
Abstract
Screening for abdominal aortic aneurysm (AAA) has been suggested for older men. Our aim was to determine the effect of participant selection on prevalence and treatment suitability. Men aged 65 to 75 years attending cardiology clinics composed the high-risk group; the control group was from the community. AAA screening was performed, with follow-up or surgery arranged. Four hundred eight of 651 (62.7%) high-risk men and 109 of 908 (45.0%; p < .0001) men attended from the community. In the high-risk patients, 40 AAAs were diagnosed, with a mean diameter of 41.4 mm (± 10.4 mm). In the control group, 22 new AAAs were found, with an average size of 40.9 mm (± 10.4 mm). Higher polypharmacy existed in the high-risk group (4.6 ± 2.2 vs 2.3 ± 2.0; p < .0001). More aneurysm patients were on dual-antiplatelet therapy (32.5% vs 15.4%; p = .048) compared with the overall high-risk group. In this group, three underwent surgery; one was anatomically unsuitable for endovascular repair and medically unfit for open repair. Two in the control group had surgery. A higher prevalence of AAA is encountered in high-risk men. Most aneurysms are small; however, a significant proportion of the aneurysms detected were of a size that would warrant repair. The decision to perform surgical repair is likely to be influenced by the comorbid medical conditions, which placed the patients in the high-risk category.
The high mortality of ruptured abdominal aortic aneurysms (AAAs) and associated morbidity of survivors remains unacceptable. 1–3 Screening for AAA results in earlier detection; thus, surgical intervention can be offered when necessary. 4,5 The majority of AAA screening studies to date are population-based cohorts of older men, usually at the age of 65 years or older, with AAA prevalence rates around 5%. 6–8 Selection of screening participants could be based on age and gender, but inclusion of other risk factors could potentially increase the pick-up rate of the disease and thereby the cost-effectiveness of any larger, long-term program. It is known from large epidemiologic studies that such factors include smoking, hypertension, hypercholesterolemia, ischemic heart disease, and a family history of AAA. 9–11
Ultrasonographic screening for AAA is not known to be physically harmful. 12 However, the psychological effect of the diagnosis of an aneurysm has been investigated by a few groups. A false-positive diagnosis may lead to depression, 13 and this heightened anxiety may persist after further tests exclude any pathology. 14 The phenomenon was also investigated by the Multicentre Aneurysm Screening Study (MASS) and the Viborg and Gloucestershire trials. 6,15,16 Physical and mental scores, including anxiety levels, were assessed using validated scoring systems. Although a small difference was found in the MASS trial around the time of diagnosis, this had dissipated by 6 weeks. 6
We therefore hypothesized that a screening program targeting men attending hospital outpatient cardiovascular clinics with such disease risk factors would be more effective in disease detection than a program with participants derived from the community. However, the comorbidity of such individuals implies that surgical intervention could potentially be more hazardous, perhaps thereby mitigating the advantage obtained by better preselection. The aims of this study were to
Determine the prevalence of AAA in a high-risk group of patients Determine the extent, if any, to which the higher risk profile influenced surgery consideration Determine the impact on patients newly diagnosed with AAA
Patients and Methods
Patient Recruitment
Ethical approval was obtained from the Northern Ireland Regional Ethical Committee, and local sponsorship was provided by Belfast City Hospital Trust. The study period ran between August 2004 and August 2006. Male patients attending the consultant-led cardiology outpatient clinics aged 65 to 75 years inclusive were identified on a daily basis. These men were designated as the high-risk group owing to their increased comorbidities. A second group of similarly aged men were recruited from the community using lists provided by general practioners. Exclusion criteria included a previous diagnosis of AAA, terminal illness with a prognosis of less than 2 years, unstable angina, or recent myocardial infarction since these patients would not be suitable for surgical intervention if any aneurysms were detected.
Screening
A letter of invitation, with a patient information sheet, was sent by mail. Nonresponders received a second invitation after 2 months. Written informed consent and a short medical questionnaire of personal and family history details were obtained prior to screening. One investigator performed the scan using a 3 MHz ultrasound probe and a Sonosite 180 Plus (Sonosite Inc, Bothwell, WA) ultrasound scanner. The patients were in the supine position, and the aorta was viewed longitudinally, with a diameter of 30 mm taken as the threshold for aneurysm diagnosis. Transverse measurements were taken for enlarged aortas, and the maximum diameter was recorded. No further follow-up was arranged for patients with normal aortas. Patients with an AAA 30 to 54 mm were reviewed at the outpatient vascular clinic, whereas those with an AAA > 55 mm were admitted for assessment for surgery. A proportion of the images were stored on the Sonosite memory and reviewed by a consultant radiologist for validation.
In addition to the past medical questionnaire completed at the time of attendance for screening, each participant newly diagnosed with AAA was mailed a generic Short Form 36 (SF-36) questionnaire within 2 weeks of diagnosis. This is a validated and widely used questionnaire to assess the impact of the disease on the physical, emotional, and social aspects of the life of the patient. All participants in the screening program also reported the number and type of medications prescribed by their responsible physician. The relationship and relevance to AAA prevalence and surgery were assessed as this would reflect on the degree to which the high-risk group was indeed high risk.
Statistical Analysis
Analysis was performed using SPSS version 13 (SPSS Inc, Chicago, IL). Age was calculated as mean and standard deviation. Attendance and prevalence were expressed as a percentage. Chi-square test was used for comparison between groups. A p value < .05 was considered statistically significant for each test.
Results
Recruitment and Attendance
Six hundred fifty-one male patients attending six consultant-led cardiology clinics at Belfast City Hospital from August 2004 to February 2006 received an invitation to be screened for AAA. This was defined as the high-risk group since these patients had a higher incidence of comorbidities. In the community-based control group, 908 patients were invited for screening in the same time period.
After the two invitations, 408 high-risk patients attended for screening, whereas the remaining 243 of the group either did not respond, refused, or did not attend their arranged appointment. In contrast, 409 of the control group attended for screening (62.7% vs 45.0%; p < .0001).
Medical Details
The men in the high-risk cohort had a mean body mass index (BMI) of 26.6 kg/m 2 (± 4.7 kg/m 2 ) and only 29 were current smokers. One hundred forty-eight were lifelong nonsmokers, whereas the rest were former smokers. The majority of this group, as expected, had a history of either ischemic heart disease, previous myocardial infarction, or hypertension, necessitating attendance at the cardiac clinic. The prevalence of clinical characteristics and family history are summarized in Figure 1.
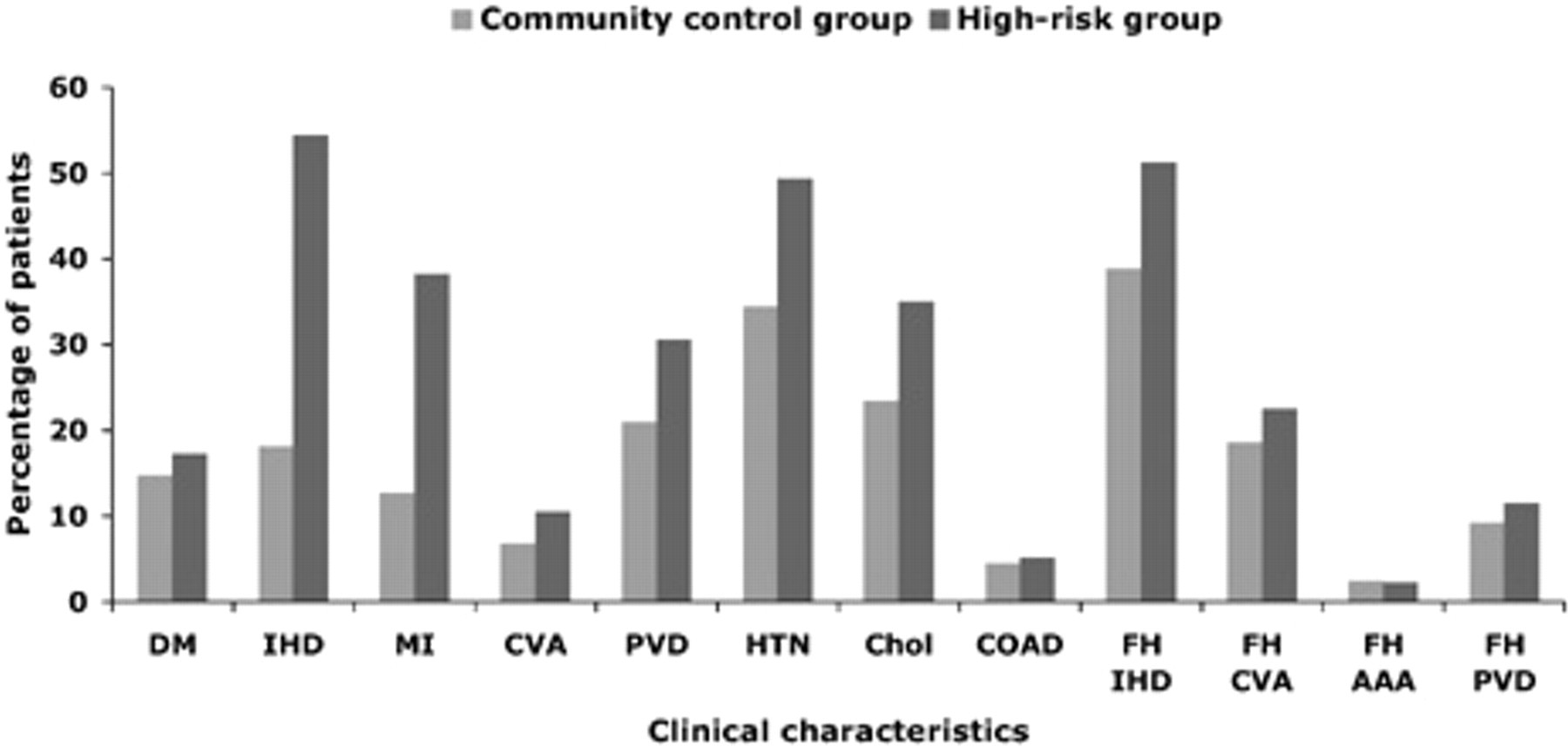
Distribution of clinical characteristics in screened men. Chol = hypercholesterolemia (p < .0001); COAD = chronic obstructive airways disease (p = .88); CVA = cerebrovascular accident (p = .053); DM = diabetes mellitus (p = .009); FH AAA = family history of abdominal aortic aneurysm (p = .95); FH CVA = family history of cerebrovascular accident (p = .038); FH IHD = family history of ischemic heart disease (p < .0001); FH PVD = family history of peripheral vascular disease (p = .0002); HTN = hypertension (p < .0001); IHD = ischemic heart disease (p < .0001); MI = myocardial infarction (p < .0001); PVD = peripheral vascular disease (p < .0001).
In the community control group, the average BMI was 27.3 kg/m 2 (± 4.0 kg/m 2 ) and 44.1% were nonsmokers. Less than half (48.6%) were ex-smokers, and the rest were currently smoking. As expected, there were much fewer men with either ischemic heart disease or previous myocardial infarction. Other clinical characteristics were decreased in this group (see Figure 1). As demonstrated in Figure 1, most of the relevant clinical characteristics were significantly increased in the high-risk group.
AAA Detected
In the high-risk group, 40 new diagnoses of AAA were made, resulting in a prevalence of 9.85%. The mean size of AAA was 41.4 mm (± 10.4 mm). The majority was less than 55 mm, but four (10%) men were admitted for surgical assessment with aortic diameters of 58, 65, 66, and 75 mm. There was a positive skew in the distribution of AAA sizes, with 37.5% measuring between 30 and 35 mm and 25% between 36 and 40 mm. Ten percent were large enough to consider surgery, whereas 27.5% were between 40 and 54 mm.
The control group yielded 22 new AAAs, representing a lower prevalence of 5.4% (p = .02). The mean size was 40.9 mm (± 10.4 mm), with only two (9.1%) requiring surgical consideration, at 56 and 75 mm. The skew of sizes was also seen in the community-sourced men, with 40.9% between 30 and 35 mm and 18.2% between 35 and 40 mm. Of the remaining, 31.8% were 40 to 54 mm.
Prescribed Medications
There was a high degree of polypharmacy in the high-risk group of men, with a mean of 4.6 (± 2.2) medications, ranging from none to 10 (Figure 2). One hundred three men (25.2%) were on long-term warfarin therapy, whereas 63 (15.4%) were on dual aspirin-clopidogrel treatment. The polypharmacy of the control group was lower at 2.3 (± 2.0) tablets per day (p < .0001), with a very different pattern of distribution (see Figure 2). The use of anticoagulation was reduced at 5.5% (p < .0001), and only 2.1% (p < .0001) used dual-antiplatelet therapy.
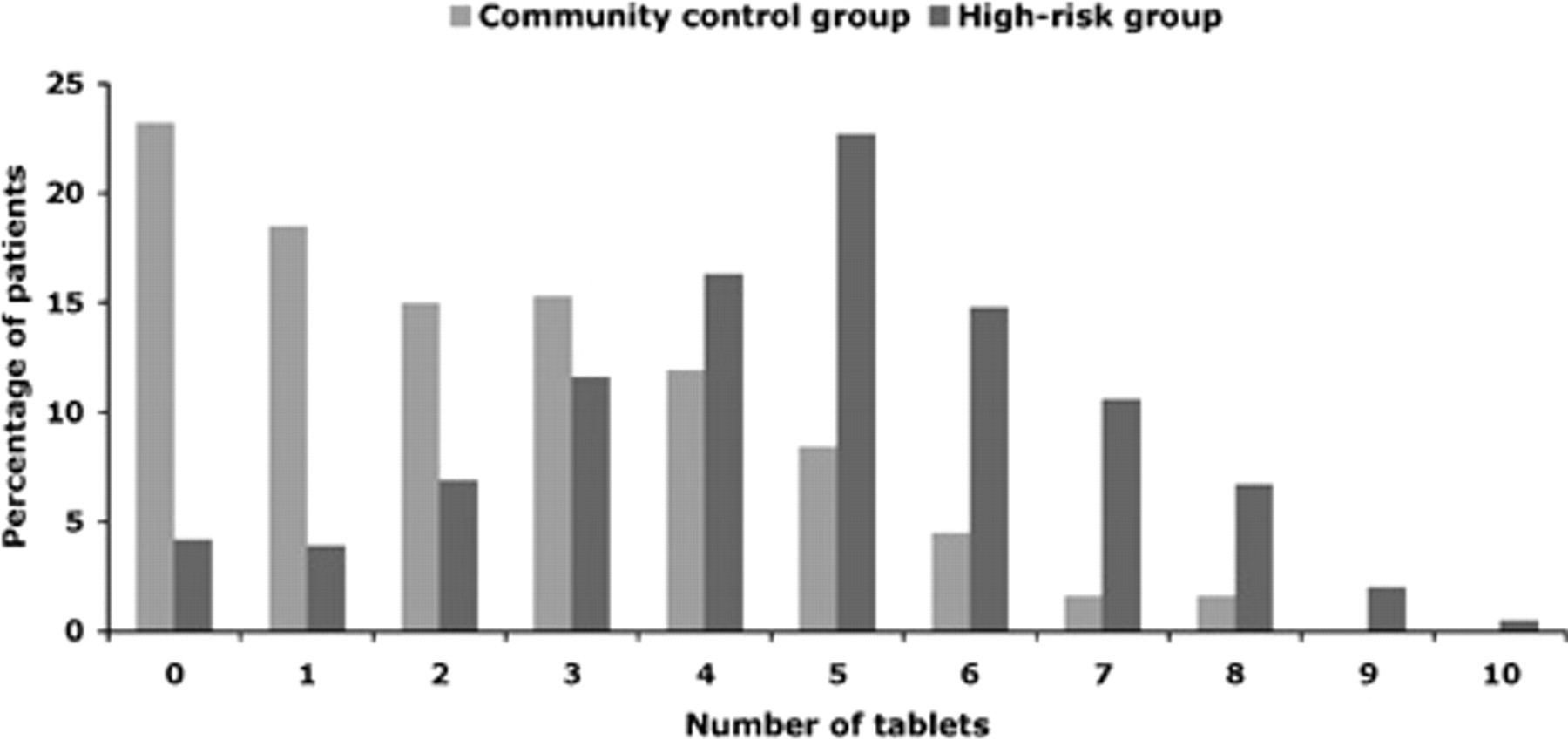
The distribution of prescribed medications across the groups.
The average number of medications in those patients, within the high-risk group, requiring surgery was 4.9 (± 2.0). Interestingly, a slightly higher proportion of aneurysm patients (30%; p = .75) were on long-term warfarin compared with the whole high-risk group, and twice the proportion of patients (32.5%; p = .048) were on dual aspirin-clopidogrel treatment, with obvious implications for surgical intervention.
Follow-Up
In the control group, one patient underwent endovascular repair and one had open repair successfully performed. No complications were encountered in this group. In the high-risk group, one man underwent endovascular repair of his aneurysm, which was successful, although his discharge was delayed owing to a groin infection. Two other men underwent open repair without complication. One man with a 65 mm AAA was assessed for surgery and was found to be anatomically unsuitable for endovascular aneurysm repair. He also had significant congestive heart failure, with a left ventricular ejection fraction of less than 20%. Following discussion with the responsible surgical and anesthetic staff, the patient declined surgical intervention owing to the high risk of mortality. Another patient was reviewed at the outpatient clinic within 6 months of diagnosis, and repeat aortic scanning revealed growth to over the surgical threshold. He successfully underwent open repair.
SF-36 Quality of Life
No significant difference was found between the groups for any of the recorded parameters (Table 1). This was in spite of the obvious contamination of general health problems in aneurysm-related questions, particularly in the high-risk group, as indicated by the responses and additional annotations on the questionnaire.
Short Form 36 Quality of Life Questionnaire Results
Discussion
The long-term success of any screening program is determined by appropriate inclusion criteria and the reduction in disease-related morbidity and death. The selection of patients is usually targeted by gender and age, although the use of risk factors would narrow this further. Hypercholesterolemia, smoking, and hypertension in middle age have been shown to relate to AAA risk in those surviving into older age. 17 These are also the risk factors in other cardiovascular diseases; consequently, comorbidities are increased in such patients. Kanagasabay and colleagues demonstrated a positive association between AAA and both intermittent claudication and myocardial infarction, although an association with angina was borderline. 18 An association with cerebrovascular disease was found in females, whereas diabetes mellitus and respiratory disease were not positive risk factors.
Our results show that a higher AAA prevalence exists in patients attending hospital cardiology clinics, at approximately twice the prevalence of similar men in a general population–derived control group. Similar findings have been reported when a modified abdominal examination protocol is used during echocardiography, with up to 13.4% AAA incidence in older hypertensive males, using the subcostal window or abdominal position. 19–21 The cardiac subgroup of those diagnosed with coronary artery aneurysm has been shown to yield an even higher prevalence of AAA, of approximately 20%. 22,23 This is of similar pathogenesis, with shared genetic candidate genes implicated. Patients with coronary artery aneurysm would be a suitable target population, although the abdominal aorta is visualized on less than 5% of angiograms. 24,25 Another interesting aspect of cardiac patients is that there may a contribution toward the aneurysmal degeneration from their antihypertensive medication. Wilmink and colleagues showed that calcium channel blockers were an independent risk factor for AAA, with increased wall stiffness. 26 However, angiotensin-converting enzyme inhibitors were associated with greater collagen turnover and decreased wall stiffness.
Although the advantage of screening high-risk patients is the higher prevalence, there are certain drawbacks to this approach. In our results, one of four men with an aneurysm greater that 55 mm was not medically suitable for repair. In addition, another patient had a prolonged hospital stay owing to groin infection, possibly complicated by his warfarin therapy. It was previously demonstrated that 27% of AAA patients have significant coronary artery disease, with almost 5% requiring coronary artery bypass graft surgery prior to aneurysm repair. 27 Others found a 40 to 60% incidence of coronary artery disease in AAA patients. 28–31 A large longitudinal cohort study reported a higher total mortality and cardiovascular mortality in AAA patients, independent of age, sex, or other cardiovascular disease. 32 Therefore, those recruited from cardiac clinics and diagnosed with AAA will, by nature, be very high-risk patients for surgery. The skew of the AAA sizes toward predominantly small aneurysms may result in a diagnosis, although the AAA may not have time to progress to life-threatening, particularly in high-risk patients with other major comorbidities. Therefore, on balance, caution is advised to avoid selecting patients who cannot undergo corrective surgery. However, a long-term follow-up comparative study would be required to ascertain if this is so.
Footnotes
Acknowledgments
We would like to thank the general practitioners of Belfast, Lisburn, and Saintfield and the cardiologists of Belfast City Hospital for their support and supply of patient details.
The vascular unit received an educational grant from Medtronic Inc.