
Abstract
A woman aged 75 years developed chylous ascites day 5 after emergency abdominal aortic aneurysm repair. She was still on artificial ventilation at the time of diagnosis. The first symptoms were high ventilation pressure, an elevated diaphragm, and abdominal distention. The patient was treated conservatively with drainage and total parenteral nutrition and given tube feeding without long-chain triglycerides. Unfortunately, the patient died of sepsis on day 25. Chylous ascites is an unusual complication of retroperitoneal surgery. Abdominal paracentesis is a simple means to confirm the diagnosis. Initial treatment consists of draining the chylus and a medium-chain triglyceride diet or total parenteral nutrition. When this fails, more invasive treatment is required, consisting of direct lymphatic repair or peritoneovenous shunting. In mechanically ventilated patients, gradually progressive symptoms of abdominal hypertension after surgery in the retroperitoneal space should arouse suspicion of this complication.
Keywords
Postoperative chylous ascites is a rare complication of retroperitoneal surgery caused by the unrecognized interruption of major retroperitoneal lymphatic channels and establishment of a lymphoperitoneal fistula (< 1%). 1 Lymphatic complications are very uncommon after elective or emergency aortic surgery. However, when they occur, treatment can be very challenging. Patients with low performance status owing to the primary operation are further debilitated by the serious mechanical, nutritional, and immunologic consequences of the constant loss of protein and lymphocytes. We report a case of chylous ascites following emergency aortic surgery and discuss the treatment options.
Case Report
A 75-year-old woman presented with a ruptured abdominal aortic aneurysm and underwent repair with a tube graft (22F polytetrafluoroethylene). She had multiple medical comorbidities, including chronic obstructive airway disease, ischemic heart disease, and diabetes mellitus. At operation, a ruptured juxtarenal aneurysm was identified, as well as associated complex renal vein anatomy on the left side. This consisted of duplicate left gonadal veins, which drained into the left renal vein. Two or three of these branches required ligation before the neck of the aneurysm could be dissected and controlled. No chyle was seen at the end of the operation. On the fifth postoperative day, while still on artificial ventilation, she was noted to have a white cell count of 21.6 cells/μL, which had doubled (9.6) from 2 days previously (normal range 4.0–10.0 cells/μL). In addition, there was an increase in ventilation pressures (peak end-expiratory pressure 10–18 cm H2O), an elevated diaphragm on a chest radiograph, and abdominal distention. Intra-abdominal pressures were checked and ranged between 15 and 22 mm Hg. She had no pyrexia. She was started empirically on intravenous cefuroxime and metronidazole. Computed tomography revealed fluid collection around the aorta and the graft (Figure 1). The collection was drained percutaneously (7.1F polyethylene pigtail catheter, Cook, Cook Ltd, Brisbane, Australia), and specimens were sent for culture and analysis. The fluid was initially milky, cloudy, and blood stained and drained approximately 750 mL per day. The concentration of triglycerides in the fluid was > 55 mmol/L, and cholesterol was 5 mmol/L. Laboratory serum analyses showed normal levels. The patient was commenced on total parenteral nutrition (TPN) and following reduction in the drainage to < 50 mL/d was commenced on nasogastric feeding without long-chain triglycerides on day 18. Drainage subsequently stopped 4 days later. Unfortunately, she later developed pneumonia with associated acute respiratory failure and died on postoperative day 25.
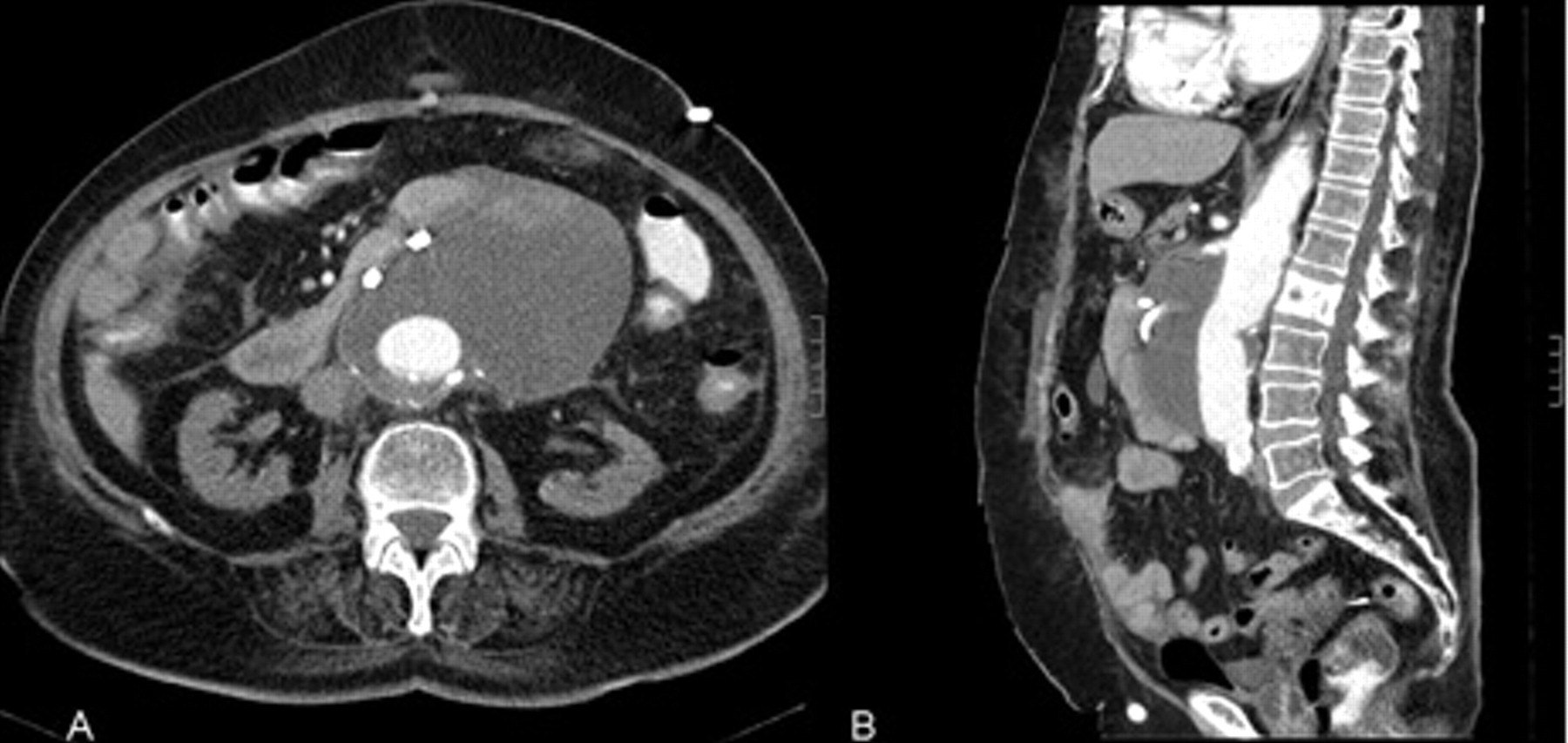
A, Contrast-enhanced abdominal computed tomographic axial image (5 mm slice thickness) showing the perigraft fluid collection with low-attenuation (Hounsfield unit [HU] 15) and high-attenuation (HU 55) components. A general purpose pigtail catheter is situated within the anterior portion of the collection. B, This image demonstrates the same collection showing its extent in the sagittal plane.
Discussion
Chylous ascites may be the result of many pathologic conditions, including congenital defects of the lymphatic system; nonspecific bacterial, parasitic, and tuberculous peritoneal infection; liver cirrhosis; malignant neoplasm; blunt abdominal trauma; and surgical injury. The most common etiologic factors are abdominal malignancy and congenital lymphatic abnormalities in adults and children, respectively. Postoperative chylous ascites is a rare condition that usually develops as a result of operative trauma to the thoracic duct, cisterna chyli, or their major tributaries 2 in combination with increased chyle production and obstruction of lymphatic drainage from the abdomen. 3
Various vascular surgical procedures, including aortic aneurysm repair, aortofemoral bypass, 3 and resection and replacement of the inferior vena cava, as part of surgery to remove malignant tumors may cause chylous complications. 4 However, chylous ascites comprises less than 1% of all complications after vascular surgery of the abdominal aorta 5 and is relatively rare in view of the large numbers of aortic reconstructions performed worldwide. 3 Chylous ascites is more prevalent after emergency surgery for a ruptured abdominal aortic aneurysm 6,7 and after resection of inflammatory aortic aneurysms than after elective aortic reconstruction. 5,8 Resection of inflammatory aortic aneurysms carries a particularly high risk of chylous complications owing to the extensive and difficult dissection involved in this type of surgery. Furthermore, ruptured abnormal retroperitoneal lymphatic vessels are involved in the pathogenesis of inflammatory aneurysms and, hence, further increase the risk of lymphoperitoneal fistula. 8
Chylous ascites usually presents with persistent abdominal distention. The time frame of postoperative ascites development varies from several days to several months after surgery. 1,3,9 The presentation is insidious, with gradual accumulation of fluid and an increase in abdominal girth. As the abdominal distention progresses, dyspnea, nausea, and vague abdominal pain associated with paralytic ileus may occur. Hypovolemia from continued fluid loss may be compounded by hypoproteinemia, which results in transcapillary fluid shifts. During prolonged chyle loss, the body's reserves of protein, fats, vitamins, and electrolytes are depleted. 10 The diagnosis is confirmed by paracentesis, which reveals milky, lipemic fluid, rich in triglycerides. 11 This is usually found to be sterile.
Currently, four therapeutic options are recognized: an oral diet with medium-chain triglycerides, TPN, venoperitoneal shunting, and exploratory laparotomy with direct ligation. 11 Limiting dietary intake of long-chain triglycerides and supplementing the diet with medium-chain triglycerides should theoretically decrease the lymphatic flow. In practice, dietary manipulation is not effective on its own. 12 TPN is effective in providing nutrition in patients with traumatic chylous ascites, and with time, the chylous peritoneal fistula usually heals. 13 It is associated with prolonged hospitalization, is expensive, and carries a risk of infection. 14 The resolution rate of chyloperitoneum by conservative management is about 50 to 60%. 15
Surgery is usually considered after failure of conservative treatment. The role and timing for surgical repair, however, remain controversial. The main argument in favor of early reintervention is that it permits direct visualization of the fistula and its ligation with immediate definitive cessation of the leak, avoiding nutritional and immunologic complications. Recently, the laparoscopic approach has been used successfully to resolve postoperative chylous ascites. 15–17 It is less invasive than the former conventional surgical technique. The lymphatic leaks can be magnified, and efficient treatment is achievable with clips, sutures, coagulation, and use of biologic glue. 15,17 Conversely, opposition to surgery stresses the hazards of reoperation in malnourished and immunocompromised patients who have barely recovered from previous major surgery and complications. 7 Despite the helpful adjunctive measures available, localization and surgical repair of the fistula may be challenging and may lead to morbidity and surgical management failure. 18
Conclusion
Chyloperitoneum is a rare complication of aortic surgery. It usually presents with persistent abdominal distention (± abdominal compartment syndrome) and is diagnosed by paracentesis. Treatment should initially be conservative, with surgical interventions reserved for those in whom conservative measures fail.