every patient is fit for open thoracoabdominal aortic aneurysm (TAAA) repair, nor is every TAAA or juxtarenal abdominal aortic aneurysm suitable for branched or fenestrated endovascular exclusion. The hybrid procedure consists of debranching of the renal and visceral arteries followed by endovascular exclusion of the aneurysm and might be an alternative in these patients.
Between May 2004 and March 2006, 16 patients were treated with a hybrid procedure. The indications were recurrent suprarenal or thoracoabdominal aneurysms after previous abdominal and/or thoracic aortic surgery (n 5 8), type I to III TAAAs (n 5 3), proximal type I endoleak after endovascular repair (n 5 2), penetrating ulcer of the juxtarenal aorta (n 5 1), visceral patch aneurysm after type IV open repair (n 5 1), and primary suprarenal aneurysm (n 5 1). Eight (50%) of 16 patients were judged to be unfit for open TAAA repair.
The hospital mortality rate was 31% (5 of 16). Four of five deceased patients were unfit for thoracophrenic laparotomy. Two patients died from cardiac complications and three from visceral ischemia. No spinal cord ischemia was detected, and temporary renal failure occurred in four patients (25%). The mean follow-up was 13 months (range 6–28 months). During follow-up, no additional grafts occluded and no patients died.
Hybrid procedures are technically feasible but have substantial mortality (31%), especially in patients unfit for open repair (80%). They might be indicated when urgent TAAA surgery is required or when vascular anatomy is unfavorable for fenestrated endografts in patients with extensive previous open aortic surgery.
Nicholas J. Cheshire
9.06–9.16 Voting and Panel Discussion
James C. Stanley, MD
University of Michigan, Ann Arbor, Michigan, USA
Niamh Hynes, Sherif Sultan
Western Vascular Institute, Department of Vascular and Endovascular Surgery, University College Hospital, Galway; The Galway Clinic, Doughiska, Galway, Ireland
We are witnessing metamorphosis in open AAA repair, and, currently, the majority are pararenal aneurysms. We aim to assess whether single suprarenal artery clamping alters technical and clinical outcome in pararenal aortic repair (PRAR) and evaluate the risks associated with increasing anatomic and comorbid complexity.
Of 130 consecutive open AAA repairs from 2002 to 2005, 70 were infrarenal aortic aneurysm repair (IRAR) (32 emergent eIRAR) and 60 PRAR (26 emergent ePRAR). We performed a parallel-group comparison of elective and emergency PRAR and IRAR in a tertiary referral university center. All suprarenal AAA had left renal vein division.
Comorbidity scores were similar, and groups were matched for age and gender. The mean aneurysm size was larger in the PRAR group compared with the IRAR group (6.7 ± 1.4 cm vs 6.1 ± 1.1 cm, p = .036). However, the mean diameter was similar for emergency repair groups.
Perioperative mortality was analogous for elective IRAR and PRAR (2.7% vs 5.9%, p = .594). Emergency perioperative mortality rates were statistically similar (eIRAR 21.9% vs ePRAR 11.5%, p = .487).
The 5-year elective survival rate for IRAR was 86.1% and for SRAR was 72.0% (p = .403). The 5- year emergency survival rate for ePRAR (64.3%) was comparable to eIRAR (53.4%) (p = .796).
Perioperative freedom from MACE was akin to elective repair (IRAR 94.7% vs SRAR 79.4%, p = .075, RR = .26) and emergent repair (eIRAR 68.7% vs ePRAR 57.7%, p = .422, RR = 0.74). Postoperative renal impairment rates did not vary (IRAR 5.1% vs PRAR 2.9%, p = .644; eIRAR 25% vs ePRAR 33%, p = .503). Using multivariate analysis, diabetes was associated with adverse outcome (p = .02).
Despite the complexity of current open AAA in the endovascular era, we have not had an escalation in perioperative or long-term MACE. When we equate PRAR to IRAR, survival rates and long-term renal function are not compromised with single renal clamping, left renal vein transfixion, minimal visceral-ischemia time, and perioperative pharmacologic manipulation.
Chris Beirne, Niamh Hynes, Sherif Sultan
Departments of Vascular and Endovascular Surgery, Western Vascular Institute University College Hospital, Galway, and The Galway Clinic, Galway, Ireland
Peripheral limb trashing was noted in five patients (9.4%) in the noniloprost group compared with no patients who received iloprost. Increased rates of acute renal failure and bowel complications were noted in those who did not receive iloprost. ICU stay was greater than twice that of iloprost patients. All-cause morbidity affected 67% of patients not receiving iloprost compared with 40% who did. Survival rates were significantly better with iloprost than without in both 30-day (p < .05) and 5-year cumulative survival (p = .0187, h = 0.20, 95% CI = 0.05–0.76).
Wael Tawfick, M. O'Connor, Sherif Sultan Western Vascular Institute, Department of Vascular and Endovascular Surgery, University College Hospital, Galway, Ireland; The Galway Clinic, Doughiska, Galway, Ireland
The Continuous Autotransfusion System (CATS) conserves the use of allogenic blood. We present our experience using CATS in open abdominal aortic aneurysm (AAA) repair (elective and emergent) over 9 years in a tertiary referral center.
Primary end points were packed RBCs transfused, morbidity, and mortality. Secondary end points were length of ICU stay, hospital stay, and cost-effectiveness.
From June 1997, 187 patients underwent open AAA repair. Allocation to CATS was based on availability of a hemovigilance technician. One hundred one patients receiving CATS were reinfused with a mean of 684 mL retrieved blood. Thirty-four percent did not require further allogenic transfusion within 24 hours. Twenty-seven percent required 2 units. All control patients required 3 units of allogenic blood. Allogenic transfusion in CATS patients decreased significantly (p < .0001). Three CATS patients developed renal impairment compared with nine controls (p = .037). Mean ICU stay was significantly reduced in CATS patients (p = .042). Mean postoperative hospital stay for the CATS group was 18 days compared with 25 days in the control group (p = .014). Thirty-day mortality was 12% in CATS patients compared with 19% in the control group (p = .199). There was a mean saving of €5,236.5 per patient using CATS.
CATS markedly reduced the amount of blood transfused. CATS was associated with reduced ICU and postoperative hospital stay. CATS proved to be cost-effective.
9.38–9.45: Discussion
SESSION VIII: Thoracic Aortic Disease: Aneurysm, Dissection, and Coarctation: From Hybrid Techniques to Best Medical Management
Moderators: Frank J. Veith, MD, Sherif Sultan, MCh, MD, FRCS, EBQS-Vasc
Jacob Buth, Peter L Harris, Roel Hobo, Randolph van Eps, Philippe Cuypers, Lucien Duijm, Xander Tielbeek
Six hundred six patients were prospectively enrolled into the EUROSTAR database. Thoracic pathologies, with either urgent or elective presentation, included degenerative aneurysm (n = 291), aortic dissection (n = 215), traumatic rupture (n = 67), anastomotic false aneurysm (n = 24), and infectious or not specified disorders (n = 9). Study end points included evidence of perioperative spinal cord ischemia (SCI) or stroke. Univariate analysis and multivariate regression models were used to assess the significance of clinical factors that potentially influenced the occurrence of. Fifteen patients (2.5%) developed paraplegia or paraparesis and 19 (3.1%) stroke. Two of these patients had both complications combined. At multivariate regression analysis, independent correlation with SCI was observed for four factors: (1) left subclavian artery covering without revascularization (p = .027, odds ratio [OR] 3.9), (2) renal failure (p = .02, OR 3.6), (3) concomitant open abdominal aorta surgery (p = .037, OR 5.5), and (4) number of stent grafts used 3 (p = .043, OR 3.5). In patients with perioperative stroke, two correlating factors were identified: (1) duration of the intervention (p = .0045, OR 6.4) and (2) female gender (p = .023, OR 3.3). Of the patients in whom left subclavian covering was required, 8.4% developed a neurologic complication (paraplegia or stroke) as opposed to 0% with prophylactic revascularization (p = .049).
Perioperative paraplegia or paraparesis was significantly associated with blockage of the left subclavian artery without revascularization. The clinical significance of this source of collateral perfusion of the spinal cord had not been confirmed previously. Intracranial stroke was associated with lengthy manipulation of wires, catheters, and introducer sheaths within the aortic arch, reflected by a longer duration of the procedure.
Alan B. Lumsden, Eric K. Peden, Jon-Cecil Walkes, Michael J. Reardon
Department of Cardiovascular Surgery, Methodist DeBakey Heart and Vascular Center, The Methodist Hospital, Houston, Texas, USA
Endovascular treatment of thoracic aortic aneurysmal disease has the potential to reduce perioperative morbidity and mortality compared with traditional open surgery in high-risk patients. To properly exclude the aneurysm segment, current endograft devices require landing attachment zones that are free of major branch vessels. Endovascular repair of aneurysms involving the aortic arch usually entails an adjunctive procedure to remove or debranch the arch vessels from the proximal landing zone. The debranched vessels are transposed or bypassed to maintain blood flow to the critical upper body structures. Preoperative computed tomography is used to size the landing zone. Present technology requires an aortic diameter < 38 mm and 2 cm of length for the landing zone. Our technique of thoracic aortic debranching to create an appropriate landing zone in the arch can be categorized based on the location of the arch vessels. For landing zones involving the origin of the left subclavian artery, we selectively perform carotid-subclavian bypass. Coverage of the origin of the left common carotid artery often adds only minimal length to the landing zone, but, when appropriate, a carotid-carotid bypass is performed in addition to a carotid-subclavian bypass. When aortic pathology extends to the innominate artery, we prefer a one-stage aortoinnominate bypass with the endograft deployed antegrade through a side branch off the graft. We describe our rationale and surgical technique for arch debranching, including the avoidance of pitfalls and complications. Until the technology for fenestrated endografting becomes better developed, aortic arch debranching for endograft placement is a feasible option for high-risk patients with aneurysmal disease.
Dieter Raithel, Lefeng Qu
Nuremberg South Hospital, Nuremberg, Germany; Changhai Hospital, The Second Military Medical University, Shanghai, China
Mark D. Morasch
Northwestern University Feinberg School of Medicine, Chicago, Illinois, USA
Rodney A. White
Mark K. Eskandari
Division of Vascular Surgery, Northwestern University, Feinberg School of Medicine, Chicago, Illinois, USA
10.27–10.37: Discussion
10.37–10.50 COFFEE BREAK
SESSION IX: Carotid Disease II: When to Operate and the Influence of Plaque Morphology and Statin Therapy
Moderators: Nicholas J. Cheshire, MD, Georgio M. Biasi, MD
Giorgio M. Biasi, MD
Luis Mendes Pedro, MD
Faculdade de Medicina de Lisboa, Lisboa, Portugal; Instituto Cardiovascular de Lisboa, Lisboa, Portugal
Carotid stenosis can be associated with neurologic events, more commonly in recently symptomatic lesions. The risk associated with > 80% asymptomatic plaques is around 2 to 3% per year, and intervention in these patients is only justified if the operative risk is low and the patient's life expectancy is long.
Other factors, beyond the degree of stenosis, are important in the clinical outcome of carotid plaques. Several publications show that the subgroup of asymptomatic plaques that will become symptomatic in the follow-up exhibits morphologic aspects of surface disruption or vulnerability to rupture. These features may be identified using computer-assisted ultrasonography or advanced magnetic resonance techniques.
Previous randomized trials designed to assess the role of surgery in asymptomatic stenosis included best medical treatment, with antiplatelet drugs and global risk factor control. In recent years, statins emerged as a powerful tool for cholesterol reduction, and they have clearly been shown to be beneficial in the primary and secondary prevention of coronary and cerebrovascular events.
Statins are able to induce some regression of atherosclerotic plaques. Nevertheless, the clinical benefit was shown to be much higher than the little amount of stenosis reduction visible on arteriography and the benefit that could be attributable to cholesterol reduction. Other effects, called pleiotropic, were demonstrated and found to influence directly the structure and biologic behavior of the lesions. Those pleiotropic properties of statins seem to promote plaque stabilization by reduction of the inflammatory and proteolytic activity inside its structure.
A large and consistent burden of evidence established that statins reduce the overall risk of coronary and cerebral events and reduce significantly the mortality of atherosclerotic patients, being indicated routinely in secondary prevention.
The role of cholesterol-lowering drugs in patients with carotid stenosis was studied in smaller studies. They suggest a decrease in neurologic morbidity associated with carotid plaques and a reduction in the risk of stroke and death in the peroperative period of carotid endarterectomy. This benefit seems to be higher in symptomatic patients, who usually have more vulnerable and active plaques–-what seems to confirm the capacity of changing plaque behavior in favor of stabilization that was attributed to statins. These mechanisms were also confirmed by biochemical studies, performed in plaques removed by endarterectomy in patients taking statins and compared with patients without that medication, which showed that in the first group, the specimens had a lesser amount of matrix metalloproteinases and interleukin-6. The direct modulation of the arterial wall by statins was also demonstrated by the control of progression or even regression of intima-media thickness and plaque burden and by the increase in plaque echogenicity, suggesting a lesser amount of calcium and collagen and thus a more stable and less vulnerable lesion.
In conclusion, statins are associated with clear benefit in terms of reduction of the global cardiovascular risk in atherosclerotic patients and should be a part of the best medical treatment for carotid stenosis at the present time.
In the absence of large randomized trials specifically designed to answer the role of statins in carotid stenosis, there is some evidence that they contribute to plaque stabilization and are associated with less per-operative risk and lower risk of symptoms. We should expect that intensive medical treatment including statins can decrease the risk of asymptomatic plaques, and the need for intervention, but, at the moment, this is an unproved issue.
Tim Counihan, MD, Mudassir Iqbal, MRCPI Galway University Hospital and National University of Ireland, Galway, Ireland
J. J. Gregory Modrall, MD, Patty I. Boyd, RVT, G. Patrick Clagett, MD
University of Texas Southwestern Medical Center and Dallas V.A. Medical Center, Dallas, Texas, USA
Nicholas J. Cheshire
Dimitri P. Mikhailidis, MD, FFPM, FRCP, FRCPath Department of Clinical Biochemistry (Vascular Disease Prevention Clinics), Royal Free Campus, University College London, London, United Kingdom
Several statin-based trials (eg, 4S, CARE, LIPID, GREACE, HPS, TNT) involving patients with coronary heart disease (CHD) showed that these drugs significantly reduce the number of strokes. In TNT, treating CHD patients with atorvastatin 80 mg/d was more effective than using atorvastatin 10 mg/d. SPARCL confirmed that aggressive lipid lowering with atorvastatin was effective in preventing both cerebrovascular and cardiac events. A key feature of SPARCL is that the patients had previous cerebrovascular events but no overt CHD. Two trials (ALLHAT and PROSPER; both using pravastatin 40 mg vs placebo) did not show a significant reduction in stroke risk, possibly because cholesterol reduction was modest.
There is evidence that raising HDL levels may reduce the incidence of stroke. Thus, in VA-HIT, a fibrate (gemfibrozil) reduced the risk of stroke/transient ischemic attacks (TIA). There is also evidence showing that aggressive lipid-lowering therapy will reduce the need for carotid interventions in high-risk patients and improve surgical outcome.
There is little evidence that lipid-lowering drugs reduce the risk of stroke in a primary prevention setting (WOSCOPS, AFCAPS/TexCAPS), although the trend is favorable. The CARDS trial showed a significant reduction in stroke in type 2 diabetics without clinically evident CHD but with additional risk factors.
The mechanism responsible for reducing the risk of stroke after using statins may involve the regression of atherosclerosis and plaque stabilization in the carotid artery and aortic arch.
More attention needs to be paid to using statins to prevent strokes and TIAs.
Carlos H. Timaran, Eric B. Rosero, MD, J. Gregory Modrall, MD, James Valentine, MD, Patrick Clagett, MD
University of Texas Southwestern Medical Center, Plano, Texas, USA
Niamh Hynes, Sherif Sultan
Western Vascular Institute, Department of Vascular and Endovascular Surgery, University College Hospital, Galway, Ireland; Department of Vascular and Endovascular Surgery, Galway Clinic, Doughiska, Galway, Ireland
Routine patching after carotid endarterectomy (CEA) is preferable to primary closure because of a threefold reduction in perioperative thrombosis, early and late stroke, and late restenosis. Polytetrafluoroethylene (PTFE) patching of CEA has comparable results to autogenous vein in early postoperative outcome. However, it requires a prolonged hemostasis time. Collagen-impregnated Dacron is believed to avoid the needle-hole injuries seen with PTFE. The differences between thin (HemaCarotid knitted) and ultrathin (HemaCarotid ultrathin) Dacron patches have not been previously studied. The objective of this study was to compare clinical and technical outcomes of two types of patch, regarding their progenicity, thickness, performance, and restenosis rate.
Sixty-five CEA were randomized to either thin (27 patients) or ultrathin (38 patients) patch closures. Patients and surgeon were blinded to patch type. All patients underwent clinical assessment and duplex ultrasound scanning at 6 weeks and 6, 12, and 18 months postoperatively. Demographic and clinical characteristics were similar in both groups. The mean follow-up was 38.4 ± 7.7 months.
Early complications included 3 (8%) cases of laryngeal edema in the ultrathin group requiring reintubation and one (4%) in the thin group. There was no ipsilateral stroke, thrombosis, TIA, or death in either group. The 3-year cumulative patency rates for the thin patch were 91.3% (± 5.6%) compared with 94.7% (± 6.3%) with the ultrathin patch (p = .91, hazards ratio [h] = 1.13, 95% CI = 0.16–8.00).
Ultrathin patches were associated with early postoperative laryngeal edema but did not compromise the surgical outcome. Although 3-year patency rates were higher with ultrathin patches, there was no significant difference in the risk of restenosis between patches. HemaCarotid ultrathin Dacron patches provide superior handling, compliance, and conformability to the native vessel compared with thin (HemaCarotid knitted) patches.
Despite the lack of statistical significance between the HemaCarotid ultrathin and the HemaCarotid thin patch, we believe that with correct adjuvant pharmacotherapy and close attention to anticoagulation, the long-term benefit of the ultrathin HemaCarotid patch in reducing restneosis will be established.
11.44–11.54 Discussion
SESSION X: Abdominal Aorta: Pushing the Boundaries: Hybrid Techniques and High-Risk Patients
Moderators: Jacob Buth, MD, Mark Eskandari, MD
John F. Eidt, Ahsan T. Ali, Nathan Mcleod, Venkat R. Kalapatapu, Mohammed M. Moursi
University of Arkansas for Medical Sciences, Little Rock, Arkansas, USA
Sherif Sultan, Niamh Hynes
Department of Vascular and Endovascular Surgery, Western Vascular Institute, University College Hospital, Galway, Ireland; Department of Vascular and Endovascular Surgery, Galway Clinic, Doughiska, Galway, Ireland
John P. Fletcher
University of Sydney and Westmead Hospital, Sydney, New South Wales, Australia
Endovascular aneurysm repair (EVAR) was first performed at Westmead in 1994 with the EndoVascular Technology (EVT) Ancure device. The advantage of this endograft was its unibody design with secure hook attachment system, but it was considered more complex to use than other systems and required a large delivery sheath (27FG).
We had 59 successful Ancure implants up until 2000 when the device became unavailable, and this cohort of patients has been carefully followed for a mean of 78 months. Early intervention for graft limb occlusion was needed in 15.3%, and abdominal conversion was required in 5.1% (one within 1 month, one at 3 years, and one at 9 years). There have been 25 late deaths (42.4%), none from AAA rupture. Endoleak rate was 15.3%, with six patients requiring intervention (two open and four endovascular). Initial aneurysm diameter was significantly greater in patients with endoleak (p = .03); an initial reduction in sac diameter occurred in both endoleak and nonen-doleak patients, but this reduction was not maintained in endoleak. Color Doppler was an effective means of follow-up. Overall, the Ancure device has been durable, with no subsequent interventions needed in 85% of patients after the first 3 months following implantation, but late events out to 9 years emphasize the need for indefinite follow-up.
Since 2000, the Cook Zenith device has been our stent graft of choice. With 75% of abdominal aortic aneurysms now managed by EVAR, the decreasing proportion of open vascular surgery has major implications for vascular surgical training.
Frank J. Veith, MD
The Cleveland Clinic and New York University Medical Center, Cleveland, Ohio, and New York, New York
Despite all therapeutic improvements, open surgical treatment of ruptured abdominal aortoiliac aneurysms (RAAAs) has a high mortality.
Our experience and that of several other centers throughout the world have shown that endovascular techniques, including the use of aortic endografts, have reduced the 30-day mortality of treatment for RAAAs to 10 to 18%. Strategies, adjuncts, and techniques that have contributed to this reduced mortality include the following: (1) hypotensive hemostasis or restriction of fluid resuscitation, allowing the systolic blood pressure (BP) to fall to levels as low as 50 mm Hg without giving fluids; (2) placement, preferably via a femoral approach under local anesthesia, of a guidewire and catheter in the supraceliac aorta; (3) using this catheter, arteriography is performed to define infrarenal aortic neck and iliac anatomy and to determine suitability for endovascular graft repair of the aneurysms using either an aortounilateral graft or a bifurcated modular graft; (4) in the event that circulatory arrest or collapse (BP < 40 mm Hg) occurs, a large (14–16F) hemostatic sheath is placed via one femoral artery into the supraceliac aorta; (5) a large compliant balloon is inserted through this sheath and inflated with dilute contrast under fluoroscopic control to occlude the supraceliac aorta, and the balloon position is supported by leaving the hemostatic sheath in place; (6) the position of the renal arteries is determined, and an aortic endograft is then deployed via the opposite femoral artery while the inflated supraceliac balloon is left in place; (7) if an aortounilateral graft is used, the balloon is then deflated and removed through its insertion sheath; (8) if a modular bifurcated graft is used, the main body is fully deployed, and a second compliant balloon is placed within the body of the graft and inflated; (9) the supraceliac balloon is deflated and removed through the large sheath, which is then removed; (10) the remainder of the operation is completed; this includes common iliac occlusion and a femorofemoral bypass if an aortounilateral graft is used; (11) if abdominal compartment syndrome is suspected because of the need for increased ventilatory pressures or elevated bladder pressure, a minilaparotomy is performed with evacuation of the retroperitoneal hematoma; (12) the abdomen may have to be left open and sealed with a VAC dressing.
Use of these methods and techniques will contribute to improved survival with endograft treatment of RAAAs, and every surgeon should be able to use them.
Rodney A. White
Sherif Sultan, Niamh Hynes
Our endeavor was to contrast clinical and technical outcome of BIF vs AUI in high risk EVAR patients.
From 2002 to 2007, 82 high-risk patients underwent elective EVAR (BIF, n = 52 [63.4%]; AUI, n = 30 [36.6%]). Mean Age 74 years (BIF vs AUI, p = .835), male % (BIF vs AUI, 86.5% vs 76.7%, p = .260) and mean aneurysm diameter (BIF vs AUI: 5.4 cm vs 5.3 cm, p = .514).
The predicted probability of receiving AUI was tabulated for all patients by using multiple logistic regressions to control for SVS comorbidity and anatomical severity scores. We used propensity scoring to adjust for baseline characteristics and selection bias by matching co-variables, creating a pseudo-randomized control design. Primary endpoints were 30-day mortality, 4-year survival and 4-year intervention free survival.
Mean proximal endograft diameter was significantly lower with BIF (29.3 vs 30.9, p = .031). Mean number of devices used was similar (3.0 vs 3.4, p = .165)
BIF and AUI had similar 30-day mortality (1.9% vs 0%, p = .453), 4-year all-cause survival (72.1% vs 74.0%, p = .882, h = 0.92 [95% CI = 0.30–2.78]) and 4-yr aneurysm-related survival (98.1% vs 100%, p = .448). There was no graft migration or structural failure. There was no intervention required for Type II (23.1% vs 36.7%, p = .191). The 4-yr limb thrombosis rate (7.6% vs 10%, p = .723) and 4-yr intervention-free survival (BIF 89.8% vs AUI 85.9%, p = .612, h = 0.71 [95% CI = 0.18–2.76]) were similar. The 4-year Fem-Fem cross over patency rate is 92.6% (95% CI = 75.6%-98.6%).
There were no significant differences in procedure time, mean blood units and change in estimated glomerular filtration rate between groups (p > .05). Length of stay/HDU (4.2 vs 7.4, p = .021/0.87 vs 1.2 days, p = .656) were similarly low, with the majority of patients discharged directly home (BIF vs AUI: 92% vs 80%, p = .103)
By using propensity scoring for the primary end-points, the proportions of AUI patients were equal to BIF for all levels of probability and were unchanged as the probability of AUI increased.
We established at 4 years that clinical and technical outcomes were not compromised with AUI compared with BIF in this high-risk cohort.
Ian Davidson
Department of Interventional Radiology, University College Hospital, Galway, Ireland
The current generation of endovascular stent grafts are more durable than earlier devices. The endovascular space and in particular the thoracic and abdominal aorta remain a relative hostile environment even for industry-manufactured, FDA-approved, CE-marked devices.
Delayed complications associated with earlier stent grafts are now well recognized. Fortunately, only a small proportion of patients treated with today's devices will develop device-related complications. For this unfortunate group of patients, the consequences may be catastrophic.
In life, complacency has a habit of following both confidence and competence. It would be BAD practice to abandon the routine surveillance of aortic stent grafts as some have advocated.
The question is not “if devices will fail” but “when will they fail” and what impact that will have on patient outcome. Thankfully, most “graft failures” never materialize as the overwhelming majority of patients fail to outlive their stent grafts, dying of non-
EVAR-related conditions. The challenge of postprocedural surveillance is to predict those patients in whom complications are more likely to occur, to detect complications early, to intervene only when appropriate, and to avoid the
DEBATE
Franklin S. Yau, Eric B. Rosero, G. Patrick Clagett, R. James Valentine, J. Gregory Modrall, Frank R. Arko, Carlos H. Timaran
University of Texas Southwestern Medical Center, Dallas, Texas, USA
Piergiorgio Cao, MD, FRCS, CAESAR Trial Collaborators
Division of Vascular and Endovascular Surgery, University of Perugia, Ospedale S. Maria della Misericordia, Perugia, Italy
Recent recommendations to screen for abdominal aortic aneurysm (AAA) in high-risk populations and the rapidly growing use of endovascular repair (EVAR) have led to increased interest in evaluating the effectiveness of treatment options for patients with small AAA (diameter 4.0–5.4 cm).
In the pre-endovascular era, two randomized trials (UK-SAT and ADAM) provided an initial valuable foundation for recommended management of small AAAs.
Both trials demonstrated that observation could be safely employed in compliant patients with 4.0 to 5.4 cm diameter AAAs with a low associated annual risk of rupture (0.6–1%) compared with immediate elective open repair.
However, these studies showed that surveillance is often followed by AAA repair; in fact, only 7% of patients surviving 8 years after inclusion in the UK SAT had no intervention.
Still, the optimal strategy to treat patients with small AAA is yet debated.
Patients lost to follow-up were associated with a 10% risk of AAA rupture and a lower overall survival rate compared with compliant patients.
This amount of uncertainty has been fuelled by the introduction of endografting with the prospective to offer less perioperative risks but undefined durability in the long term.
EVAR has been rapidly replacing open aneurysm repair for the treatment of infrarenal AAAs. Recent insights from two randomized studies comparing EVAR and open repair (EVAR 1 trial and DREAM) showed reduced operative mortality and aneurysm-related death.
Nevertheless, RCTs on EVAR analyzed exclusively populations with large AAA.
EVAR of large AAAs is vulnerable to imperfect outcomes because such aneurysms are more likely to be associated with hostile aneurysm anatomy.
The proportion of potential candidates anatomically suitable for enrolment into the EVAR 1 trial was 54%; an additional point of concern about surveillance is that patients with a growing AAA can become unsuitable candidates for EVAR.
EVAR could be representing the treatment of choice for small AAAs.
The CAESAR study (Comparison of Surveillance vs Aortic Endografting for Small Aneurysm Repair study) is a randomized multicenter clinical trial designed to compare endovascular repair versus surveillance and eventually delayed treatment in patients with small AAAs (measuring between 4.1 and 5.4 cm in maximum diameter defined by CT scan) suitable for EVAR. Patients between 50 and 80 years of age, with small AAA anatomically suitable for EVAR, are randomly allocated to early EVAR or surveillance.
The CAESAR trial started in Europe in 2004. The sample size was estimated to be 740 patients. The primary study end point is mortality from any cause. Secondary end points include aneurysm-related death, AAA rupture, perioperative or late complications, conversion to open repair, and complications associated with delayed treatment including loss of treatment options, growth of the aneurysm, and reduced quality of life. The CAESAR trial has currently enrolled 333 patients at 19 centers with demonstrated experience.
A similar study in the United States, the PIVOTAL trial (Positive Impact of endovascular Options for Treating Aneurysms earLy), is planned to compare surveillance to EVAR for AAA of 4 to 5 cm, including 1,700 patients at 70 clinical centers. The primary end point is AAA-related mortality, and secondary end points are survival and freedom from rupture.
In the meantime, until the results of the ongoing trials will be available, patients with small AAAs should be included in a strict surveillance protocol or enrolled in randomized trials.
12.57–13.07: Voting and Panel Discussion
Anthony J. Comerota, MD, FACS, FACC Jobst Vascular Center, Toledo, Ohio, USA

_
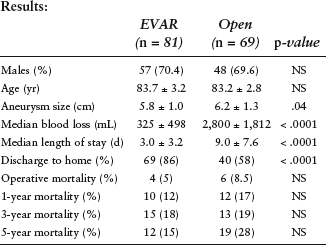
A total of 27 of 81 (33%) patients in the EVAR group died compared with 34 of 69 (49%) patients in the OR group. The median survival time for EVAR was 350 weeks (145–404) compared with 317 weeks (233–342) for the OR group. A Kaplan-Meier log-rank analysis showed no difference in early or long-term survival between EVAR and OR (p = .13).
Niamh Hynes, Sherif Sultan Western Vascular Institute, Department of Vascular and Endovascular Surgery, University College Hospital, Galway, Ireland; Department of Vascular and Endovascular Surgery, Galway Clinic, Doughiska, Galway, Ireland
Operative survival is as high as 96% for elective abdominal aortic aneursym (AAA) repair but as low as 10% for emergency repair. Our primary aim was to compare elective AAA repair in octogenarians with nonoperative management. Our secondary aim was to compare octogenarians with their younger counterparts.
From 1998 to 2003, 180 patients with AAA were treated operatively or nonoperatively. Factors determining treatment included American Society of Anesthesiologists grade 4, inoperable malignancy, New York Heart Association class III, forced expiratory volume in 1 second < 35%, creatinine > 6.0 mg/dL, and patient and family choice. A parallel-group observational study was performed to assess age and treatment effects on outcome.
Seventy (39%) patients were repaired electively, 68 (38%) were managed nonoperatively, and 42 (23%) underwent emergency repair. Fifty-nine (33%) were octogenarians.
The octogenarian 5-year survival rate was 20% following emergency repair, 42% if treated nonoperatively, and 83% following elective repair. Younger cohort rates were 55% (emergency), 44% (nonoperative), and 76% (elective).
The octogenarian mean expansion rate was 0.26 cm/yr in those treated nonoperatively and 1.04 cm/yr in confirmed rupture. Rupture rate was related to expansion rate (95% confidence interval [CI] 0.06–0.59, r = .35, p = .01). The rates in the younger subgroup were 0.32 cm/yr and 1.14 cm/yr (95% CI -0.021–0.672, r = .37, p = .03).
The octogenarian survival rate was highest following elective repair. Rupture was closely correlated with aneurysm expansion. Screening should reduce the incidence of octogenarian rupture of AAA and identify those patients most suitable for nonoperative management.
Chris Beirne, Sherif Sultan
Western Vascular Institute, Department of Vascular and Endovascular Surgery, University College Hospital Galway, Galway, Ireland
13.24–13.34: Discussion
13.34–14.30: LUNCH
SESSION XI: Peripheral Vascular Disease II: Medical Optimization and Adjuvant Techniques
Moderators: Peter R.F. Bell, MD, FRCS, DSC, KBE, Dimitri P. Mikhalidis, MSc, MD, FACB, FFPM, FRCP, FRCPath
Anthony J. Comerota, MD, FACS, FACC
Jobst Vascular Center, The Toledo Hospital, Toledo, Ohio, USA
Patients with peripheral arterial disease (PAD) have significant cardiovascular morbidity and mortality, which is “dose related” to the severity of their lower extremity occlusive disease. 1 In fact, cardiovascular mortality of PAD patients exceeds that of patients presenting with coronary artery disease and those presenting with stroke. 2
Platelet inhibition is the foundation of pharmacotherapy for all patients with vascular disease. The Antiplatelet Trialists’ Collaborative demonstrated that platelet inhibition resulted in a 27% risk reduction of stroke, amputation, myocardial infarction, and vascular death following their meta-analysis of 142 randomized trials evaluating over 73,000 patients. 3 Their updated publication reporting on over 100,000 patients revealed that lower doses of aspirin (75–150 mg) were more effective than higher doses. 4
The results of large clinical trials in patients with PAD will be reviewed. Conclusions from this review are as follows:
All patients with PAD should be treated with platelet inhibition. If ASA is used, lower doses (75–150 mg/d) are more effective than higher doses. Clopidogrel (75 mg/d) is more effective than ASA in reducing ischemic events and vascular death in PAD patients. Pretreatment with combined platelet inhibition (ASA plus clopidogrel) in patients undergoing percutaneous angioplasty and stenting appears reasonable, based on PCI studies. Combined platelet inhibition is more effective than ASA alone in patients with prosthetic lower extremity bypass grafts. Combined platelet inhibition is not recommended for primary prevention. Combined platelet inhibition is associated with significantly higher bleeding risk.
D.P. Mikhailidis, MD, FFPM, FRCP, FRCPath Department of Clinical Biochemistry (Vascular Disease Prevention Clinics), Royal Free Hospital, University College London, London, United Kingdom
Peripheral arterial disease (PAD) is considered a coronary heart disease (CHD) equivalent by several guidelines. This is because these conditions are associated with a very high vascular morbidity and mortality. Despite this evidence, these patients are often undertreated.
Improving the lipid profile (eg, with statins) is associated with a reduction in vascular events in patients with PAD (Heart Protection Study; simvastatin 40 mg vs placebo) and improved walking distance. There is also some evidence from retrospective surveys showing that statins improve perioperative morbidity and mortality as well as the results of vascular interventions.
It is important to consider that a very high proportion of patients with PAD have CHD. The evidence that statins are of benefit in patients with CHD is overwhelming. PAD is also an important predictor of stroke. It is therefore of interest that it is now widely accepted that statins play a significant role in stroke prevention. Impaired renal function is a common feature in patients with PAD. There is emerging evidence showing that statins exert a “nephroprotective” action.
In terms of prevention, there is evidence in The Program on the Surgical Control of the Hyperlipidemias (POSCH) trial that lowering cholesterol levels decreases the risk of developing PAD.
The evidence is there; the issue now is implementing treatment. This presents several difficulties, which include education, expertise, and cost.
J. Gregory Modrall, MD, Jennie Hocking, PA-C, G. Patrick Clagett, MD
University of Texas Southwestern Medical Center, Dallas, Texas, USA
Chris Beirne, Sherif Sultan
Western Vascular Institute, Department of Vascular and Endovascular Surgery, University College Hospital, Galway, Ireland; The Galway Clinic, Doughiska, Galway, Ireland
Wael Tawfick, Olubumni Esan, Anne Fahy, Sherif Sultan
Western Vascular Institute, Department of Vascular and Endovascular Surgery, University College Hospital, Galway, Ireland; The Galway Clinic, Doughiska, Galway, Ireland
Critical limb ischemia (CLI) patients are at high risk of primary amputation. Using a sequential compression biomechanical device (SCBD) represents a nonoperative option in threatened limbs.
We aim to determine the outcome of using SCBD in amputation-bound nonreconstructable CLI patients regarding limb salvage and 90-day mortality.
Thirty-five patients with 39 critically ischemic limbs (rest pain = 12, tissue loss = 27) presented over 24 months. Thirty had nonreconstructable arterial outflow vessels and 5 were inoperable due to severe comorbidity scores. All were Rutherford classification IV/V with multiple level disease. All underwent a 12-week treatment protocol and received best medical treatment. The mean follow-up was 10 months (SD ± 6 months). There were four amputations, with an 18-month cumulative limb salvage rate of 88% (SE ± 7.62%). Ninety-day mortality was zero. Mean toe pressures increased from 38.2 to 67 mm Hg (SD ± 33.7; 95% CI 55–79). Popliteal artery flow velocity increased from 45 to 47.9 cm/s (95% CI 35.9–59.7). Cumulative survival at 12 months was 81.2% (SE ± 11.1) for SCBD compared with 69.2% in the control group (SE ± 12.8%) (p = .4, hazards ratio = 0.58, 95% CI 0.15–2.32). The mean total cost of primary amputation per patient is €29,815 in comparison with €13,900 for SCBD patients.
SCBD enhances limb salvage and reduces length of hospital stay, nonoperatively, in patients with nonreconstructable vessels.
15.01–15–11: Discussion
SESSION XII: The Diabetic Foot and Wound Management: Are We Prepared for the Diabetes Epidemic?
Moderators: Sean Dinneen, FRCPI, FACP, Cliff P. Shearman, MS, FRCS
Cliff P. Shearman
University of Southampton, Southampton,
United Kingdom
Over 40% of patients presenting with peripheral arterial disease have diabetes, and this pattern seems to be continuing to increase. Patients with diabetes and PAD have a worse prognosis, and the majority of lower limb amputations in the United Kingdom are performed for diabetic vascular disease. Some countries, notably Finland, have been successful in reducing amputation rates in patients with diabetes. In this presentation, I will demonstrate how we changed our approach to this common problem and the effect it had on amputation rates and on our service.
A prospective database was set up for all patients with diabetic foot complications presenting to secondary care. A process mapping exercise was undertaken to identify areas of poor practice. Following this, a diabetic foot team (DFPT) was formed working across primary and secondary care.
Between 2003 and 2007, the hospitalization rate was, on average, 11.4 admissions per month, with 59 admissions in 6 months before the team began, 118 in the first year (average LOS 21 days), 126 in the second year (average LOS 20 days), and 174 in the third year (average LOS 15 days). In those hospitalized, the median length of stay reduced from 47 to 18.7 days, and there was a noticeable shift in elective compared with nonelective admissions. This represented a cost saving over 3 years of £1.3 million. This is balanced with an overall increase of 7% more patients being managed appropriately in primary care year on year. The number of revascularization procedures has increased year on year. This is linked to an increase of 45% more minor amputations, but this was matched by a 60% reduction in major amputations. By checking the HRG coding of the procedures, we also identified during these time coding inaccuracies that lost the service a potential £750,000.
We have demonstrated that a DFPT will reduce major amputation rates and hospitalization in patients with diabetes. It is highly cost-effective, reducing length of stay by 50%, and patients value it. A national approach to the problem of diabetic vascular disease could make a major impact on amputation rates in the United Kingdom.
Sean F. Dinneen, Laura Kelly, Lorna Hurley, Catherine Dolan, Sarah Kelly
Department of Medicine, NUI Galway and Diabetes Centre, University Hospital Galway, Galway, Ireland
Diabetic foot complications are a frequent cause of hospitalization. With appropriate screening, many of these complications are preventable. To make the case for investment in preventive services, we (a) profiled the cost of care for three patients with complex diabetic foot problems and (b) assessed the prevalence of unrecognized early foot complications in an urban general practice.
_
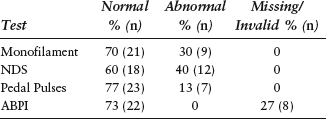
Stella Vig, BSc, MB BCh, FRCS Department of Vascular Surgery, St. George's Hospital, London, United Kingdom
Arjan J. van den Hil
Biomet Biologics Inc., Warsaw, Indiana, USA, and Rieslinggaard 21, Woerden, the Netherlands
The wound healing cascade exists of many complex processes. When tissue is damaged, the first processes to occur are bleeding, coagulation, and platelet activation. Platelets contain a variety of growth factors, cytokines, and antimicrobial peptides, which are released on activation of the platelets. These factors play a major role in the wound healing process.
An overview will be given on the role of these growth factors and cytokines, along with a description of a simple technique to make a platelet concentrate at the point of care from a small amount of the patient's own blood.
A protocol on how to use a platelet concentrate for wound healing is presented, along with an overview of several clinical studies and case presentations, showing the beneficial effect of this new technology.
At the end, a brief introduction will be given on the possibility to harvest a stem cell concentrate from the patient's own bone marrow for treatment of, for example, peripheral arterial disease.
Gabrielle Colleran, Helen Heneghan, Clare-Anne McKeon, Sherif Sultan
Western Vascular Institute, Department of Vascular and Endovascular Surgery, University College Hospital Galway, Galway, Ireland
Successful level of amputation is gauged by the attainment of long-term limb salvage. There is an accepted hypothesis that IDA is complicated by gangrene and an indication for further amputation.
Between October 2002 and January 2008, 265 patients underwent lower limb amputation, of whom 114 patients (153 procedures) had ITMA or IDA for CLI. Seventy-six (66.7%) IDA and 38 (33.3%) ITMA were performed. Revascularization procedures were performed in 49% of cases (57/114).
The composite end points were number of repeat operations, time to major amputation, and survival. The mean age was 72.99 in the IDA group and 70.55 in the TMA group. Eighty-seven (76.31%) were male.
There was no statistically significant difference between the two groups in their demographics and comorbidities. Twenty-five patients in the IDA group had at least a second amputation compared with 11 in the ITMA group (p = < .735). Twelve IDA patients progressed to major amputation in comparison with eight ITMA patients (χ = 0.486).
Nine patients died in each group. There was no difference in survival between the two groups.
Patients with CLI who endured IDA have a high frequency of recurrent and persistent ischemia with imperiled limb loss. ITMA propounded brisk wound healing in diabetic patients and offered an alternative to above-knee amputation at the transtibial level with early prosthetic rehabilitation and mobility.
15.44–15.54 Discussion
SESSION XIII: Renal and Visceral Disease: Vascular Management and Organ Protection
Moderators: James C. Stanley, MD, Jerry Goldstone, MD, FACS, FRCSE
Jerry Goldstone, MD, FACS, FRCSE Department of Surgery, Case School of Medicine and Division of Vascular and Endovascular Surgery, University Hospitals Case Medical Center, Cleveland, Ohio, USA
Renal duplex scan (RDS) is the most frequent noninvasive test that we use to identify patients with renal vascular disease and for evaluating intraoperative and postoperative renal artery repair. In spite of the wide availability of CTA and MRA, with the increasing recognition of ischemic nephropathy as a cause of renal failure and the increasing use of renal angioplasty and stenting, we have seen a marked increase in the number of RDS, from 24.7/month in 2000 to 42.5/month in 2006. A detailed analysis of a recent sample of 741 consecutive RDSs revealed that the most frequent indications were hypertension, suspect/known renal artery stenosis (RAS), postprocedure surveillance (PPS), renal failure, and miscellaneous. Studies were classified, using the Strandness criteria, as positive for 60% stenosis, negative, or equivocal. Overall, 18.2% were positive, 75.3% negative, and 6.6% equivocal or technically unsatisfactory. The results by indication for the study were as follows:
_
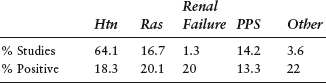
In our laboratory, RDS correlated with contrast angiography in 81% of cases. Internal medicine services ordered 39.8% of the RDS, and 15.9% were positive. The vascular surgery service ordered 35.4% of the studies, and 25.1% were positive; 6.6% of studies were interpreted as equivocal or nondiagnostic. These were most common when performed on inpatients and especially when performed at the bedside. About 1 hour of technician time was required for each scan.
Donal Reddan
Department of Nephrology, Galway University Hospitals, Galway, Ireland
Contrast nephropathy (CIN) is defined as the new onset or exacerbation of renal dysfunction after contrast administration without other identifiable causes. The definition includes an increase in serum creatinine of 25% or an absolute increment of 44.2 μmol/L. The number of diagnostic and interventional procedures that use iodinated contrast media (CM) has increased dramatically in recent years. Unfortunately, despite the availability of newer CM with reduced toxicities and improved safety profiles, some patients remain at risk for serious adverse events. At-risk patients must be identified and properly managed to reduce the risk of contrast-associated complications. Early identification of at-risk patients can ensure that patients are properly prepared and can lead to changes in approaches to their management.
Chronic kidney disease at baseline presents a significant increase in the risk of developing CIN. Although creatinine has been the traditional surrogate for renal function, prediction equations such as the Modification of Diet in Renal Disease (MDRD) formula are much more practical in detecting CKD.
Among low-risk patients, prevention requires ensuring adequate hydration status.
The major strategies for prevention of CIN in high-risk patients include the following:
Avoid nephrotoxic drugs Volume repletion Minimize contrast volume N-acetylcysteine Nonionic, low osmolar contrast media
Once CIN has been established, there are no specific interventions identified that specifically target the process, and management is largely supportive, including renal replacement therapy where necessary.
Ali Amin, MD, RVT, FACS, FACC
Arteriography is a technique where radiopaque contrast material is injected into the vessels. This allows visualization of the arterial tree during diagnostic or therapeutic interventions. Two principal categories of intravascular contrast agents are (1) positive contrast: liquids that have greater attenuation than soft tissue due to the presence of iodine or gadolinium and (2) negative contrast: agents that have lower attenuation than soft tissue, such as carbon dioxide gas. Since the iodinated contrast agents are the most common contrast media used in angiography, nephropathy induced by these agents remains the most clinically important complication during angiography. Radiocontrast nephropathy (RCN) is associated with increased morbidity and mortality. As more vascular surgeons perform their own diagnostic and therapeutic endovascular interventions, it is important to develop techniques that could minimize the development of RCN. Use of other noniodinated contrast agents such as CO2 and gadolinium is technically limited, difficult, and expensive, especially in the hands of vascular surgeons, who might be unfamiliar with and lack the proper equipment to use these products. Patients at increased risk for development of radiocontrast nephropathy include those with diabetes mellitus, preexisting renal insufficiency, dehydration, congestive heart failure, chronic liver disease, and multiple myeloma.
Since nephrotoxicity is most commonly due to the iodinated part of the contrast agent, several protective measures may be used to minimize the toxic effect. A combination of these protective measures, with advance use of wires and catheters, can reduce the risk of renal insufficiency without compromising the detail anatomic road map needed to pursue endovascular intervention or bypass surgery in a high-risk patient. Protective measures to decrease nephrotoxicity include (1) adequate hydration with saline or sodium bicarbonate and (2) dilute contrast agent by 50%. Modifications of the technical procedure help deliver the diluted contrast to the area of intent without compromising the detail needed to pursue endovascular intervention or bypass surgery.
Anil P. Hingorani, MD
College of Medicine, SUNY Brooklyn and Maimonides Medical Center, Brooklyn, New York
Jerry Goldstone, MD, FACS, FRCSE Case School of Medicine and Division of Vascular and Endovascular Surgery, University Hospitals Case Medical Center, Cleveland, Ohio, USA
Several options exist for the surgical management of renal artery stenosis (RAS). The two major categories are direct (aortorenal) and indirect (hepato/splenorenal). We compared the outcomes of 166 elective renal revascularizations in 124 successive patients treated at our institution for atherosclerotic RAS using these techniques. Demographics: mean age 71.8 years; 51% male; 21.8% diabetic; 89.5% hypertensive, and 1.6% on dialysis. Aortic cross-clamping was required in 101 of 124 (81.5%), and concurrent aortic reconstruction was performed in 92 of 124 (74.2%) patients. Indirect bypass was performed in 23 of 124 (18.5%) patients (28 arteries), 82% with an autogenous vein. PTFE conduits were used in 92% of the aortorenal procedures. Overall operative mortality was 5.6%, with all seven deaths in patients over 70 years of age in the aortorenal group. There was only one early graft occlusion, an aortorenal bypass. Follow-up averaged 13.8 months, and 98.4% of grafts that were imaged were patent. Mean SICU and total length of stay, measures of morbidity, were longer for the aortorenal compared with the hepato/splenorenal group in spite of the latter being older and sicker. There was no difference between groups in functional results of the renal revascularizations.
Brian J. Manning, Sherif Sultan
Department of Vascular and Endovascular Surgery, Western Vascular Institute, University College Hospital, Galway, Ireland
Chronic mesenteric ischemia (CMI) is a rare yet important trigger of abdominal pain, difficult to diagnose, and challenging to treat. A neurogenic or vascular etiology has been proposed. We reviewed our experience over a 5-year period.
Seven patients were treated for CMI; four had median arcuate ligament (MAL) decompression and celiac ganglion sympathectomy (CGS). Three had MAL decompression and CGS combined with mesenteric reconstruction.
There was no morbidity or mortality. An early symptomatic response with resolution of symptoms was seen in all patients. At a mean of 20 months of follow-up, duplex ultrasonography (DU) showed high peak systolic velocity (PSV) in five patients that did not correlate with return of symptoms, with 71% of patients remaining symptom free at 2.4 years (mean).
MAL decompression and CGS are associated with demonstrable improvement in mesenteric blood flow and excellent symptomatic improvement. Asymptomatic restenosis on duplex examination is common, suggesting that symptoms are both neurogenic and vascular in origin.
16.34–16.44: Discussion
16.49–17.00: COFFEE BREAK
SESSION XIV: Venous Disease I: Varicose Veins
Moderators: K. Simon Cross, MD, MmedSci, FRCSI(Gen), FRCS(Ed), Anthony J. Comerota, MD, FACS, FACC
Mahj S. Gohel, Alun H. Davies
Department of Vascular Surgery, Charing Cross Hospital, London
Niamh Hynes, Sherif Sultan
Western Vascular Institute, Department of Vascular and Endovascular Surgery, University College Hospital, Galway, Ireland
There is a paucity of data on the EVLT incidence of postoperative pain, phlegmon, and recanalization. Our aim is to compare saphenous closure rates, complications, and cost-effectiveness of HE-EVLA and stab avulsion with level II saphenofemoral junction ligation and stab avulsion with upward perforate invaginate stripping (EUPIS) or conventional downward invaginate stripping (DIS).
From 2003 to 2007, of 756 consecutive VVS procedures, we matched controlled 257 patients with primary VVs, CEAP 2, 3, and 4. Sixty-four had HE-EVLA under local anesthesia (88% female; mean age [± SD] = 50 ± 11 years), 130 had EUPIS under spinal anesthesia (75% female; mean age [± SD] = 52 ± 13 years), and 63 had DIS (60% female; mean age [± SD] = 50 ± 15 years). HE-EVLA was performed with 14 W at 100 J/s. Major adverse events (MAE), quality time spent without symptoms or toxicity (Q-TWiST), and cost-effectiveness were analyzed. Venous clinical severity (VCSS), segmental disease (VSDS), and disability (VDS) scores were compared, but all were statistically similar (p > .05).
The mean follow-up was 29 ± 8.7 months, and the LSV closure rate with HE-EVLA was 96.2% (95% CI 87.2–99.2%) at 36 months. At 3 years, there was no incidence of recurrence with EUPIS or DIS. The mean length of stay was lower with HE-EVLA (5 hours vs 15 hours [ES] vs 18 hours [CS], p < .0001).
There was one incidence of wound infection with DIS (1.6%, p = .217). There were eight cases of severe postoperative pain in the HE-EVLT group (12.5%), two in the DIS group (3.2%), and none in the EUPIS group (p = .000154). There were two cases of phlegmonous phlebitis with HE-EVLA (3%, p = .047). All cases resolved with oral antibiotics and analgesia. Using Cox proportional hazard ratios, the only factors found to influence the rate of MAE were use of laser (p = .005), antiplatelets (p = .012), and length of LSV (p = .025). The use of endovenous conduits reduced the risk of MAE (HE-EVLA and EUPIS vs DIS, p < .001).
Three-year Q-TWiST was longest with DIS (35 months) compared with HE-EVLA (23 months, p < .1) or DIS (26 months, p < .01). But there was a 30% reduction in mean cost per QALY with HE-EVLA compared with EUPIS or DIS.
The use of endovenous stripping reduces the incidence of hematoma and pain along the track of the LSV. HE-EVLT is a safe, prudent, effectual procedure; however, postoperative thermal injury pain is the foremost constraining dynamic factor with contemporary laser probes.
Simon Cross, M. Corrigan, T.Y. Khan
Department of Vascular Surgery, Waterford Regional Hospital, Ireland
Brendan O'Cochlain
The Galway Clinic, Galway, Ireland
Patent foramen ovales (PFO) are seen in up to 25% of the adult population. Cryptogenic strokes account for 20 to 40% of all ischemic strokes. The source of emboli is thought to be either venous clot or fibrin debris that crosses to the systemic circulation through the PFO. Observational studies show an increased prevalence of a PFO in patients experiencing this type of stroke. Sclerotherapy for varicose veins involves the injection of a sclerosing agent into the veins of the lower extremity. There is a theoretical risk of the sclerosing agent crossing from the venous circulation to the systemic circulation through a PFO. This could potentially cause a stroke. This subject requires further evaluation.
Michel Perrin Lyon, France
It is difficult to assess the results of perforator surgery since analysis of various series reported shows that the procedure was almost always associated with other surgical procedures.
Deep venous reconstructive surgery at 1 to 99 months (mean 23) the healing cumulative rates after ballooning and stenting of iliocaval obstruction were available for 158 C6 patients. There was no significant difference in terms of results between primary (62%) and secondary (55%) etiology.
Surgical treatment of deep vein reflux is credited with various rates of absence of ulcer recurrence at the 5-year follow-up, depending on the etiology. In primary reflux, the rate is about 70%, whereas in PTS, the rate is between 40 and 80%.
Conversely, surgery to eradicate primary varices is indicated in the absence of deep venous insufficiency to prevent ulcer recurrence. The management of perforator is more problematic, but a degree of consensus exists with regard to endoscopic ligation of incompetent large-caliber perforators of the leg.
The indications for reconstructive surgery of the deep vein network for both obstruction and reflux remain controversial as there is no RCT study, but it must be kept in mind that in the case series reported, deep vein surgery was in all cases undertaken after failure of conservative treatment.
Wael Tawfick, Sherif Sultan
Western Vascular Institute, Department of Vascular and Endovascular Surgery, University College Hospital, Galway, Ireland; The Galway Clinic, Doughiska, Galway, Ireland; Embricon Innovation Centre, NUIG, Galway, Ireland
Venous ulceration has an incidence of 3/1,000 population and 20/1,000 population in octogenarians. Topical wound oxygen (TWO2) proposes an option for management of refractory venous ulcers, without the adverse effects of a full-body hyperbaric chamber.
The aim of this study is to prove the safety and efficacy of TWO2 in managing refractory venous ulcers. Primary end points are the proportion of ulcers healed, percentage of reduction in ulcer size, time to full healing or skin grafting, and bacterial elimination at end of therapy. Secondary end points are pain reduction and recurrence rates.
Ulcers were measured using Visitrak to determine surface area, maximum width, and length. Punch biopsies were taken from all ulcers. Necrotic tissue was débrided. In the TWO2 group, the limb was placed in a TWO2 chamber for 180 minutes bidaily at 50 mbars pressure, with oxygen supplied at 10 L/min. The compression group was managed using Profore compression dressings. Ulcers were digitally photographed and measured at 3-day intervals and swabbed weekly.
Forty-six chronic refractory nonhealing ulcers of more than 2 years’ duration were managed using TWO2 and 36 with compression dressings. Both groups were comparable regarding risk factors, demographics, ulcer size, and location. All patients were classified as C6 in the CEAP classification. At 3 months, 80% of TWO2-managed ulcers (n = 37) were completely healed, compared with 25% (n = 9) of the compression group (p < .0001). The mean time to 70% reduction in surface area was 22 days in the TWO2 group as opposed to 125 days in the compression group (p < .0001, 95% CI -176.774 to -101.641). The mean time to full healing or skin grafting was 62 days in TWO2 patients and 187 days in compression patients (p < .0001, 95% CI -209.922 to -82.0779). Eighty-seven percent of TWO2 ulcers (n = 40) healed by reverse gradient (from the center of the ulcer outward). Three patients were referred for primary amputation following failure of compression therapy and skin grafting. All of these three fully healed using TWO2 therapy. Seventeen ulcers were MRSA+ve prior to TWO2 therapy, 9 of which became MRSA-ve after TWO2 treatment. This is compared with 18 MRSA+ve ulcers managed by compression dressings, all of which remained positive after treatment (p = .033). Six of the TWO2-managed ulcers were skin grafted. All six went on to fully heal. Using a pain numerical rating scale, the pain score threshold in the TWO2 managed patients improved from 8 to 3 by 13 days. Two refractory ulcers due to associated staphylococcal scalding skin syndrome improved remarkably on TWO2 therapy, both completely healing within 4 weeks. Three TWO2-managed ulcers showed no signs of healing. One of these ulcers was exposing underlying tendon and bone. The other two proved positive for malignancy. No local or systemic complications were witnessed in either treatment group. After 3 months of follow-up, 3 of the 9 healed compression dressing ulcers showed signs of recurrence compared with none of the 37 TWO2-healed ulcers.
TWO2 is a valuable tool in managing chronic non-healing venous ulcers. We believe that TWO2 is safe and effective in refractory venous ulcer management, without the risks of full-body hyperbaric chambers.
17.38–17.48 Discussion
SESSION XV: Venous Disease II: Modern Management Deep Vein Thrombosis
Moderators: Alan Dardick, MD, PhD, Mark Morasch, MD
Martin Feeley
Department of Vascular Surgery, The Adelaide and Meath Hospital incorporating the National Children's Hospital, Tallaght, Dublin, Ireland
Conventional wisdom/teaching taught us that phlebitis approaching the saphenofemoral junction should be treated as a relative emergency by saphenous ligation to prevent propagation to the deep system. That propagation to the common femoral vein from the great saphenous or popliteal from the lesser saphenous can occur is not in doubt.
It seems difficult to reconcile this with the new varicose vein treatment modalities. The objective of both heat-induced (laser and radiofrequency) and foam sclerotherapy is to induce thrombosis of the saphenous vein up to the junction.
In patients in whom thrombus propagation into the deep system has occurred, treatment is almost exclusively anticoagulation, initially with heparin followed by 3 to 6 months of warfarin therapy.
Perhaps not surprisingly, studies have shown that anticoagulation is more effective in preventing development of DVT than saphenous ligation. But is 3 to 6 months of warfarin therapy preferable to ligation, which can be easily completed under a local anesthetic?
The real question is, of course, which patients need treatment in the first place? With the use of the newer varicose vein treatment modalities, this now becomes a very pertinent question.
Anil P. Hingorani, MD
College of Medicine, SUNY Brooklyn and Maimonides Medical Center, Brooklyn, New York
Anthony J. Comerota, MD, FACS, FACC Jobst Vascular Center, Toledo, Ohio, USA
_
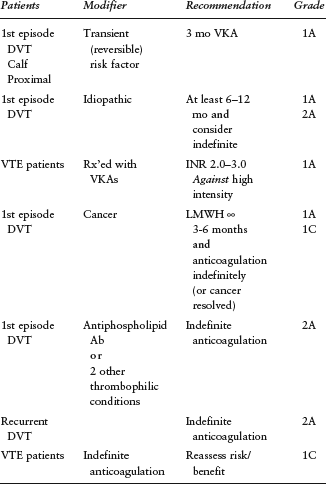
18.09–18.19 Discussion
SESSION XVI: Miscellaneous Topics
Moderators: J. Gregory Modrall, MD, Piergiorgio Cao, MD, FRCS
David L. Gillespie, MD, RVT, FACS, DMCC Uniformed Services University of the Health Sciences, Vascular Surgery, Walter Reed Army Medical Center, Bethesda, Maryland, and Washington, DC, USA
John G. Laffey
Department of Anaesthesia, National University of Ireland, Galway and Galway University Hospitals, Galway, Ireland
Inflammation constitutes a generalized, nonspecific response to tissue injury, of whatever etiology, and is a rapid, highly amplified, controlled humoral and cellular response. The physiologic trespasses of surgery and the perioperative period provoke a vigorous inflammatory response. This inflammatory response is well tolerated by most patients but may result in especially deleterious consequences in some individuals. Nonspecific activators of the inflammatory response to surgery include surgical trauma, blood loss and/or transfusion, and hypothermia.
The inflammatory response to cardiac surgery is increasingly well characterized and provides a useful model of the stress response to surgery in general. Scientific knowledge in this field is continually expanding, and this area constitutes a major interface of clinical and basic scientific research. Cardiopulmonary bypass (CPB) may directly activate the inflammatory response via at least three distinct mechanisms. One mechanism involves direct “contact activation” of the immune system following exposure of blood to the foreign surfaces of the CPB circuit. A second mechanism involves ischemia-reperfusion injury to vital organs as a result of aortic cross-clamping. Restoration of perfusion on release of the aortic cross-clamp is associated with activation of key indices of the inflammatory response. In addition, systemic endotoxemia, resulting from gut translocation of endotoxin across a damaged mucosal barrier compromised following splanchnic hypoperfusion, may indirectly activate the inflammatory cascade.
There are several key components to the inflammatory response to cardiac surgery. The complement cascade is activated upon contact of the blood with the foreign surfaces of the extracorporeal circuit, reperfusion of ischemic tissues, and heparin neutralization with protamine. Proinflammatory cytokines such as tumor necrosis factor α, interleukin-1 (IL)-β, IL-6, and IL-8 play a pivotal role in stimulating and coordinating the inflammatory process. The role of the coagulation/fibrinolytic cascades and its interaction with the inflammatory response are increasingly recognized. The cellular immune response, in particular the process of neutrophil-endothelial adhesion, may lead to widespread endothelial damage and dysfunction. The inflammatory response may result in widespread endothelial activation and diffuse endothelial injury, which is considered a key event leading to widespread organ injury and dysfunction.
The clinical consequences of inflammatory response constitute a pathophysiologic continuum, from a mild generalized transient response, termed the systemic inflammatory response syndrome [SIRS], to life-threatening organ dysfunction. Although SIRS is well tolerated by most patients and may have important beneficial effects, a significant minority of patients progress to the development of single or multiple organ dysfunction, termed multiple organ dysfunction syndrome. The factors that influence the incidence, severity, and clinical outcome of the inflammatory response, and in particular the reasons why certain patients develop life-threatening perioperative complications, are currently not well understood.
The therapeutic potential of strategies to control the inflammatory response, particularly the inflammatory component of the response, is clear. Off-pump coronary artery bypass (OPCAB) techniques, which avoid the need for extracorporeal circulation, attenuate the inflammatory response and appear to confer clinical benefit. Concerns regarding the quality of the revascularization following OPCAB appear to have been allayed. In patients undergoing CPB, strategies to improve the biocompatibility of the extracorporeal circuit, such as heparin coating, and modifications of the perfusion technique, such as modified ultrafiltration, hold promise. Strategies to maintain perioperative hemodynamic stability, such as enoximone therapy, may be beneficial, particularly in elderly patients. Direct antimediator therapies that focus on key effector molecules and pathways of the inflammatory response offer future therapeutic options.
Despite this, the optimal anti-inflammatory therapeutic strategy (or strategies) and the optimal target subgroup of cardiac surgical patients remain to be fully elucidated. Our goal must be to attenuate the deleterious effects of the stress response while preserving the ability of the patient to mount an appropriate defense to the physiologic trespasses of the perioperative period. Modulation of the stress response, rather than simple inhibition, is likely to confer substantial benefit. Furthermore, therapeutic strategies should be focused on the subset of cardiac surgical patients most likely to suffer deleterious consequences and hence most likely to experience benefit. This subgroup of high-risk patients is increasingly well characterized. Large-scale clinical trials of the more promising therapeutic strategies, restricted to the patient group at significant risk of perioperative morbidity, and hence most likely to experience benefit, are urgently needed.
D.P. Mikhailidis
Department of Surgery and Department of Clinical Biochemistry (Vascular Disease Prevention Clinics), Royal Free Hospital Campus, University College London, London, United Kingdom
The US guidelines recommend low-density lipoprotein cholesterol (LDL-C) level targets of 2.6 mmol/L (100 mg/dL) and 1.8 mmol/L (70 mg/dL) for high-risk and very high-risk patients, respectively. In the United Kingdom, some guidelines recommend a target of 2.0 mmol/L (80 mg/dL).
In PROVE IT-TIMI, 22 pravastatin (40 mg) and atorvastatin (80 mg) were compared in patients (n = 4,162) with acute coronary syndrome (ACS). The reduction in LDL-C was significantly (p = .001) greater with atorvastatin, as was the primary composite end point (n = .005). The TNT trial showed that in patients (n = 10,001) with stable coronary heart disease (CHD), atorvastatin 80 mg/d was more effective than atorvastatin 10 mg/d. The A to Z trial (different doses of simvastatin in 2,232 patients with ACS) and the IDEAL study (simvastatin 20 mg vs atorvastatin 80 mg in 8,888 patients with previous myocardial infarction) also broadly support the concept of “lower is better” for cholesterol levels. This conclusion was confirmed by a meta-analysis. However, there is evidence showing that the highest doses of statins are not well tolerated.
It is also relevant that in HPS (n = 20,536 high-risk patients, follow-up 5.0 years; simvastatin 40 mg vs placebo), those with a baseline LDL-C < 2.6 mmol/L (100 mg/dL) still benefited from treatment.
Ezetimibe, a selective cholesterol transport inhibitor, has proven useful in the struggle to lower LDL-C levels. A recent meta-analysis showed that ezetimibe added to a statin lowered LDL-C by a further 23%.
Just prescribing statins is not enough–-we need to achieve targets!
Wael Tawfick, M. O'Connor, S. Tawfik, N. Hynes, Sherif Sultan
University College Hospital, Galway, Ireland; Department of Vascular and Endovascular Surgery, Galway Clinic, Doughishka, Galway, Ireland
Recombinant activated factor VII (rFVIIa) is considered a universal hemostatic agent. We present our experience with rFVIIa in vascular surgery patients who developed major hemorrhagic complications with no obvious major vessel bleeding as an expansion of the indications of rFVIIa.
Of 973 major complex vascular procedures, 18 patients with intractable bleeding were administered 40 to 80 Ag/kg rFVIIa. Blood and by-products transfused, pH, coagulation profile, platelet count, and preoperative antiplatelets and anticoagulants were recorded.
Twelve patients (67%) showed clinical improvement. Six remained unstable despite further hemostatic measures and died perioperatively. Thirty-three percent (n = 6) received over 20 U of blood before rFVIIa administration. All but one died within the first 24 hours (p = .0175). Seven patients had acidosis with a pH of 7.3 or less. Five of them died within 24 hours (p = .05). Six patients had a platelet count below 100,000/cm3, five of whom died perioperatively (n = .0175). Patients with an international normalized ratio above 1.2 had a better survival rate because rFVIIa was used early. There were no signs of systemic or local thrombotic events. The amount of blood and plasma transfused was significantly reduced after rFVIIa administration.
rFVIIa is a safe adjunct for patients with significant hemorrhagic complications, with a low risk of thrombotic complications. We found it effective if administered early with measures to achieve hemodynamic stability and correction of acidosis.
Arshad Hussain, Sherif Sultan
Western Vascular Institute, Department of Vascular and Endovascular Surgery, University College Hospital, Galway, Ireland; The Galway Clinic, Doughiska, Galway, Ireland
Neurovascular compression due to thoracic outlet syndrome (TOS) is gruelling to gauge because of the variability of symptoms, and procedural success can be capricious. Scalenectomy is considered an effective treatment for TOS and decompression of the thoracic outlet.
The purpose of this study was to evaluate the effectiveness and the functional outcome of scalenous anterior resection by supraclavicular approach and the validity of DASH scoring as an assessment tool in the management of TOS.
Between March 2005 and September 2007, 20 patients underwent 24 scalenectomies and brachial plexus neurolysis by supraclavicular approach. Two had cervical rib resection. The mean age was 34.3 years (range 16–62). Eight patients were male and 12 were female. The mean follow-up was 15 months. Primary symptoms were vascular in 4 patients and neurogenic in 16 patients. All had intolerable pain and arm claudiacation. All patients underwent radiography of the cervical spine, segmental arterial pressures (two cervical ribs, three reduced pressures on abduction), duplex scan, and magnetic resonance imaging (three subclavian artery and one vein impingement). The common pathologic feature was adhesions, infiltration, and scissoring effect of anterior and medial scalene muscles on the brachial plexus, in spite of normal findings on MRI.
Symptomatic improvement was encountered after 92% of procedures. One patient, with positive lupus antibodies, had no change in vasospastic symptoms. The DASH scoring system was used in assessment pre-and postoperatively. The mean preoperative DASH score for patients with vascular symptoms was 55.75 as opposed to a mean postoperative score of 30.5 (mean difference 25.25, p = .21, 95% CI 25.32–75.82). The mean preoperative DASH score for patients with neurogenic symptoms was 27.33 in comparison with a mean postoperative score of 8.83 (mean difference 18.5, p = .012, 95% CI 6.085–30.91). Overall primary symptom improvement was statistically significant; p = .002.
The supraclavicular approach provides excellent revelation for thoracic outlet decompression. Anterior and middle scalenectomy with brachial plexus neurolysis provides adequate relief of TOS symptoms. Patients with neurogenic symptoms primarily have better relief of symptoms, and DASH scoring provides an excellent assessment tool.
Chris Beirne, Sherif Sultan
Western Vascular Institute, Department of Vascular and Endovascular Surgery, University College Hospital, Galway, Ireland
Triona Walsh, Wael Tawfick, Sherif Sultan Western Vascular Institute, Department of Vascular and Endovascular Surgery, University College Hospital, Galway, Ireland; The Galway Clinic, Doughiska, Galway, Ireland
Surgical site infection (SSI) remains an important complication of surgical interventions and is associated with high mortality and morbidity rates. Candidates for vascular surgery have high incidences of comorbidities, including diabetes mellitus and renal impairment.
The aim of this study is to assess the influence of the introduction of a wound care protocol on the incidence of SSI. The primary end point is the incidence of SSI. Secondary end points are length of hospital stay, organisms isolated, and incidence of secondary interventions.
The wound care protocol for all wounds involved the use of a Stryker Interpulse System for antibiotic (cefuroxime) irrigation prior to closure, an absorbable monocryl subcuticular suture to close the skin, and tissue adhesive 2-octyl cyanoacrylate (Dermabond) application to the wound edges. No dressings were used to cover any surgical wound.
Comparison was made between the incidence of SSI in patients treated during a 6-month period prior to the introduction of this wound care protocol (January to June 2004 inclusive) with that of patients who underwent procedures after the introduction of this protocol (January to June 2006 inclusive) in a specialized vascular and endovascular unit in a tertiary referral center.
The incidence of wound infections, causative organism(s), and vascular-related risk factors was recorded from detailed review of medical notes, nursing notes, and microbiology records.
Demographics and vascular risk factors were similar in both groups. During the control period, 123 vascular/endovascular procedures were performed on 119 patients. During the study period, 128 procedures were performed on 122 patients. There was no significant difference in the breakdown of procedures performed in either group. During the control period, 28 SSIs (28/123 procedures) were diagnosed (20.3%) as opposed to 15/128 (11.7%) in the study period (p = .025). There was no significant difference in the incidence of SSI within each individual procedure group.
The introduction of this wound care protocol has positively improved the incidence of SSIs. Meticulous attention to detail during wound closure significantly improved the outcome of vascular surgical procedures.
Elrasheid A.H. Kheirelseid, Aidan Devitt,
Martin Cormican
Royal College of Surgeons in Ireland, Surgical SHO,
Galway University Hospital, Galway, Ireland; Merlin
Park/Galway University Hospital, Galway, Ireland; Galway University Hospital, Bacteriology, NUI, Galway, Ireland
Six of the visitors (5.6%) gave a history of MRSA colonization or infection, 11 (10.2%) had a previous contact with patients with MRSA infection, and 50 (46.3%) had visited another hospital or nursing home in the last 2 weeks. In addition, 13.9% had chronic medical illnesses, including diabetes mellitus, hypertension, and asthma; 7.4% were admitted to hospitals during the previous 3 months; 75 (52.8%) had direct contact with animals and pets; and 10.2% had recent antibiotic therapy. MRSA was not isolated from the nose of any participant.
19.05–19.15: Discussion
19.15 ADJOURN