
Abstract
In carotid endarterectomy (CEA) patients, platelet aggregation is increased despite heparinization. We investigated whether this phenomenon correlates with the occurrence of perioperative microemboli. Of 27 CEA patients, 18 (67%) used aspirin and 9 also used clopidogrel. Blood was collected at multiple time points before, during, and after CEA. Platelet aggregation and P-selectin expression were determined. Transcranial Doppler monitoring was used to measure microemboli. Platelet aggregation showed a significant increase 5 minutes postheparinization compared with preheparinization (19.7 ± 2.8% vs 8.9 ± 0.9% in the aspirin group and 22.5 ± 4.4% vs 8.7 ± 1.2% in the clopidogrel group; p < .01 and p < .05, respectively). P-selectin expression showed a tendency to increase postheparinization in both groups (p = .07 and p = .09, respectively). The number of microemboli ranged from 0 to 50. Clopidogrel patients displayed fewer microemboli than aspirin patients (4.1 ± 2.3 vs 17.6 ± 18.2; p < .01). Patients with a high number of microemboli displayed had a tendency toward higher baseline platelet aggregation than patients with a low number of microemboli (p = .08). In conclusion, platelet aggregation is transiently increased during CEA despite the administration of antiplatelet agents. Clopidogrel is associated with a decreased number of perioperative microemboli. The exact relationships between these findings, postoperative microemboli formation, and the risk for thromboembolic complications after CEA remain to be determined.
Carotid endarterectomy (CEA) significantly reduces the risk of recurrent ischemic events in patients with severe internal carotid artery stenosis. 1 Nonetheless, perioperative thromboembolic events still provoke most CEA-related major complications, such as stroke and death. 2,3 To reduce the risk of such adverse events, antithrombotic medications such as heparin, aspirin, and clopidogrel are administered. 4–6 However, recent data show that, in some patients, platelet aggregation actually increases during some stages of CEA. 7 This appears to be an indirect effect induced by the administration of heparin during surgery. 8 Because the combination of aspirin with clopidogrel has been shown to reduce P-selectin-mediated platelet activity 9 and to reduce postoperative thromboembolic potential, 4 we investigated whether the platelet aggregation increase occurs in the presence of clopidogrel, whether it is P-selectin mediated, and whether it correlates with the occurrence of microemboli in the cerebral circulation.
Materials and Methods
Patients
All consecutive patients who underwent elective, primary CEA in our tertiary referral center between May and October 2005 who received treatment with aspirin alone or in combination with clopidogrel for at least 1 month prior to surgery were included on an intention-to-treat basis. Patients were randomized to receive aspirin alone or aspirin in combination with clopidogrel as part of a different trial. Exclusion criteria were platelet disorders or hematologic problems and the use of other antiplatelet drugs or anticoagulants. Ethics committee approval was granted, and all patients gave written informed consent.
Twenty-seven consecutive patients underwent CEA under normocarbic, normotensive general anesthesia. Endarterectomy was performed in all patients with selective use of shunting. A bolus of 5,000 IU unfractionated heparin (Leo-Pharma, Breda, the Netherlands) was given 3 minutes before clamping of the carotid artery. Carotid arteries were reconstructed with either an autologous venous patch or a synthetic patch (Dacron, Invista International, Geneva, Switzerland). Perioperative electroencephalography and transcranial Doppler (TCD) monitoring (as described previously 10 ) were used in all patients. Patients underwent a neurologic examination pre- and postoperatively by a consulting neurologist. Clinical data were collected prospectively.
Blood Collection
To analyze platelet aggregation at specific perioperative stages, blood samples were collected at seven time points: (1) at admission prior to surgery; (2) after induction of anesthesia but before skin incision; (3) 5 minutes after heparinization; (4) 1 hour after heparinization; (5) after 5 minutes in the second postoperative hour; (6) at the end of the second postoperative hour; and (7) 24 hours postoperatively but before the next administered dose of aspirin and clopidogrel (Table 1).
Blood Collection Time Points
Blood was collected in Vacutainer tubes (Sarstedt Monovette, Nümbrecht, Germany) using a 21-gauge needle. During the intervention, blood was collected from an indwelling arterial line. Platelet count was measured on the day of admission from an ethylenediaminetetraacetic acid (EDTA) tube to exclude patients with hematologic disorders (PlateletWorks, Helena Laboratories, Beaumont, TX). Subsequent samples were taken into trisodium citrate for further analysis.
Platelet Aggregometry
Platelet-rich plasma was obtained from citrated blood by centrifugation for 10 minutes at 200 g and was adjusted to 250 × 10 9 platelets/L by adding homologous platelet-poor plasma (centrifuged at 3,309 g for 15 minutes). Platelet aggregation was measured without stimulation, in response to 1.6 mmol/L arachidonic acid (Bio/data Corporation, Horsham, Pennsylvania, PA) and in response to 5 μmol/L adenosine diphosphate (ADP; DiaAdin, Cressier sur Morat, Switzerland) using an APACT-4 aggregometer (Salm and Kipp, the Netherlands). 11 Aggregation was recorded as the percentage of maximal aggregation, compared with light transmission through autologous platelet-poor plasma. These values were corrected for spontaneous aggregation.
Flow Cytometric Analysis for Expression of P-Selectin
Because P-selectin is a platelet interaction mediator 12 and its expression in acute ischemic stroke patients is inhibited by aspirin and clopidogrel, 13 P-selectin (CD62p) expression was determined using flow cytometry. Analysis was performed using the Epics II XL-MCL cytometer (Beckman Coulter, Mydrecht, the Netherlands), as described elsewhere. 14 In brief, whole blood samples taken into a buffer/citrate tube were processed within 15 minutes of collection. Three microliters of citrated blood was added to 30 μL of 1% paraformaldehyde-based fixative (Isoton II, Beckman Coulter), followed by the addition of 2 μL fluorescein isthiocyanate conjugated CD42a monoclonal antibody (Beckman Coulter). Activated platelets were identified by use of 2 μL phycoerythrin conjugated monoclonal antibody to CD62p (Beckman Coulter). Murine control monoclonal antibody was used to set a threshold for activated platelets. P-selectin expression was expressed as the number of platelets positive for CD62p.
TCD Monitoring
Because TCD monitoring provides insight into the pathophysiology of CEA-related thromboembolic complications, 15,16 we also analyzed the TCD monitoring results in our patients. This procedure has been described in detail elsewhere. 17 Briefly, the occurrence of microemboli was counted perioperatively by an experienced sonographer. Only particulate microemboli were considered to be platelet-related and were therefore used to analyze the association with platelet aggregation. Microemboli detected during shunt placement and at clamp release were probably a result of deairing and excluded for further analysis. The number of microemboli was used as a surrogate outcome measurement.
Data Analysis
The statistical significance of data was determined by Student t-test (normally distributed variables) and Pearson chi-square test (frequencies). The results were expressed as mean ± standard error of mean (SEM), and differences were considered significant at p < .05.
Results
Clinical Characteristics
Of the 27 patients undergoing CEA, 18 patients received only aspirin at a dose of 100 mg/d, and 9 patients received aspirin at a dose of 100 mg/d and clopidogrel at a dose of 75 mg/d. There were no significant differences in the baseline clinical characteristics between the two groups (Table 2). Two-thirds of the patients were male. In the aspirin group, the mean age was 70.8 ± 11 years and the mean body mass index was 27.6 ± 5 kg/m 2 . Four patients (22%) were current smokers, 16 patients (89%) had hypertension, 9 patients (50%) had hyperlipidemia, and 6 patients (33%) had diabetes. The demographics for the clopidogrel group were as follows: two patients (22%) were current smokers, nine patients (100%) had hypertension, seven patients (78%) had hyperlipidemia, and three patients (33%) had diabetes. In the aspirin group, the CEA intervention time was 111 ± 27 minutes, and the clamping time was 42 ± 13 minutes. In the clopidogrel group, the intervention time was 116 ± 28 minutes, and the clamping time was 37 ± 16 minutes. Perioperative carotid artery shunting was performed in four patients (22%) of the aspirin group but in none (0%) of the clopidogrel group. A synthetic patch was used in 10 aspirin patients (56%) and in 4 clopidogrel patients (44%). In all other patients, a venous patch was used. None of the aforementioned variables differed significantly between both groups.
Baseline Clinical Characteristics of 27 Carotid Endarterectomy Patients
ACE = angiotensin-converting enzyme; BP = blood pressure; NS = not significant.
Platelet Aggregation
Baseline platelet aggregation (not corrected for spontaneous aggregation) in response to 1.6 mmol/L of arachidonic acid was higher in the aspirin group compared with the clopidogrel group (14.5 ± 6.1% vs 10.3 ± 3.0%; p < .05, results not shown). Platelet aggregation during specified perioperative time points (see Table 1), corrected for spontaneous aggregation, is shown in Figure 1. Prior to surgery, platelet aggregation in response to arachidonic acid was inhibited to 10.7 ± 1.2% in the aspirin group and 7.5 ± 0.7% in the clopidogrel group. There were no significant changes in aggregation after induction of general anesthesia (8.9 ± 0.9% in the aspirin group and 8.7 ± 1.2% in the clopidogrel group). However, 5 minutes after systemic administration of heparin (see Figure 1, time point 3), platelet aggregation in response to arachidonic acid was increased significantly to 19.7 ± 2.8% in the aspirin group and to 22.5 ± 4.4% in the clopidogrel group (p < .01 and p < .05, respectively). In the 24-hour period following surgery, platelet aggregation gradually decreased to preoperative values in both groups (13.4 ± 1%, 11.2 ± 0.9%, 10.3 ± 1.0%, and 11.1 ± 1.2% in the aspirin group and 22.2 ± 5.1%, 11.8 ± 1.5%, 11.7 ± 1.2%, and 8.7 ± 1.1% in the clopidogrel group at time points 4, 5, 6, and 7, respectively).

Platelet aggregation in A, aspirin and B, clopidogrel patients in response to arachidonic acid. Values are expressed as a percentage of maximum ± SEM. SEM = standard error of mean.
Platelet aggregation in response to 5 μmol/L ADP was also measured. At all time points, platelet aggregation in response to ADP was significantly higher than aggregation in response to arachidonic acid (Figure 2 vs Figure 1) but showed no significant changes in response to surgery or heparin administration. In the aspirin group, aggregation was 54.1 ± 4.3%, 48.1 ± 2.9%, 54.9 ± 2.6%, 54.1 ± 2.5%, 53.0 ± 1.8%, 52.8 ± 3.0%, and 55.3 ± 2.7%. In the clopidogrel group, aggregation was 33.1 ± 4.1%, 31.9 ± 5.4, 37.5 ± 5.6%, 34.6 ± 5.2%, 33.9 ± 4.0%, 37.0 ± 6.1%, and 35.7 ± 3.4% for time points 1 through 7, respectively (see Figure 2).
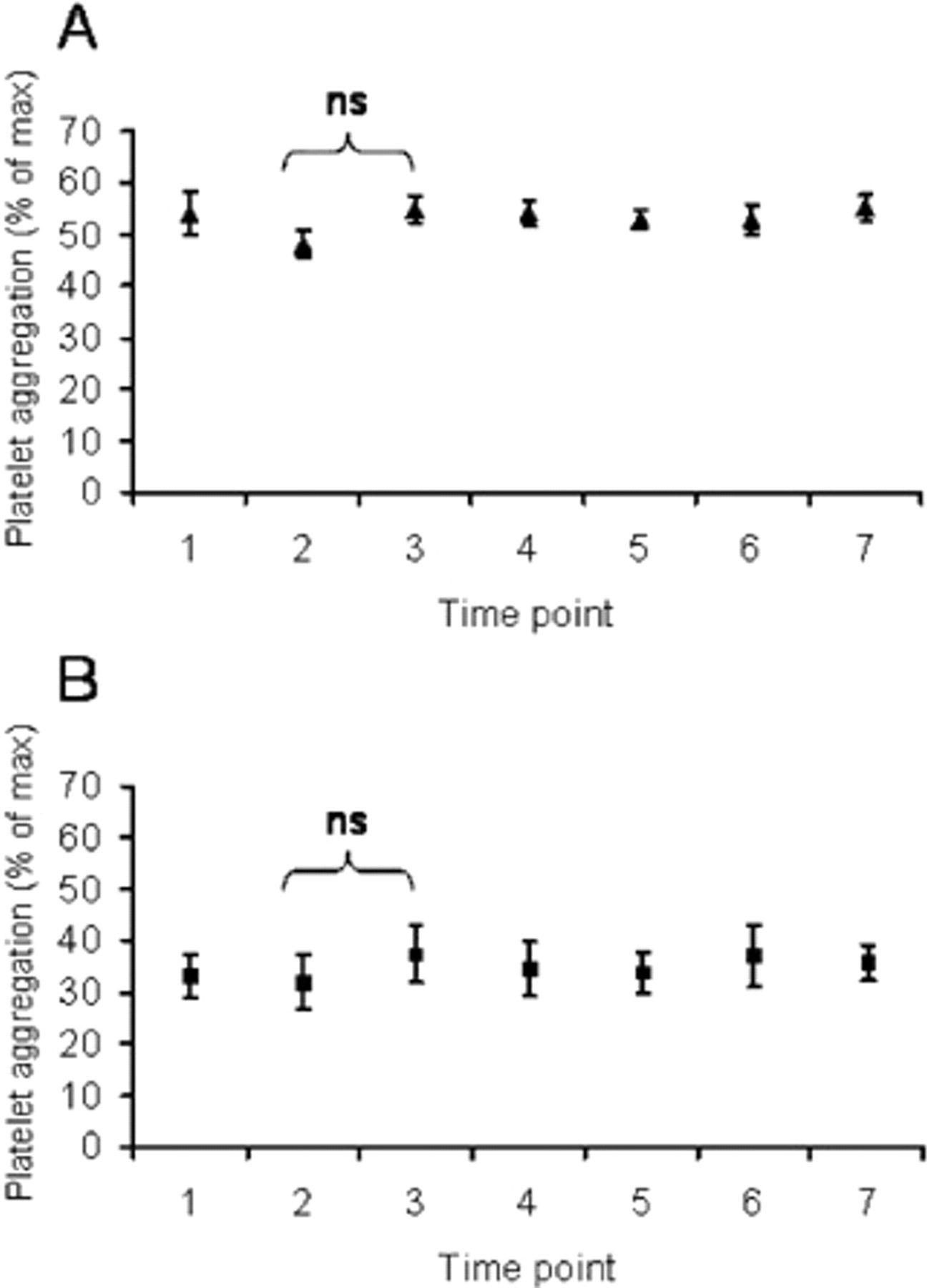
Platelet aggregation in A, aspirin and B, clopidogrel patients in response to adenosine diphosphate. Values are expressed as a percentage of maximum ± SEM. ns = not significant. SEM = standard error of mean.
P-Selectin Expression
Because of its role as a platelet interaction mediator, P-selectin expression was determined by flow cytometry. P-selectin expression (expressed as P-selectin–positive platelets per 10,000 platelets) was 9.6 ± 2.7, 10.6 ± 3.0, 17.7 ± 4.6, 11.3 ± 2.5, 10.4 ± 3.3, 10.6 ± 3.1, and 8.2 ± 2.2 in the aspirin group and 11.2 ± 3.9, 6.3 ± 2.0, 16.7 ± 5.3, 9.3 ± 2.5, 11.1 ± 5.6, 7.5 ± 1.9, and 7.8 ± 2.1 in the clopidogrel group, respectively. P-selectin expression showed a tendency to increase at 5 minutes after heparin administration. However, this increase was statistically not significant (p = .07 and p = .09 in the aspirin and clopidogrel groups, respectively; Figure 3).

Expression of P-selectin in A, aspirin and B, clopidogrel patients. Data are presented as mean ± SEM. ns = not significant. SEM = standard error of mean.
Perioperative Microemboli
To investigate whether the observed increase in platelet aggregation correlates with the number of perioperative measured microemboli, we determined the number of microemboli occurring in our patients using TCD from the start of CEA until the whole second postoperative hour. Figure 4 shows the distribution of patients according to the number of microemboli measured perioperatively. Three patients from the aspirin group and two patients from the clopidogrel group were excluded because, in these patients, no TCD monitoring window could be detected. In the remaining patients, the number of microemboli ranged from 0 to 54. In the aspirin group, 0 microemboli were detected in 1 patient, up to 10 microemboli were detected in 7 patients, 11 to 20 microemboli were detected in 2 patients, 21 to 30 microemboli were detected in 1 patient, 31 to 40 microemboli were detected in 2 patients, 41 to 50 microemboli were detected in no patients, and 51 to 60 microemboli were detected in two patients. In the clopidogrel group, up to 10 microemboli were detected in 7 patients. Comparing both entire treatment groups, a significantly lower number of microemboli was detected in the clopidogrel group (4.1 ± 2.3 vs 17.6 ± 18.2, respectively; p < .01). In addition, it was found that patients in the aspirin group with a high number of microemboli (> 30) had a tendency toward a higher baseline platelet aggregation than patients with a low number (ie, < 30) of microemboli (19.5 ± 4.9% vs 13.3 ± 5.6%). However, this difference was not statistically significant (p = .08; Figure 5).
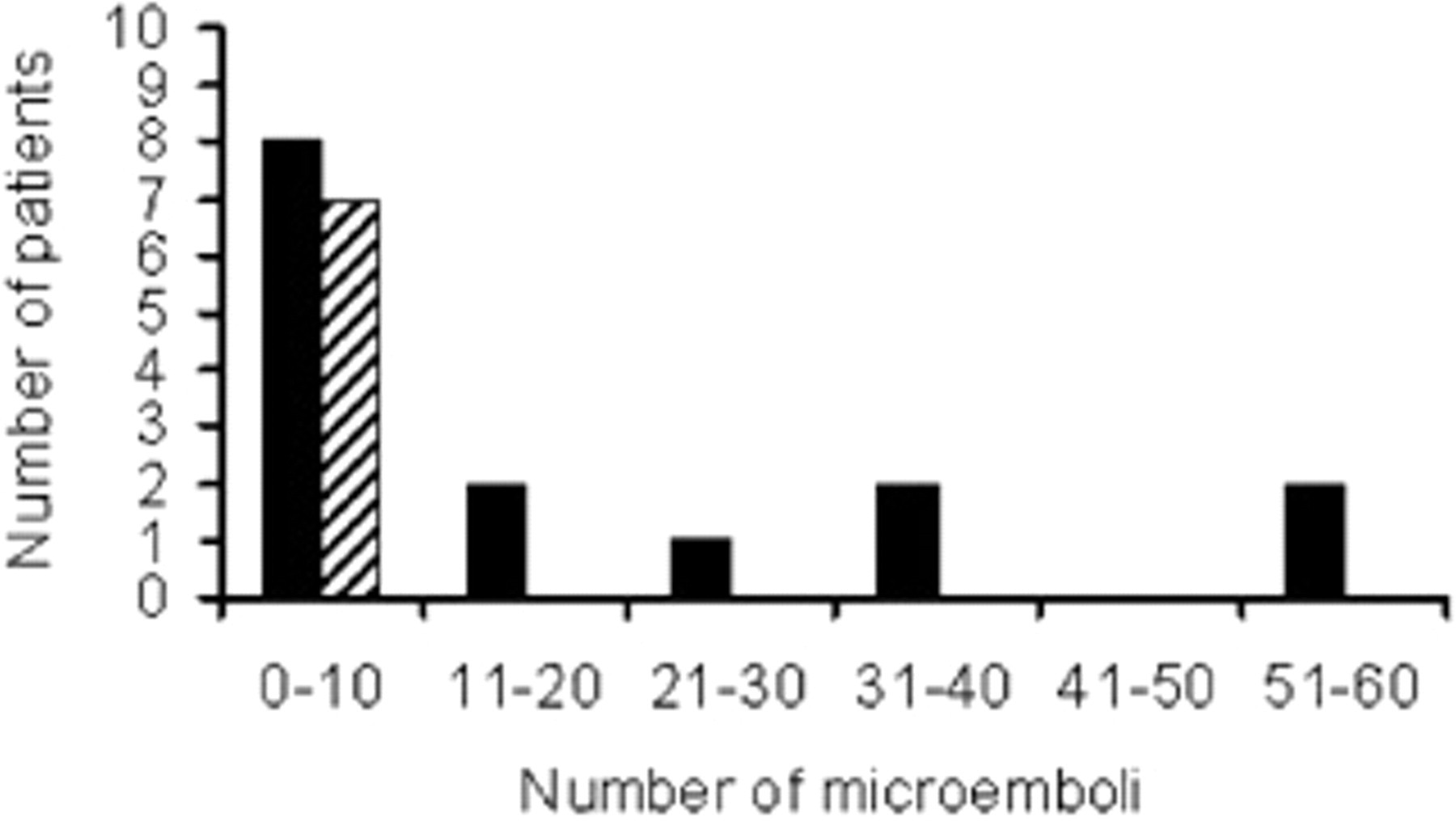
Distribution of perioperative microemboli in aspirin (solid bars) and clopidogrel (dashed bars) patients.
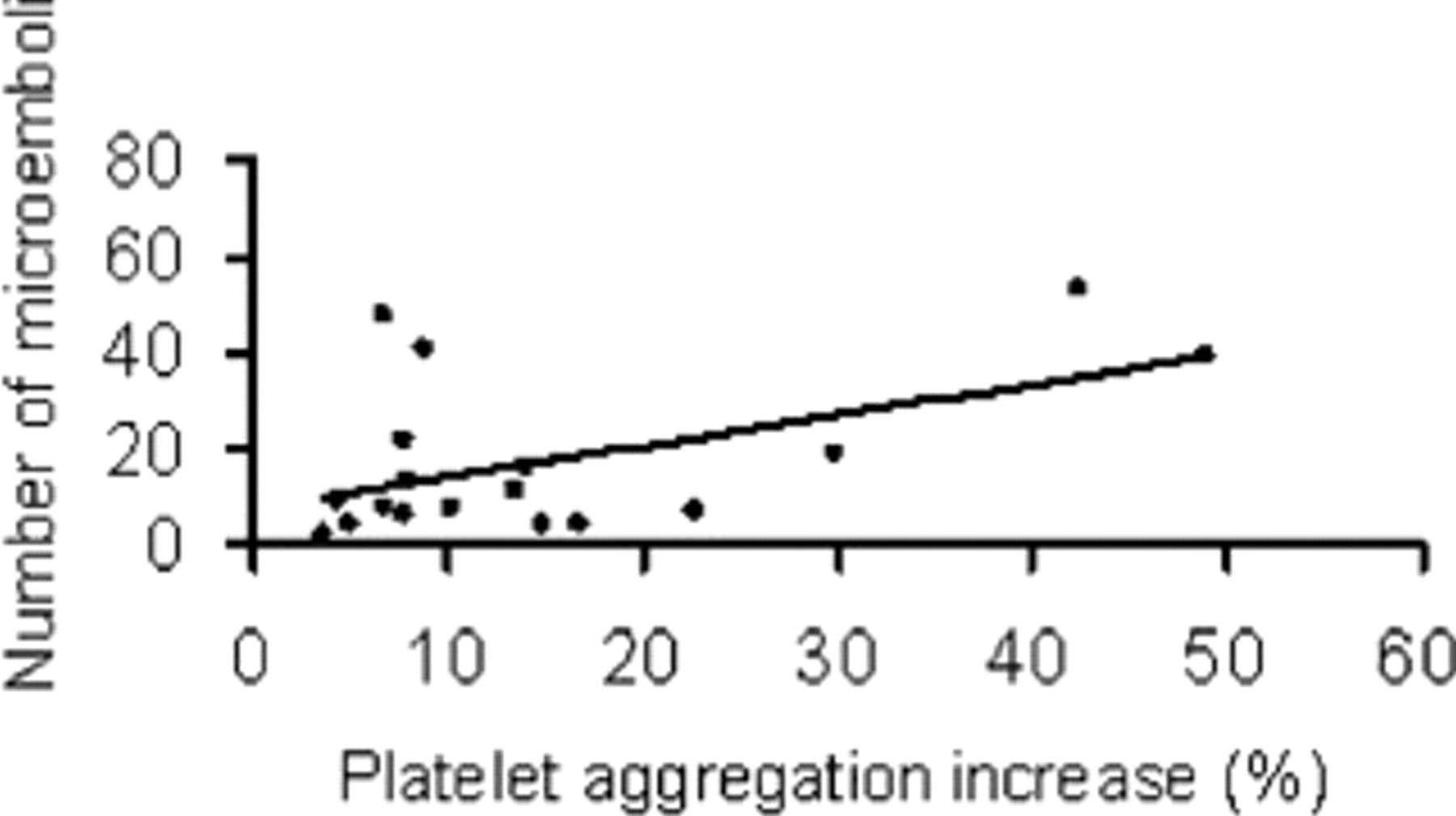
Correlation of perioperative platelet aggregation and number of microemboli in individuals. Pearson analysis showed r 2 = .26.
Discussion
The aim of the present study was to analyze the transient increase in platelet aggregation during CEA despite the administration of antiplatelet agents. Our findings show that platelet aggregation in response to arachidonic acid is transiently increased in CEA patients despite the administration of antiplatelet drugs such as aspirin and clopidogrel. The observed increase in platelet aggregation occurred at 5 minutes after heparinization and disappeared during the first postoperative hour.
These results correspond with other reports that showed that the inhibition of platelet function by preoperative treatment with aspirin in CEA patients can be transiently reversed by heparin. 8 Activation of platelets and platelet agonists by heparin in therapeutic concentrations has been reported in other conditions. 18,19 In these studies, it was shown that the addition of heparin to the blood of healthy volunteers increases the expression of P-selectin. 19 In the current study, the expression of P-selectin was slightly, but not significantly, elevated during CEA. The observations can be explained by the limited sample size of our population or by the possibility that the platelet aggregation increase during CEA is mediated by factors other than P-selectin.
One such factor could be the integrin receptor glycoprotein (GP)IIb/IIIa, which is abundantly expressed on the platelet surface and facilitates platelet–fibrinogen interaction. 20 GPIIb/IIIa is hypothesized to play a role in cerebral microemboli formation during adverse events 21 and can be upregulated by heparin. 19 Furthermore, the number of microemboli detected by TCD monitoring in patients with recent symptomatic cerebral embolism can be reduced by tirofiban, a GPIIb/IIIa receptor antagonist. 22
In addition, there are data showing that GPIIb/IIIa-mediated fibrinogen binding to platelets from CEA patients is associated with the amount of postoperative microemboli detected by TCD monitoring. 23 Therefore, further investigation into messenger pathways triggered by the GPIIb/IIIa receptor activation may prove to be a worthwhile effort.
Drug resistance to both aspirin 24 and clopidogrel 25 has been reported, and it appears that patients' unresponsiveness to aspirin predisposes them to clopidogrel resistance. 26 However, the increase in platelet aggregation in our study is transient, and platelet aggregation returns to normal before administration of antiplatelet drugs is resumed. In addition, recent reports suggest that drug resistance may be attributed to a variability in platelet response to ADP and is unaffected by drug administration. 27 Taken together with the observation that the increase in platelet aggregation is transient, it can be concluded that aggregation increase during CEA is mediated by another pathway than resistance to arachidonic acid or ADP inhibition.
Because clopidogrel inhibits the P2Y12 ADP receptor on platelets 28 and because the use of clopidogrel significantly reduces post-CEA embolization, 4 we expected that the clopidogrel group might not exhibit an increase in platelet aggregation in response to heparin. Although the platelet aggregation in patients taking aspirin and clopidogrel was lower at all time points than the aggregation in patients taking only aspirin, the use of clopidogrel was, in fact, associated with a significantly increased platelet aggregation 5 minutes after heparin administration. Adequate studies have demonstrated the clinical efficacy of clopidogrel treatment in addition to aspirin 5 and indicate that the efficacy of clopidogrel to inhibit platelet aggregation is dependent on the individual's preexisting response to ADP and body weight. 27 Because there were no significant differences in body mass index between the aspirin and clopidogrel groups in the current study, the analysis of individual, preoperative, ADP-induced platelet aggregation in our subjects could theoretically reveal a lower ADP response in our study population and thus account for the observed platelet aggregation increase in clopidogrel patients. However, because the complexity of heparin–platelet interaction has not been completely unraveled, other mechanisms could be responsible for a platelet aggregation increase in the presence of clopidogrel.
Because of its ability to detect microemboli prior to the occurrence of thromboembolic stroke, TCD monitoring is an effective tool in evaluating perioperative stroke risk during CEA. 5,15 In our study, there was a tendency for patients with a high number of microemboli to have a higher platelet aggregation. In addition, patients in the clopidogrel group showed a significantly lower number of microemboli during CEA. This finding correlates with other reports showing reduced postoperative magnitude of embolization in patients treated with clopidogrel compared with patients receiving placebo 4 during CEA. Because preoperative platelet characteristics have been shown to be highly variable, 29 we investigated whether the platelet aggregation increase correlated with postoperative embolization. However, there was only a weak correlation (r 2 = .26), which does not reach statistical significance.
A transient increase in platelet aggregation during CEA despite the addition of antiplatelet drugs is a reproducible effect. This aggregation increase occurs despite the addition of clopidogrel. It appears not to be mediated by P-selectin or may be partially mediated by P-selectin and does not correlate with the number of microemboli detected postoperatively by TCD monitoring. However, the use of clopidogrel is associated with a lower overall number of microemboli. Together with existing data, our findings suggest that additional studies could identify patients at risk for post-CEA thromboembolic complications by preoperative platelet aggregation assay and allow for preoperative treatment adjustments. The exact relationships between these findings, postoperative microemboli formation, and the risk for thromboembolic complications after CEA remain to be determined.
Footnotes
Acknowledgments
We thank O. Yasar for aggregation assays and data collection, M. van der Mee for TCD measurements, and F. Haas and H.D.W.M. van de Pavoordt for critical review of the manuscript.