
Abstract
Endovascular repair is increasingly used for ruptured abdominal aortic aneurysms (RAAAs). This study estimated the mortality rate for this approach. A review of 307 publications in English was performed. Thirty-four publications representing 1,200 patients with RAAA were deemed appropriate for analysis by weighted least squares regression. Of the 1,200 patients, 531 (44.3%) underwent endovascular aneurysm repair (EVAR). The average age was 74 years, and 13% were female. Aortouni-iliac grafts were used in 49.4% of patients, and 50.6% received bifurcated grafts. The technical success rate was 94.9%, with a mortality rate of 30.2%. The ratio of endovascular cases to the total number of cases strongly predicted the mortality rate (weighted coefficient −0.378, p < .0003). The mortality rate following EVAR of RAAA is 30%. A 3.8% reduction in mortality was found for each 10% increase in the percentage of ruptures repaired endovascularly at each center. These results are suggestive of a learning curve.
Ruptured abdominal aortic aneurysms (RAAAs) are associated with significant morbidity and mortality. 1,2 In the United States, over 15,000 patients die per year from ruptured aneurysms. 3 In a recent 50-year meta-analysis of the English literature, the overall operative mortality rate for patients with RAAA who underwent open repair was 48%. 4 Despite the advances in care, this study demonstrated only a 3.5% decline in mortality per decade since 1955.
Since the introduction of endovascular aneurysm repair (EVAR) by Parodi and colleagues in 1991, 5 the technique has been widely adopted for the elective repair of abdominal aortic aneurysms. The first successful case of EVAR for a RAAA was performed by the Montefiore group in April 1994 and reported in 1995. 6 The first report of EVAR for a RAAA was reported by the Nottingham group in 1994. 7 Following that, the Montefiore group reported a series of 12 patients who underwent EVAR using a homemade aortouni-iliac device. 8 Following that, Ohki and colleagues reported a series of 12 patients who underwent EVAR using a homemade aortouni-iliac device. 7 Since then, EVAR has being increasingly reported for the treatment of RAAA. The aim of this study was to estimate the overall mortality of patients who undergo EVAR for treatment of RAAA.
Methods
We performed a literature search for “endovascular repair of ruptured abdominal aortic aneurysms” using PubMed (<http://www.pubmed.gov>). Potentially relevant articles were retrieved. Publications that included figures for the total number of patients and mortality were included in the analysis. Several centers had published more than one report of their EVAR series. In these cases, only the data from the most recent publication were included for analysis. The method of selection is depicted in Figure 1. Perioperative, 30-day, and in-hospital mortality data were not uniformly available or defined among different studies. For the purposes of this study, we defined mortality as 30-day and in-hospital mortality pooled together.
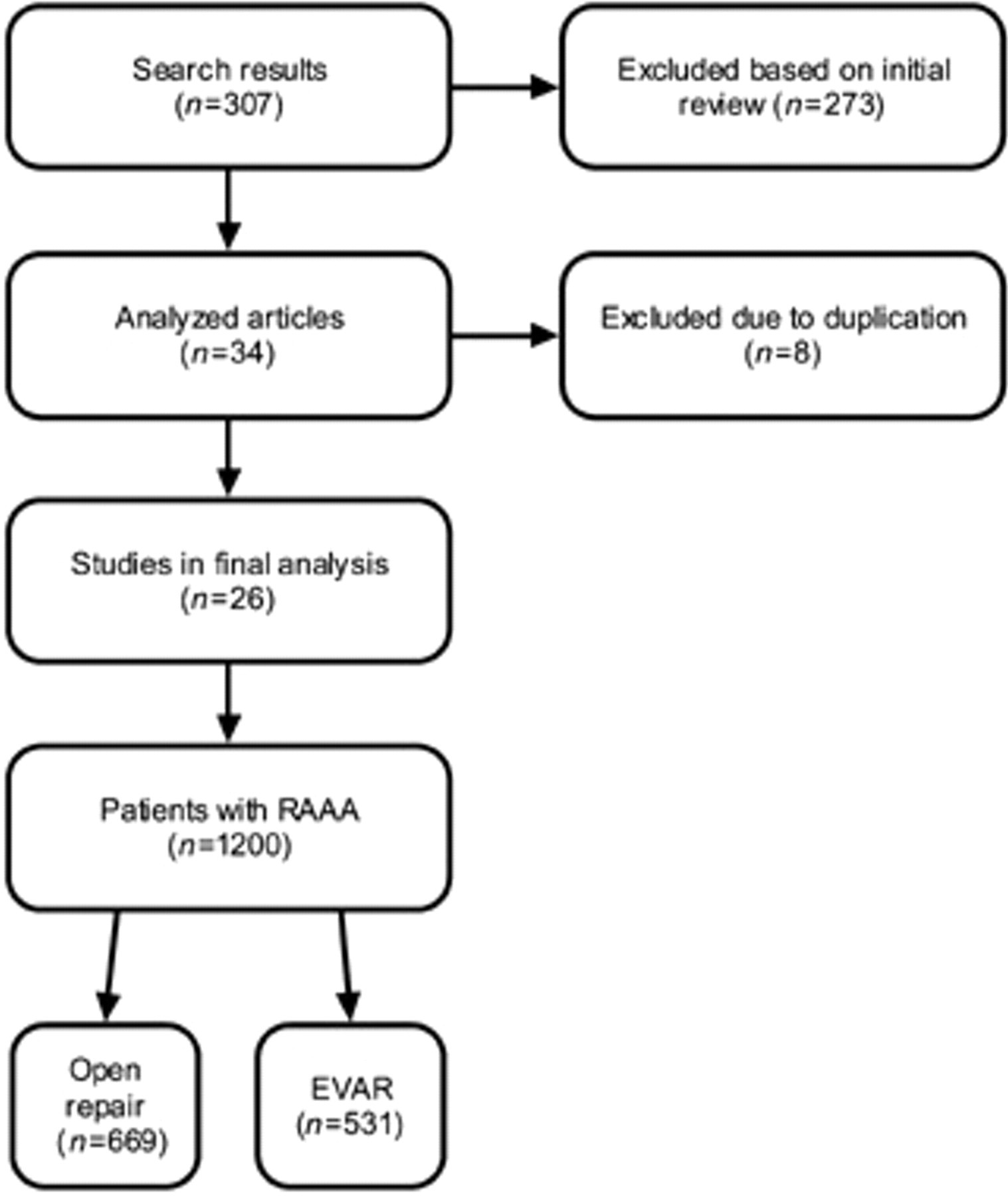
Method of selecting reports from the literature. EVAR = endovascular aneurysm repair; RAAA = ruptured abdominal aortic aneurysm.
Mortality for the series was computed overall by summing the total deaths and dividing by the total sample size. Univariate estimates of continuous variables were performed using means weighted by total sample size for each series. To assess the contribution of case mix volume to mortality outcome, weighted least squares regression was used to compute the appropriate series-weighted estimates. Weighting for regression analysis was done two ways: with weighting by total sample size for each series and with weighting by the inverse of the variance for each series (best linear unbiased estimates regression). Case series reporting 100% endovascular cases were presumed to be reporting only their endovascular experience and were not felt to be representative of the center's total experience. Therefore, for the regression analyses designed to evaluate experience mix, articles reporting only endovascular cases were excluded. Given that treatment comparisons were not generally available in the literature, no odds ratios, forest plots, or other standard meta-analytic details are presented. All computations were performed using SAS version 9.13 for Windows (SAS Institute Inc., Cary, NC).
Results
The literature search identified 307 publications: 273 publications were excluded based on the initial review. This left 34 publications that included figures for the total number of patients and mortality. After the second review, eight of these were excluded because of the publication of a more recent report from the same center (Table 1). 8–41 We included two publications from the Nottingham group because they represented different study periods (1994 to 2000 11 and 2002 to 2004 37 ). The remaining 26 publications representing 1,200 patients with RAAA were included in the final analysis.
Summary of Endovascular Aneurysm Repair Reports
EVAR = endovascular aneurysm repair; NA = not available.
*Excluded from analysis because data from the publication were superseded by a later report.
†Excluded from the EVAR/open repair mortality comparison owing to reporting only endovascular data.
Of the 1,200 patients available for review, 531 (44.3%) underwent EVAR. The remainder underwent open repair. The average age of the population was 74 years, and 13% of patients were female. Preoperative computed tomography (CT) was performed in 88.9% of patients; 49.4% of patients underwent EVAR using aortouni-iliac grafts, with the remainder undergoing bifurcated graft placement. It was difficult to retrospectively identify the type of graft that was placed in the patients who died. However, we found no significant difference in mortality in centers that primarily used aortouni-iliac devices compared with centers that primarily used bifurcated devices. The overall technical success rate was 94.9%. The weighted mortality was 30.2%. The percentage of case mix done endovascularly ranged from 5 to 100%, with a mean of 44.3% EVAR cases. After excluding six publications describing only endovascular experience, the ratio of endovascular cases to the total number of cases was a strong predictor of mortality. Each 10% increase in the percentage of cases done endovascularly was therefore associated with a 3.8% reduction in mortality (sample size-weighted coefficient −0.38, p < .0003). With observations weighted inversely to their variance in best linear unbiased estimates regression, the coefficient was −0.49 (p < .0001), indicating a 4.9% mortality reduction for each 10% increase in the proportion of cases done endovascularly. A weighted linear regression of the relationship between mortality and the percentage of RAAA patients repaired by EVAR is shown in Figure 2.
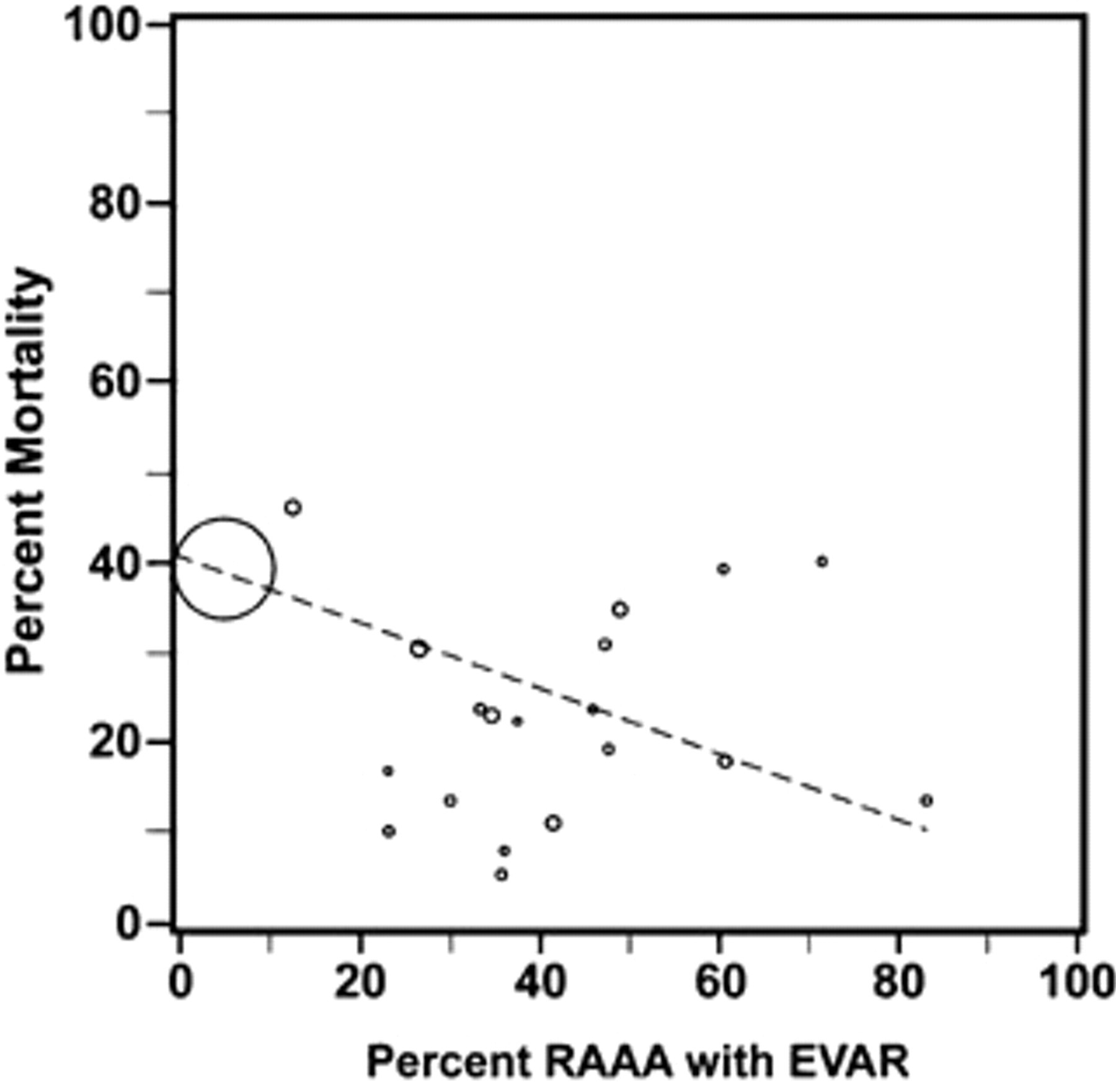
Weighted linear regression showing relationship between mortality and the percentage of ruptured abdominal aortic aneurysm (RAAA) patients repaired by endovascular aneurysm repair (EVAR).
Discussion
Our study demonstrates a short-term mortality of 30.2% for patients undergoing EVAR. The most recent meta-analysis of open repair for patients with RAAA revealed a 48% overall mortality. 4 Comparing these results demonstrates a 17.8% reduction in mortality for EVAR compared with open repair.
Although the results of EVAR appear to be very promising, several limitations to this study should be mentioned. To begin with, this was a retrospective analysis. Both the amount and quality of data reported in different publications were highly variable. In the early stages of our research, we attempted to analyze multiple data points, including patient risk factors, intraoperative variables, postoperative complications, and follow-up. However, owing to the paucity of available data, we limited our analysis to a very small number of variables. These included the total number of cases, the number of EVAR cases, the type of device (aortouni-iliac vs bifurcated), the presence of preoperative CT scans, the technical success rate, and the overall mortality. Perioperative, 30-day, and in-hospital mortality data were not uniformly available or defined among different studies.
Other limitations of this study include the selection bias that may be present. Some centers offer EVAR only to hemodynamically stable patients. 22,24,33 In addition, many of the surgeons offering EVAR practice in tertiary care medical centers. The patients who survive the transfer to these centers may have had ruptures with inherently improved survival.
Finally, a publications bias may also be present as authors tend to disfavor publishing bad results. This publications bias, if present, would also apply to the results of open repair and therefore would not be as significant a factor when comparing the meta-analysis of open repair versus EVAR. Standard tools for assessing this, such as funnel plots and Egger regression, are not suited to application to a body of literature that does not report a treatment effect size, so we have not attempted to provide formal assessments of publication bias.
The majority of the studies we analyzed, with a few exceptions, were single- or multi-institution case series. We included a large four-state Medicare study that included mortality figures for EVAR. This study was used only in the calculation of overall mortality. Every effort was made to avoid duplication of data.
Our analysis also revealed that the experience of the center is a strong predictor of mortality. In analyzing the contribution of volume to mortality, we examined the ratio of total RAAA cases that were performed by EVAR compared with open repair. We made the assumption that EVAR is likely not applicable to 100% of patients. Therefore, we excluded six publications that did not report their concurrent open experience from this subanalysis. Centers with a higher proportion of EVAR compared with open repair showed a significant improvement in mortality. This seems to suggest that there is a learning curve for EVAR in patients with RAAA.
In reviewing the literature, we found some practice patterns among the centers performing EVAR that should be mentioned. To begin with, a specialized protocol is sometimes present. 18,22,25,32,33,35 This may expedite the mobilization of the imaging facility, operating room, ancillary staff, and surgeons. Next, some surgeons advocate elimination of routine CT in hemodynamically unstable patients. 30,32,35,41 Our analysis, however, revealed that 88.9% of patients who underwent EVAR had a preoperative CT study. In these institutions, the device is selected based on the intraoperative angiogram. Significant oversizing is sometimes tolerated when precise preoperative measurements are not available. This further reduces the delay associated with obtaining a CT scan. A policy of “hypotensive hemostasis” has been advocated by some authors. 18,22,32,33,35,39,42 Blood transfusions are withheld as long as the patient is awake and responsive. The hypotension is thought to limit the blood loss, providing the surgeons with time to exclude the aneurysm. Other operative techniques reported include selective use of proximal occlusion balloons and aortouni-iliac devices. The proximal occlusion balloon is often inflated in the supraceliac aorta to limit further blood loss while a device is being placed. 11,24,32,38,41 Use of an aortouni-iliac device can exclude the aneurysm more rapidly because it eliminates the need for cannulation of a contralateral gate. 18,21,31,33,35 In our analysis, we found that 49% of the patients received an aortouni-iliac device. We also found that some centers have liberalized the anatomic criteria for performing EVAR. Although most device manufacturers recommend a 15 mm proximal landing zone, some investigators have liberalized their anatomic inclusion criteria. 22,32,35,41 Among the complications reported after EVAR, abdominal compartment syndrome (ACS) is among the most devastating. One study found a fivefold increase in mortality in patients with ACS compared with patients without ACS. 29 Whereas some investigators have reported durable midterm outcomes of EVAR, others regard it as a bridge to elective open conversion. 25,38,39 This technique may potentially avoid the morbidity and mortality of an emergency open repair. Some investigators coined this concept “endovascular damage control.” 41
The management of patients with RAAA remains a significant challenge. Despite health care advances, the mortality for open repair remains high. The results of EVAR for RAAA seem very promising. The experience of the center appears to be a strong predictor of mortality. The corpus of literature describing EVAR for RAAA is poor, and few published studies provide interpretable comparisons of EVAR versus open repair. Randomized trials in this setting are needed.
Footnotes
Acknowledgments
Editorial assistance was provided by G. Ken Goodrick, and illustrations were provided by Chris Akers.
Presented in part at the Peripheral Vascular Surgery Society meeting, Baltimore, MD, June 8, 2007.