
Abstract
Intimal hyperplasia is the most common final pathway for hemoaccess occlusion in dialysis patients. Drug eluting stents have been shown to decrease intimal hyperplasia in coronary arteries and possibly in peripheral arteries. We evaluated the use of a sirolimus loaded polyurethane graft as prophylaxis in hemodialysis access. Grafts were loaded with sirolimus and elution curves were determined for the polyurethane material. The arteriovenous grafts were then placed in the neck of 20 sheep. A non-loaded graft was placed in the contralateral neck. Patency rates, ultrasound evaluation, angiography and histomorphometry were determined for each graft. At 30, 60 and 90 days the drug loaded graft had improved patency rates compared to the control, with a 25% improvement noted at 3 months. Life table analysis showed the drug loaded graft consistently better patency than the control (p = .136). The control graft had greater neointimal stenosis (14.5% vs 9.17%) over the course of the study (p = .157). Although none of these findings was statistically significant in this pilot study, the sirolimus coated graft out-performed the control in every measured parameter at each time point evaluated. Further work to asses the validity of drug coated materials to prevent intimal hyperplasia in hemodialysis access is warranted.
Intimal hyperplasia is the Achilles heel of hemoaccess for dialysis patients. It is the mode of failure for the vast majority of synthetic grafts and native fistulae. Although native fistulae are the preferred access of choice, many patients have inadequate vessels for a fistula and will require a synthetic graft, and many dialysis units have indicated a preference for synthetic grafts. 1 Native fistulae have a longer primary patency than synthetic grafts, but their secondary patency rates can be similar. 2 Intimal hyperplasia, although occurring in different areas, is a common nemesis for both types of access. Multiple studies have shown that a major part of vessel stenosis is due to the migration of medial and adventitial smooth muscle cells and fibroblasts. 3 It is suggested that these processes, both proliferative and fibrotic, are accelerated and enhanced in this setting, particularly with synthetic grafts, in which noncompliant material meets compliant vessels.
It appears that antiproliferative drugs may help the venous process as well as they have for arterial stenotic disease. 4–6 Drug-eluting stents have been shown to reduce intimal hyperplasia in both animal and human models, with the most experience obtained in the coronary artery position. 7,8 When coated with an antiproliferative agent such as sirolimus or paclitaxel, the stents have performed well at reducing the incidence of restenosis. 9–11 This has been used to treat a stenotic lesion and minimize the recurrence of that lesion. The growth of a stenotic lesion is similar to the intimal hyperplasia seen in hemodialysis access, with proliferation of the smooth muscle cells as the common factor leading to the hyperplastic stenosis. 3 Recent studies have evaluated the use of drug-eluting stents for peripheral vessels, and early indications suggest that a similar benefit can be obtained as for the coronary artery position. 12–14 Early studies in coronary artery patients have shown a 24 to 26% improvement in the restenosis rate in patients receiving the sirolimus-eluting stents. A similar result was found in the superficial femoral artery location for sirolimus-eluting stents, with both studies showing these data at the 6-month follow-up. 10,14 With a generally similar mode of stenosis formation, it was felt that hemodialysis access might benefit from a similar approach.
Taking this concept one step further, it is reasonable to postulate that an initial benefit can be achieved from a drug-eluting graft in preventing intimal hyperplasia from the onset. This became our premise in evaluating a sirolimus-coated hemodialysis graft. It was postulated that a drug-eluting graft would significantly delay the onset of intimal hyperplasia and should result in an improved primary patency and possibly secondary patency for the synthetic graft. In general, stents use a polymer coating as a reservoir for the drug and the drug is released over a period of time after implantation. The graft we investigated uses a proprietary polymer, polyetherurea urethane. 15 To initiate this drug-eluting graft concept, sirolimus was coated onto a polyurethane graft and drug elution curves were determined. An animal model was then chosen for implantation that would aid in the rapid assessment of this premise. Sheep were chosen for their previously documented ability to generate intimal hyperplasia in a more rapid fashion than other laboratory models. 16 The protocol was approved by both the Institutional Review Board and the institutional animal care and use committee.
Materials and Methods
Vectra grafts manufactured by Thoratec Corporation (Pleasanton, CA) were used in the study. The grafts were constructed using Thoratec's polyurethane, Thoralon. Vectra grafts contain three layers: a highly porous luminal layer that enhances intimal tissue adherence, a solid middle layer, and a porous adventitial layer. The adventitial layer contains polyester fibers to prevent the graft from kinking. All three layers are made from Thoralon.
Drug Loading of Vectra Grafts
The Vectra graft was loaded with sirolimus after completing the fabrication of the device. To take advantage of the impermeable characteristic of the graft and the nature of the material, a solvent swelling method was developed to load an approximately 2 cm length of one end of the graft with sirolimus. First, the intimal surface of the graft was loaded with 700 to 900 μg of sirolimus. Next, the outer layer of the graft was loaded with the drug using approximately 900 to 1,000 μg of sirolimus. Finally, the graft was dried in a vacuum oven at room temperature for a minimum of 1 hour to remove any residual solvent.
Drug Release Profile
For evaluation of drug release from the device, Thoralon tubes were used for the study.
The drug release from the film or the device was studied by the following procedure: The drug-loaded Thoralon was suspended in 4% bovine serum albumin solution in buffered saline, and the solution was kept at 37°C. This was gently agitated and changed once a week. A sample of the film or the device was removed periodically and treated with suitable solvent to extract the remaining drug. The concentration of the drug was then analyzed by high-performance liquid chromatography. From the amount of drug remaining at each time point and the known loaded drug concentration, the release profile was obtained.
Graft Implantations
These drug-loaded grafts were then implanted into 20 Suffolk Cross wethers (castrated male sheep) using a carotid to jugular loop configuration. The opposite side of each animal was implanted with a noncoated polyurethane graft, so each animal served as its own control. All grafts were 6 mm in diameter, and anastomoses were done with a CV-6 Gore-Tex (W.L. Gore & Associates, Newark, DE) suture. The sheep ranged in size from 27.9. to 47.4 kg. Their arteries averaged 4.95 mm in diameter, and their veins averaged 8.18 mm in diameter. All of the animals had ultrasound examinations of the anastomotic areas performed at 30 days postimplantation (Figure 1). Six sheep were followed for 30 days, six sheep for 60 days, and eight sheep for 90 days. At the end of the follow-up period, angiography was performed on the sheep (Figure 2) and the grafts were then explanted. Samples were obtained for histologic and morphometric analysis of the venous anastomotic sites. The data were entered into a database (FileMaker Pro, Filemaker, Inc. Santa Clara, Ca), and the demographics were evaluated. Statistical analysis was accomplished using a commercially available program (SPSS, SPSS Inc, Chicago, IL).
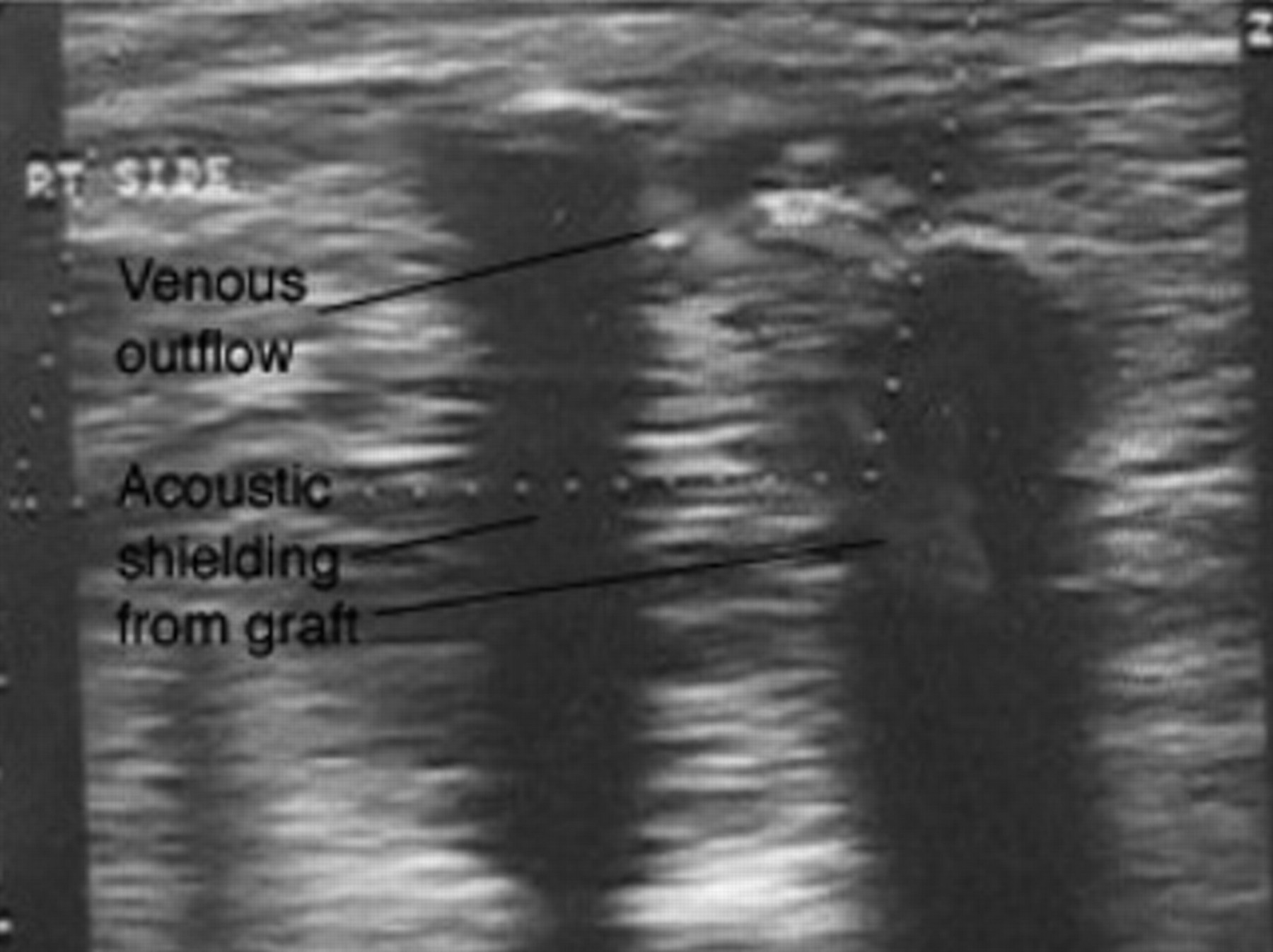
Graft sonogram.

Angiogram of a 3-month-old graft.
Histomorphometry
The explanted venous end of the graft and the vessel were studied by histology. To determine the extent of hyperplasia, the explants were sectioned as represented in Figure 3. The first section, V1, was made as close to the anastomosis as possible. The sections on the vein were made approximately 1 mm away from the toe and heel of the anastomotic ends. After the samples were prepared, the lumen area and the hyperplasia area were determined in all sections. The results were reported in mm 2 for the total lumen area and the neointimal area. The percent stenosis owing to neointima was then calculated from these data. Any acute clots observed in these sections were not included in determining the lumen area open either in the vein or in the grafts.
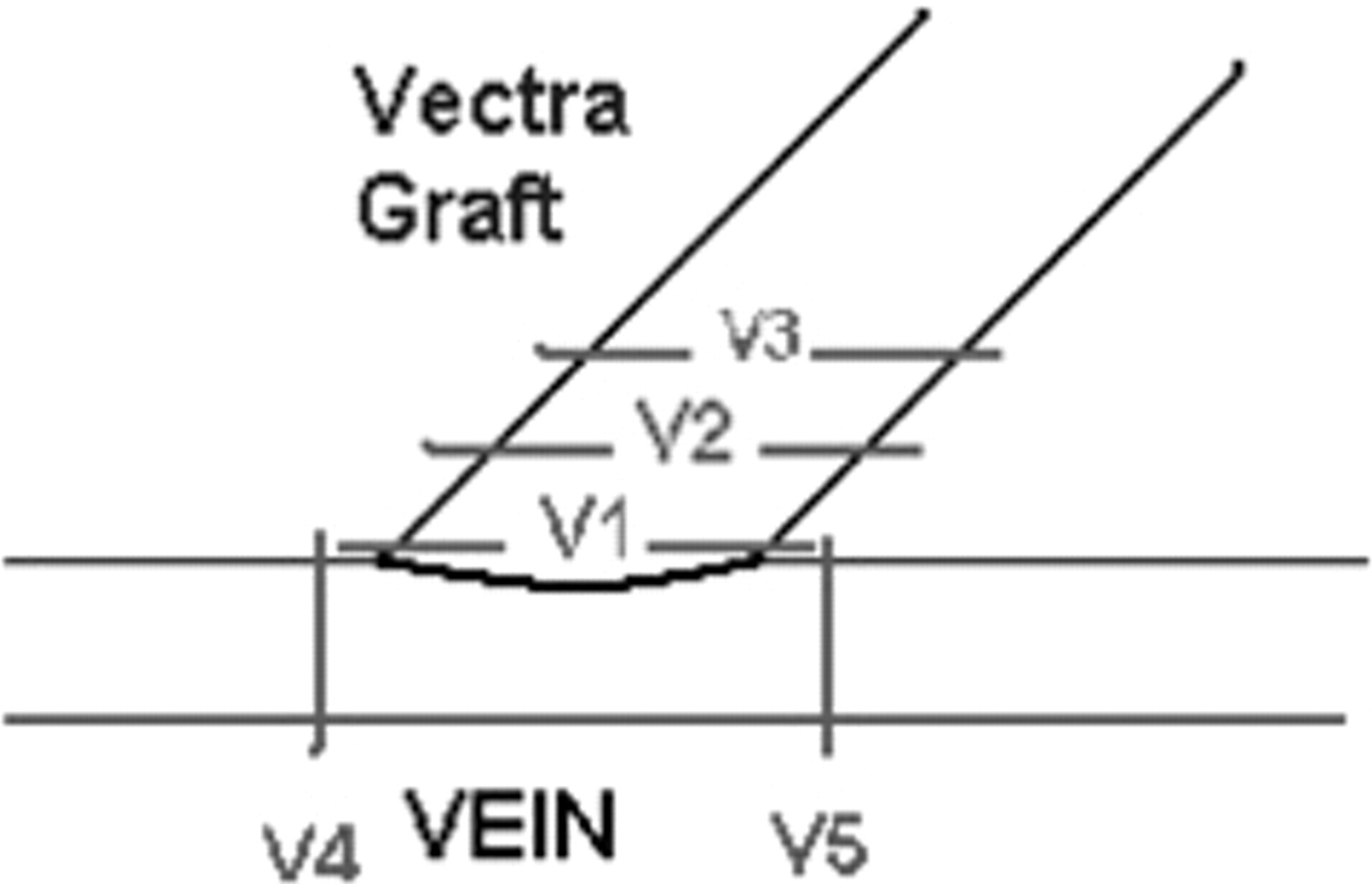
Histology sections of the explanted venous end.
Results
Drug Loading
The sirolimus release profile was obtained from the sirolimus-loaded trilayered design Thoralon tube and is presented in Figure 4. The in vitro release profile from Thoralon suggests that about 70% of the drug is released in the first 40 days. After that period, the curve levels out, with little drug released after 60 days.

In vitro release profile of sirolimus from a trilayered Thoralon construct.
Graft Implantation
The implanted grafts were immediately patent on all animals. There were problems with clotting at the time of implantation for the first two animals. To solve this, and to prevent clotting for the subsequent animals, dosing of 150 to 200 units of heparin/kg was required, and no further clotting episodes were encountered. One sheep had a stroke 30 hours after surgery and was the only perioperative death to occur. This gave a perioperative survival rate of 95%. At 1 month after implantation, the ultrasound evaluation showed that 13 of the 19 coated grafts (68%) were functioning versus 12 of 19 (63%) control grafts.
Patency was assessed at study end points via angiography. In the 1-month group, two of the five grafts were patent on the control side and three of the five grafts on the coated side. At 2 months, four of the six grafts in each arm of the study were patent. In the animals evaluated at 3 months, no control grafts were patent, whereas two of the eight coated grafts were still functioning. Figure 5 shows the life table curves for the coated grafts versus the control grafts. The cumulative patency of the coated graft outperformed the control graft at each time period. However, this was not statistically significant (p = .136).

Life table curves for the coated grafts versus the control grafts.
The histologic analysis showed a range of changes at the anastomotic area from full patency through acute clot to partially organized fibrinous clot to completely organized clot. At 30 days, two of the five coated grafts showed organized clot versus three of the five grafts in the control group. At 60 days, two of the six grafts in the coated group and three of the six grafts in the control group had a well-organized clot. At 90 days, two of the eight grafts in the coated group had an organized clot versus seven of the eight grafts in the control group. Overall, 6 of the 19 anastomoses in the coated group showed an organized clot versus 13 of 19 anastomoses in the control group (p = .149).
Morphometric analysis was used to evaluate the area of neointima, when present, and compare it with overall luminal size. The area of luminal stenosis owing to intimal hyperplasia was then calculated from this morphometry. In each time period, the control group had a higher percentage of neointimal stenosis than the coated group (Figure 6). At 30, 60, and 90 days, the stenosis was, respectively, 9.82, 25.6, and 18.2% in the control group versus 5.2, 13.4, and 7.4% in the coated group. The overall average neointimal stenosis was 14.5% for the control group versus 9.17% for the coated group (p = .157). These measurements were through the anastomosis as a negligible amount of intimal hyperplasia was noted in the venous outflow. The histology of one of the 90-day explants from the control grafts and one of the 90-day explanted drug-loaded grafts is presented in Figure 7.

Percent stenosis from intimal hyperplasia.

Histology of a 90-day explant. A, Drug-loaded graft. B, Control.
Discussion
The benefits of an antiproliferative drug have been studied in a variety of species for the coronary and peripheral locations. 17–19 Systemic and local applications have been evaluated with less systemic toxicity from the local approach. 4,19 Arteries, veins, and synthetic grafts have been studied. 4,19,20 These studies show a consistent benefit from antiproliferative drugs (most commonly sirolimus) in reducing fibrosis and neointimal hyperplasia. This ranged from 12 to 15% in mouse arteries to 25 to 33% in rat arteries and 41% in mouse inferior vena cava.
Sirolimus-coated stents have had a great impact on the outcome of restenosis in coronary arteries. 7–10 Although other agents have been postulated, the antiproliferative drugs have had the most success to date in minimizing intimal hyperplasia. Sirolimus has had the best outcomes in recent clinical studies. 21,22 Data suggest that the initial difference seen at 6 months of follow-up is durable at 2 to 4 years. 23,24 Major studies have shown a 20 to 30% reduction in restenosis rates as determined by angiography. 10 This has led to a 10 to 20% reduction in clinical events. 25,26
The use of this approach to peripheral vessels is less well established. The SIROCCO study showed a benefit for sirolimus-eluting stents in the infrainguinal position. 27 This study is being repeated. The 18-month follow-up showed a slight difference in the rate of restenosis, with 7% less restenosis in the drug-coated arm of the study. The drug-eluting stent had a 6% less rate of occlusion at 24 months. In the SIROCCO II study, there was no difference between a sirolimus-coated stent and a bare stent in the superficial femoral artery at 6 months. At 9 months, there was slightly less restenosis in the drug-eluting stent arm of the study. 28
These data suggest that sirolimus-coated stents may reduce intimal hyperplasia in a durable fashion. We have postulated that this effect can be duplicated in a prophylactic situation as applied to hemodialysis grafts. The intimal hyperplasia seen at the venous end of a graft arteriovenous fistula is similar to that seen in coronary restenosis. It is characterized by smooth muscle cell proliferation, angiogenesis, and matrix deposition. This process is the cause of 80% of all access graft dysfunction.
Using a sheep model for its rapid intimal proliferation, we showed that a polyurethane graft coated with sirolimus decreased neointima formation, decreased organized clot formation, and increased patency versus a standard polyurethane graft. Intimal hyperplasia in the coated graft was reduced by 36% in comparison with that of the control. A completely organized clot was twice as frequent in the control graft as in the coated graft. At 90 days, the cumulative patency of the coated graft was 17% better than the control. These results are similar to those seen from sirolimus-eluting stents placed in the coronary position. Future studies that look at the histomorphometry further down the vein (up to 5 cm) will be of value. This would cover the full range of the perianastomotic stenoses that are seen clinically. The impact of sirolimus at that distance would be interesting to evaluate.
Conclusion
We have shown that polyurethane grafts can be coated with antiproliferative agents and have provided elution curves that illustrate drug release over a 30-day period. These sirolimus-coated grafts can decrease luminal stenosis and improve patency rates when implanted in a sheep model for arteriovenous access. Although this study was not powered to show a statistically significant difference, these data show a consistent difference with improvement in fibrosis, intimal hyperplasia, and patency in the drug-loaded grafts. If validated by further studies, a trial of this approach would be warranted in a clinical setting.