
Abstract
The role of matrix metalloproteinases (MMPs) in abdominal aortic aneurysm (AAA) pathogenesis is well described. However, a clear role for the MMPs in disease prediction has not been established. The aim of this study was to determine if circulating levels of MMPs correlated with AAA diameter and with MMP concentrations within the aneurysm wall. Preoperative plasma samples and intraoperative infrarenal AAA sac biopsies were taken in a standard fashion from 31 patients undergoing elective repair. The concentrations of MMP-1, MMP-2, MMP-3, MMP-9, tissue inhibitor of matrix metalloproteinase (TIMP)-1, and TIMP-2 were quantified in plasma and aneurysm wall homogenates using enzyme-linked immunosorbent assay. Comparison used the Spearman correlation. There were no correlations between the paired plasma and aneurysm wall concentrations for any MMP or TIMP. Correlation between MMP-9 levels in the aneurysm wall and aneurysm diameter was negative (r = −.42, p = .019). Other correlations between plasma and tissue levels with aneurysm diameter were nonsignificant.
Keywords
The principal factor determining the suitability of an abdominal aortic aneurysm (AAA) for repair is maximum transverse diameter. The UK Small Aneurysm Trial determined that aneurysms less than 5.5 cm in diameter did not benefit from open repair. Ultimately, two-thirds of small aneurysms initially managed nonoperatively continued to expand and progressed to open operative repair over the active course of the trial. 1 Aneurysm diameter and expansion rates represent complete determinants of disease activity; however, the search for other markers of disease activity, particularly biologic activity, continues. The biologic determinants of aneurysm formation have been extensively investigated. The formation of an AAA is characterized by the degradation of aortic elastin and collagen through the overexpression of native matrix metalloproteinases (MMPs). 2,3
The circulating levels of various MMPs have been reported to predict the natural history of small aneurysms. 4 Indeed, falling circulatory levels of MMPs may indicate successful aneurysm exclusion after endovascular repair, whereas persistently high levels may indicate the presence of an endoleak. 5 The ability of circulating MMP levels to reflect tissue MMP levels of the AAA, thus acting as a surrogate for biologic activity, has not been determined.
This study quantified levels of MMPs and their endogenous inhibitors (tissue inhibitors of matrix metalloproteinases [TIMPs]) in matched plasma and tissue samples from patients undergoing open AAA repair. The primary objective of this study was to observe a correlation between paired circulating and aneurysm tissue MMP and TIMP concentrations. The secondary objectives were the determination of correlations for circulating and tissue MMP and TIMP levels with respect to AAA diameter.
Methods
Patient Selection
Thirty-one patients undergoing elective open AAA repair were recruited. The cross-sectional diameter of each aneurysm was measured from the most recent preoperative computed tomogram. Consent was obtained in accordance with guidelines from the local research ethics committee.
Patient demographic information included age, gender, the presence of a cardiovascular event (documented myocardial infarction, cerebrovascular or peripheral vascular disease, angina requiring medication), hypertension (requiring medication), smoking history (current or ex-smoker of less than 10 years versus nonsmoker or ex-smoker of greater than 10 years), and diabetes (requiring medication or dietary modification). Cardiovascular medication was also recorded (statin, β-blocker, calcium channel blocker, acetylcholinesterase inhibitor, and aspirin).
Sample Collection
Blood samples were obtained immediately preoperatively by venipuncture to tubes containing sodium ethylenediaminetetraacetic acid. Separation of cellular and plasma components was achieved with centrifugation (3,000g for 20 minutes), and the plasma was decanted and stored at −80°C. Aneurysm tissue samples were obtained intraoperatively in a standard fashion at the point of maximal diameter and stored at −80°C prior to processing.
MMP Quantification
Protein extracts of MMPs and TIMPs were prepared from the aneurysm wall biopsies according to an established method. 6,7 The levels of MMP-1, MMP-2, MMP-3, MMP-9, TIMP-1, and TIMP-2 in each plasma and aneurysm wall extract were quantified in duplicate by enzyme-linked immunosorbent assay (ELISA) (Amersham Pharmacia Biotech, Buckinghamshire, UK). The study used conventional sandwich ELISA and measured total levels of target enzyme. TIMP-1 assay measured total TIMP-1, including that bound within TIMP-MMP complexes. The TIMP-2 assay recognized free TIMP-2 and that complexed to active forms of MMPs. All samples were run in duplicate, and an average was obtained. The MMP and TIMP concentration in the AAA wall biopsy was expressed as nanograms of target enzyme per milligram of protein extract. The MMP and TIMP concentration of each plasma sample was expressed as nanograms of target enzyme per milliliter of plasma.
Statistical Analysis
Statistical analysis used GraphPad Prism 5 (GraphPad Software, California, USA). Data were nonparametrically distributed, and the Spearman rank test was used to test correlations. Statistical significance was assumed at the p < .02 level.
Results
Patient Demographics
The clinical features of the AAA patient cohorts are described in Table 1.
Demographics, Comorbidity, and Medications for 31 Abdominal Aortic Aneurysm Patients
AAA = abdominal aortic aneurysm; ACE = angiotensin-converting enzyme.
AAA Tissue and Plasma MMP and TIMP Levels: Correlation between Paired Samples
Table 2 details MMP and TIMP concentrations in the paired plasma and AAA tissue biopsies. There were no correlations between plasma and AAA tissue values for any MMP or TIMP examined.
Correlation of MMP and TIMP Concentrations between Paired Plasma and Abdominal Aortic Aneurysm Tissue Samples
MMP = matrix metalloproteinase; TIMP = tissue inhibitor of matrix metalloproteinase.
Data are presented as median and interquartile range; the statistics used were Spearman correlation coefficient and 95% confidence limits; p < .02.
AAA Tissue and Plasma MMP and TIMP Levels: Correlation with Aneurysm Diameter
Table 3 shows AAA tissue biopsy concentrations of MMPs and TIMPs correlated against AAA diameter. Within AAA tissue biopsies, a negative correlation between MMP-9 levels and AAA diameter was observed (r = −.42, p = .019; Figure 1). No other significant correlations were observed for MMP or TIMP tissue concentrations against AAA diameter. Furthermore, there were no significant correlations for plasma MMP or TIMP values versus AAA diameter.
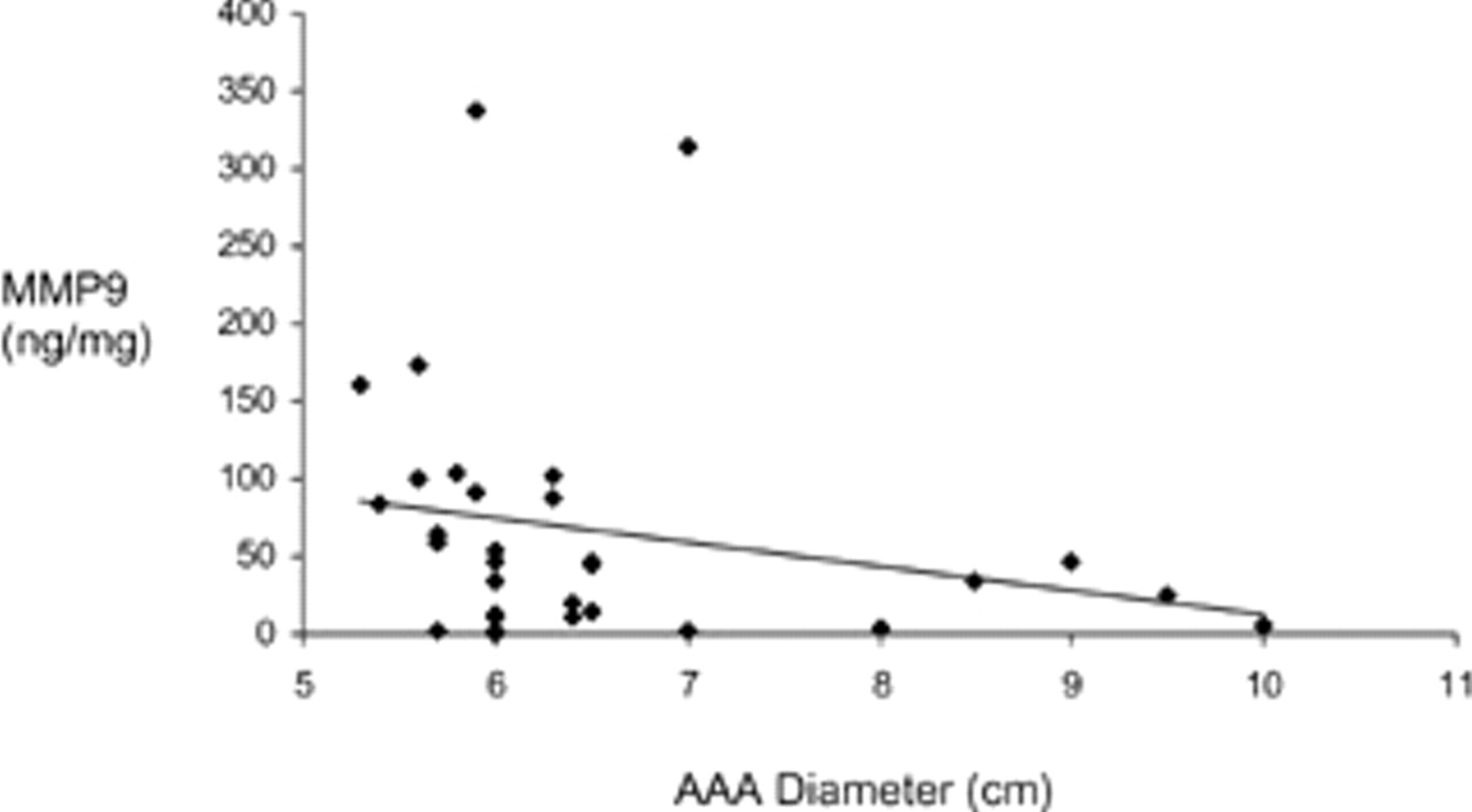
Correlation between abdominal aortic aneurysm (AAA) tissue matrix metalloproteinase 9 (MMP-9) and AAA diameter (Spearman correlation r = −.42, p = .019).
Correlation of Plasma and AAA Tissue MMP and TIMP Concentrations with AAA Diameter
AAA = abdominal aortic aneurysm; MMP = matrix metalloproteinase; TIMP = tissue inhibitor of matrix metalloproteinase.
Data are presented as median and interquartile range; the statistics used Spearman correlation coefficient with 95% confidence limits; *p < .02.
Discussion
The structural integrity of the aorta is dependent on elastin and the fibrillar collagens. 8 Dobrin's in vitro model suggests that loss of elastin is responsible for early aortic expansion, whereas late expansion and rupture are modulated by collagen breakdown. 8 The principal group of endogenous proteases implicated in aneurysm biology are the MMPs, and their elevation within aneurysmal aortic tissue is well documented. 2,3 The critical role of MMP-9, MMP-2, and TIMP-1 in the aneurysm process is demonstrated by gene knockout and transfection studies. 9–11 Less is known about the changes in circulating MMPs with the presence of an aneurysm, although a few reports discuss the association between circulating MMPs and aortic tissue concentrations.
The principal objective of this study was the determination of plasma MMP and TIMP levels relative to aortic tissue levels within an aneurysmal cohort. Hovsepian and colleagues suggested an exponential relationship for MMP-9 between plasma and tissue in four patients' samples. 12 We failed to demonstrate any significant associations between plasma and tissue enzyme levels within our patient cohort of 31 patients. This suggests that plasma levels of MMPs do not reflect MMP tissue levels within aneurysms greater than 5.3 cm in diameter.
The secondary objectives of this study were to correlate plasma and tissue MMP and TIMP levels with aneurysm diameter. We failed to demonstrate significant correlations between enzyme levels and aneurysm diameter greater than 5.3 cm. By contrast, Lindholt and colleagues demonstrated the direct correlation of plasma MMP-9 with aneurysm diameter in a cohort of smaller aneurysms (3–5 cm). 4 The difference between their observations and our own may be due to the disparity in aneurysm diameter between the two studies and indicates that the comparison of plasma MMP levels in small versus larger aneurysms is justified.
Levels of tissue MMP-9 protein correlated negatively with aneurysm diameter, whereas other enzyme levels showed no association. The negative correlation between MMP-9 and vessel diameter has been described at transcription and posttranscription levels. McMillan and colleagues demonstrated significantly higher expression of MMP-9 messenger ribonucleic acid in medium-sized aneurysms (diameter 5–6.9 cm) when compared with larger aneurysms (p = .01). 13 Peterson and colleagues observed an inverse correlation between tissue MMP-9 protein levels and aneurysm diameter with a low coefficient of correlation (p = .04, r = −.31), 14,15 whereas MMP-2 levels did not correlate with aneurysm size. 15 Several hypotheses are reported to support the case for a decrease in MMP-9 in larger aneurysms at transcription and posttranscription levels. First, given that elastin loss is considered an early event in aneurysm formation, a decrease in elastin substrate may result in the failure of positive feedback required to maintain tissue MMP-9 levels. 13 Alternatively, a negative correlation between tissue MMP-9 levels and aneurysm diameter may be the result of aneurysms with lower MMP-9 levels remaining unruptured and simply expanding, whereas aneurysms with higher MMP-9 levels may rupture earlier at a smaller diameter. 15
The results of this study were interpreted in the context of the study's design limitations. First, we recognize that the extraction technique may not be complete and that proteases may degrade directly under the action of other enzymes or as a result of the extraction process. 16,17 Further, we acknowledge that the tissue homogenate from a single biopsy may not represent the whole aneurysm wall. The aneurysm wall is a heterogeneous entity, consisting of many cell types. Separating the cell types is possible; however, the objective of this study was to assess global MMP levels as a marker of disease activity rather than the delineation of cellular activity and expression. The study was restricted to aneurysms with a diameter of 5.3 cm and greater undergoing open repair. It is entirely possible that the diameter range was too limited, and the inclusion of aneurysms less than 5.3 cm may be useful and represents future work.
In conclusion, care must be exercised when interpreting the significance of plasma MMPs as a predictor of aneurysm wall activity. Plasma levels do not predict tissue expression of MMPs in aneurysms that require operative repair. The correlation of circulating MMP levels with aneurysm diameter is variable, and a clear pattern has not been established. The longitudinal observation of plasma MMP levels in smaller aneurysms may be justified.