
Abstract
A 45-year-old male presented with increasing hoarseness and swelling of his right neck over 5 months. He was noted to have right vocal cord paralysis and hemiatrophy of his tongue. He was found to have a schwannoma of the vagus nerve with compression of the right hypoglossal nerve. One month after his surgery, the patient's tongue mobility was improving, he was not aspirating, his voice was better and his right vocal cord remained abducted. A discussion of this case is followed by a review of the literature surrounding this rare disease and this unique presentation.
Vascular surgeons are often referred patients with a neck mass for work-up and treatment. Included in the differential diagnosis of the neck mass is a potpourri of conditions that may mimic a carotid body tumor. We present the case of a schwannoma of the vagus nerve masquerading as a carotid body tumor. To our knowledge, this case is unique in that this large tumor arising from the vagus nerve was responsible for the dysfunction of the hypoglossal nerve.
Case Report
A 45-year-old male presented to the emergency room with 5 months of increasing hoarseness and right neck swelling, rightward tongue deviation, dysphagia, and unintentional weight loss. He denied right upper extremity numbness or other neurologic changes. Physical examination revealed right tongue hemiatrophy (Figure 1), hoarseness, a palpable right neck mass, and right supraclavicular muscle atrophy. A computed tomographic (CT) scan of the head demonstrated a right parapharyngeal mass lesion that was 3 × 3 cm, elliptical, smooth-walled, and nonenhancing (Figure 2). The mass was between the internal carotid artery (ICA) and the external carotid artery at the bifurcation and was displacing the ICA medially. This led to the working diagnosis of a carotid body tumor versus schwannoma. Magnetic resonance imaging (MRI) revealed a contrast-enhancing mass approximately 2.9 × 3.1 × 5.7 cm within the right carotid canal extending just distal to the jugular foramen to the level of the epiglottis.

Hemiatrophy of the tongue ipsilateral to the neck mass.
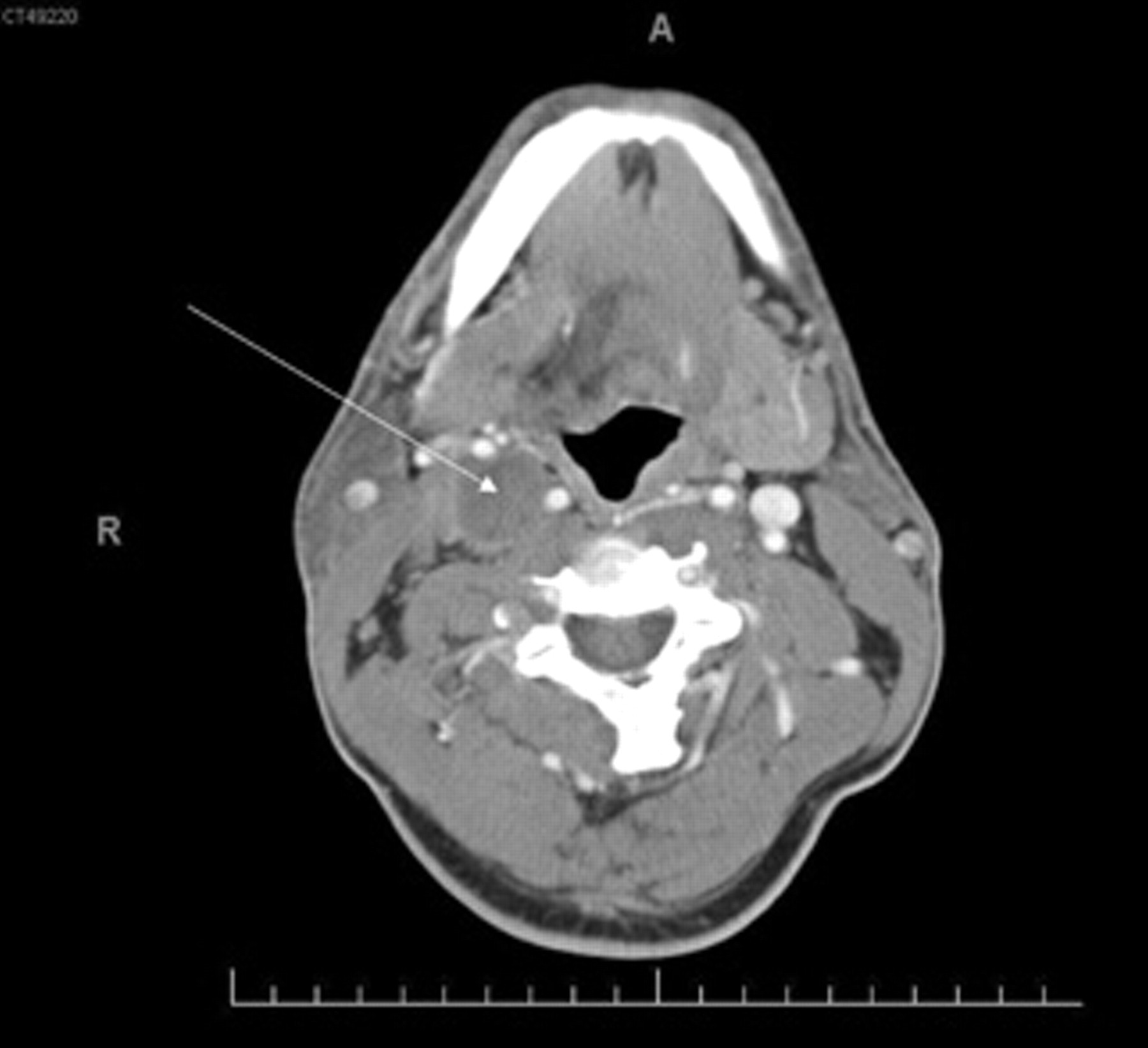
Computed tomographic scan of the head. The arrow indicates the presence of a neck mass.
Several weeks later, resection revealed the tumor to be posterolateral to the carotid bifurcation, appearing to arise from the vagus nerve (Figure 3). The hypoglossal nerve was severely compressed, the etiology for the patient's right tongue hemiatrophy. During the operation, the vagus nerve was ligated and the hypoglossal nerve was preserved. The mass was well encapsulated but could not be delivered en bloc as the cephalad aspect of the mass extended to the base of the skull and could not be freed during dissection. The capsule was incised, aspirated, and debulked by approximately 90%, leaving behind the cephaladmost portion after electrocoagulation. The intraoperative frozen section suggested the mass to be a benign schwannoma with spindle cells. The final pathology reported a benign nerve sheath tumor with positive staining for S-100. The patient was discharged the following morning with improved swallowing and tongue deviation. Repeat indirect laryngoscopy 4 weeks later showed that the right vocal cord continued to be fixed in abduction. Tongue function and mobility had improved. There were no clinical signs of aspiration, his voice quality had improved, and the wound was well healed.

Resection of the tumor. The arrow indicates the mass arising from the vagus nerve.
Discussion
Patients with cervical neck masses near the carotid bifurcation are often referred to the vascular surgeon. Carotid body tumors, or paragangliomas, are the most common masses near the carotid bifurcation. Cervical sympathetic chain schwannomas are rare neurogenic tumors that can be mistaken for carotid body tumors. When evaluating a lateral neck mass, the differential diagnosis includes salivary gland tumors, neurogenic tumors, lymphatic masses, vascular tumors, vascular malformations, thyroid masses, lipomas, and branchial cleft cysts.
The parapharyngeal space is divided by the styloid process into anterior and posterior compartments. The posterior parapharyngeal space contains the internal and external carotid arteries, internal jugular vein, glossopharyngeal nerve, vagus nerve, spinal accessory nerve, hypoglossal nerve, and the cervical sympathetic chain. On CT, splaying of the carotid bifurcation with hypervascularity usually indicates a carotid body tumor. Without hypervascularity, carotid bifurcation splaying may suggest a cervical sympathetic chain schwannoma. Separation of the internal jugular vein and the ICA without widening of the carotid bifurcation may indicate a vagus nerve schwannoma. 1–4
Carotid body tumors usually present as a painless neck mass at the angle of the mandible, and they can be pulsatile owing to their carotid artery juxtaposition. Rarely, patients demonstrate neurologic abnormalities caused by vagal or hypoglossal nerve involvement, and even more rarely, patients can present with Horner syndrome. 5 In contrast, schwannomas, or “neurilemmomas,” are benign tumors of neurogenic origin. Schwann cells form the inner layer of the nerve sheath and are thought to be the cells of origin. Schwannomas may arise in all cranial nerves, except in the optic and olfactory nerves, as these do not contain Schwann cells. They account for only 5% of benign soft tissue tumors. Approximately 45% of schwannomas occur in the head or neck and can occur at any age, but most commonly occur between the ages of 20 and 50 years. 6,7
Schwannomas of the neck are usually lateral and present as a solitary slowly growing painless neck mass. Pain is more commonly associated with larger tumors. They can arise anywhere from the skull base to the thoracic inlet but most commonly are found in the midneck. Schwannomas are usually classified according to the nerve involved and the site of origin within the head and neck. In the neck, schwannomas may arise in the poststyloid compartment and frequently displace the ICA anteriorly and laterally. Most believe that encapsulated schwannomas are completely benign and do not undergo malignant transformation. Therefore, when excising, if possible, the nerve should be left intact. 6,7 We felt it necessary intraoperatively to sacrifice the involved nerve to excise the tumor, but, interestingly, no postoperative deficits were appreciated.
Schwannomas are generally avascular, whereas carotid body tumors tend to be vascular. Contrast-enhanced CT or MRI is essential for diagnosis. On MRI, schwannomas are generally hypointense on T1-weighted images, depending on cellularity. The T2 relaxation time diminishes with increasing cellularity. Gadolinium administration results in marked enhancement of the solid component of the tumor. Some schwannomas are hypervascular, and paragangliomas should be considered in the differential diagnosis. 8 Schwannomas usually have a strong affinity for S-100, which may aid in diagnosis. Angiography may be helpful to evaluate blood supply and embolize vessels as needed. 9 Based on relatively extensive prior experience, the vascular surgeon in our case felt that this step was unnecessary.
A mediastinal vagus nerve schwannoma can present with increasing hoarseness. 10 Katz and colleagues summarized 15 cases of neurogenic neoplasms of the face and neck, with one vagal schwannoma presenting as hoarseness. 11 Another tumor presented as vocal cord paralysis and was found to be a vagal chemodectoma. Biswas and colleagues found in a 10-year review that in the neck 77% of schwannomas present as an asymptomatic isolated neck mass. 6 Preoperatively, they were able to identify the nerve of origin in 47% of the cases. Two of 14 originated from the vagus, 1 from the hypoglossal nerve, and 1 from the sympathetic chain.
Hallett and colleagues reported on 153 carotid body and cervical paragangliomas in a 50-year period. 12 They found an improvement in the perioperative stroke rate and perioperative mortality and no change in postoperative cranial nerve dysfunction, which was permanent in 48%. They identified 139 carotid body, 11 vagus, and 3 glomus jugulare paragangliomas. The mean patient age was 52 years. Local recurrence affected 5% of patients, and metastatic disease was found in 1.7%. The authors removed 89% of the tumors completely but did not specify if recurrence occurred in the partially resected tumors. 12 Pesavento and colleagues found 74 cases of schwannoma of the cervical vagus nerve in their review of the literature. 13 During the surgery they performed, excision of the vagus nerve was required along with the schwannoma, as in our case. Postoperative complications of vagal schwannoma resection include Horner syndrome and vocal cord paralysis as often the nerve from which the schwannoma originated cannot be preserved. 14,15
Lee and colleagues presented a case of an intracranial hypoglossal nerve schwannoma causing tongue hemiatrophy and concluded that theirs was the seventieth case of a hypoglossal neurinoma in Medline. 16 Sato and colleagues presented transcervical removal of a hypoglossal schwannoma as well. 17 To our knowledge, ours is the first case report of a vagal schwannoma causing hypoglossal nerve compromise and presenting as a growing neck mass with dysphonia, dysphagia, and hemiatrophy of the tongue.