
Abstract
The diagnosis of a lower extremity glomus tumor (GT) is often delayed owing to the lack of awareness and low level of suspicion by the treating physician. GT is thought to arise from cutaneous arteriovenous connections, often involving the nail beds. The unusual location of the lower extremity often leads to missed or delayed diagnosis and management. Surgical excision of GT is often curative and provides significant symptomatic relief. There is a paucity of information in regard to GT in general, especially among vascular surgeons. The aim of this report is to make the surgical community more aware of this disease entity based on the analysis of our own experience and review of the literature.
Glomus tumors (GTs), also termed tumors of Popoff, or Barré-Masson syndrome, are rare but often disabling conditions that are typically overlooked or misdiagnosed at early stages of disease. Although their precise etiology remains unclear, GTs are thought to arise from cutaneous arteriovenous anastomoses. These structures are densely found within fingers and toes and are responsible for temperature and vascular tone regulation, as well as sensory function. Histologically, these structures are surrounded by epithelioid and glomus cells, forming a structure known as glomus or neuromyoarterial bodies. A glomus body is composed of vessels and glomus cells in varying proportions embedded in a stroma.
GTs have been reported in about 1.6% of 500 consecutive patients with primary soft tissue upper and lower extremity tumors. 1 Multiple classifications of GTs have been proposed by several investigators, depending on the tumor histology and behavior. 2–5 They often occur sporadically and present as multiple or solitary forms. 6 Multiple tumors are unusual and differ from the solitary ones in both clinical presentation and histology. 7 When familial, GTs are often inherited in an autosomal dominant fashion. 7 A higher incidence among men has been reported in the familial forms, 8 and tumors may be present at birth or appear later in life. GTs affecting the lower extremities are thought to be distinctly rare and have been reported, but mostly limited to single case reports. The glomangiomyoma form of the tumor is frequently located in the lower extremities. A review of a single hospital's experience in Holland over 19 years revealed that only 14% of all excised GTs involved the lower extremity. 9 Even though most of the published reports state its rarity, lower extremity GTs appear not to be as unusual as previously thought. However, as noted in this case report, GT is often misdiagnosed at the initial presentation and often results in a delay in management.
Case Report
A 74-year-old diabetic man presented with a 2-month history of exquisite tenderness and induration in the medial aspect of the right thigh. His past medical history was significant for end-stage renal disease secondary to a nephrectomy owing to renal cell carcinoma. Physical examination revealed a 1 cm–round mobile mass, with localized pain to palpation. There was no evidence of infection. He underwent a 6-week trial of pain medication, warm compresses, and leg compression for the presumptive diagnosis of superficial thrombophlebitis. He had no symptomatic improvement, and a varicose vein excision was offered. Preoperative lower extremity venous duplex ultrasonography (DU) revealed no venous insufficiency in the right leg. At operation, a 1 × 1 cm bluish friable nodule was excised. Pathologic evaluation revealed dilated vascular spaces with normal endothelial cells surrounded by a proliferation of cells with eosinophilic cytoplasm and small, round nuclei, consistent with a benign glomangioma (Figure 1). He reported complete resolution of his symptoms and was pain free at the 1-year follow-up.
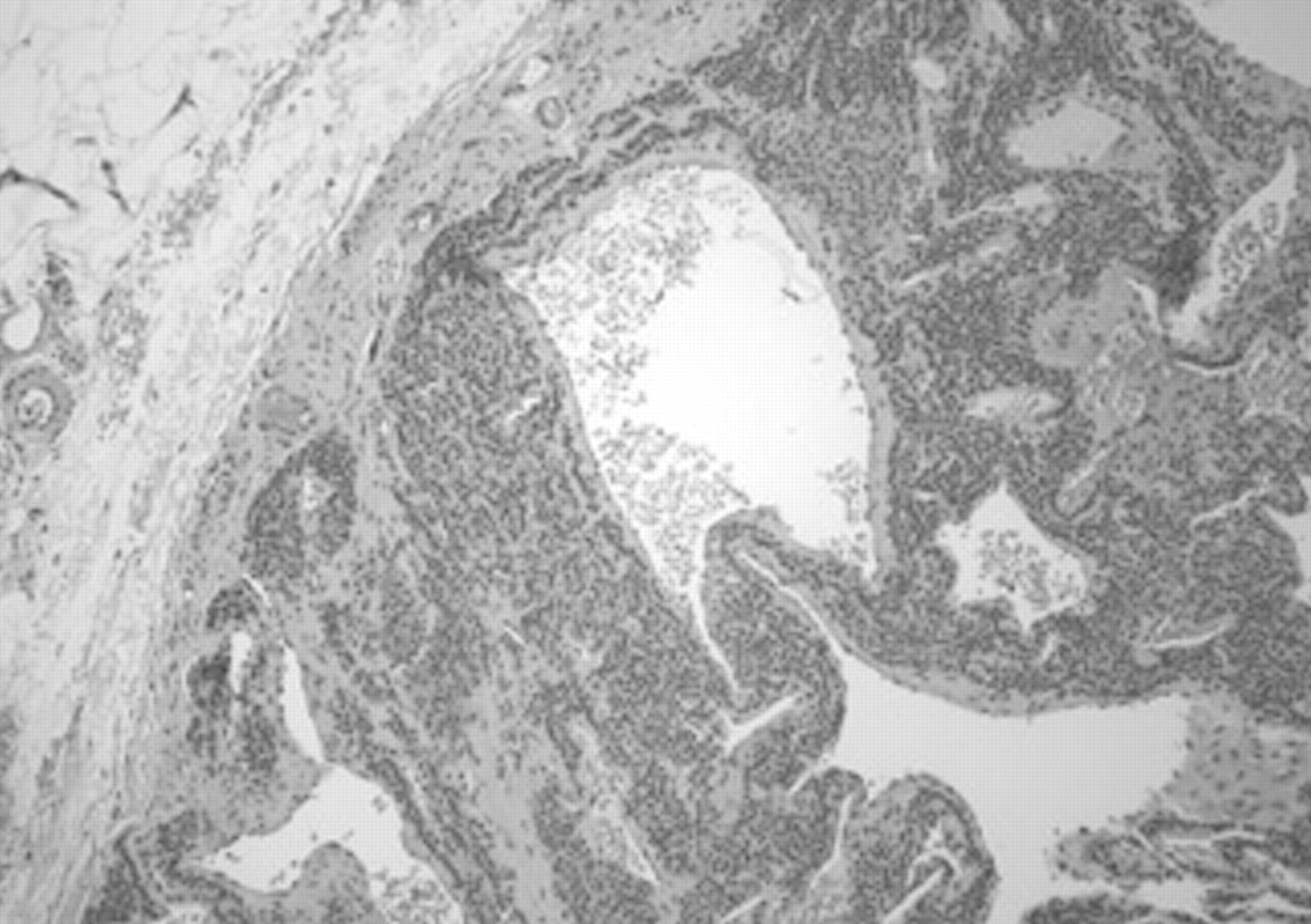
Pathology slide revealing dilated vascular spaces with normal endothelial cells surrounded by a proliferation of cells with eosinophilic cytoplasm and small, round nuclei, consistent with a benign glomangioma (hematoxylin-eosin stain; ×10 original magnification).
Materials and Methods
A Medline search (National Library of Medicine and OVID) was carried out in all languages. A manual search was also performed using bibliographies from all relevant published reports. The main key words were glomus tumor, glomangioma, glomangiosarcoma, glomangiopericytoma, glomangiomatosis, Barré-Masson syndrome, and similar terms. Other relevant terms included limb length discrepancy, leg pain or atrophy, diagnosis, clinical presentation, and management. Only atypical locations involving the lower extremity were included (excluding the feet). No prospective studies were identified. Therefore, retrospective series and case reports (n = 108) 1,4,5,9–109 were included. This article is based on those 108 reports and an additional 19 articles relating to GTs, in typical and atypical locations (127 references in total). 1–127 These articles were primarily published in nonvascular surgical, orthopedic, medical, dermatologic, and multiple other subspecialty journals. The vascular literature was represented by only three references included in journals of angiology 10–12 and one publication in Cardiovascular Surgery. 13 No articles were found in the subspecialized vascular surgical literature. Most of these references (over half of them) were published within the last 20 years.
Cases were subdivided into benign solitary (n = 64), 1,4,11,14–35,37–44,75–92,94–97,99–103,106–108 benign multiple (n = 32), 9,10,13,36,45–64,93,98,104,105,109–111 and malignant GTs (n = 12). 5,12,65–74 One report was included in both benign solitary and multiple categories as it reported cases of both solitary and multiple benign GTs. 64 Three reports were cited in other references (Frykholm, Paes, and Singh), but the actual articles were not found, despite a thorough search.
Reports were classified according to language and the type of specialty journal in which they were published, as well as publication year. Data were analyzed with respect to demographics, tumor number, size, location, and histology. Several authors compared tumor sizes with those of legumes, objects, or fruits. To approximate actual size as accurately as possible, we attributed estimated sizes to the objects to which the tumors were compared (pinhead masses, 1 mm; wheat, grain, or rice, 4 mm; small chickpeas, flattened garden pea, peas, or small nodules or formations, 7 mm; large peas or coffee beans, 10 mm; small walnut, almond, or hazelnuts, 13 mm; hazelnuts or small coin, 15 mm; lima beans, 20 mm; cherries or finger tip, 25 mm).
We also analyzed our own experience (Veterans Affairs Hospital [VA] and University of Arizona Medical Center [UMC] in Tucson, Arizona) from 1985 to 2006 by analyzing the same parameters mentioned above.
Statistical Analysis
Descriptive statistics were used to analyze the patients' characteristics. A two-tailed unpaired t-test was used to compare the ages between benign solitary and benign multiple groups (normality test, p = .3), and the Mann-Whitney rank sum test was used to compare ages between the benign solitary and malignant groups, as well as between the benign multiple and malignant groups (normality test, p ≤ .0001 and p = .0283, respectively). Differences in proportions were analyzed with the chi-square test. Yates correction for continuity and the Fisher exact test were used when the expected value in any of the cells was below a desirable level.
Results
Arizona Experience
Our experience revealed 13 cases of GTs at UMC, with 7.7% of cases affecting the lower extremities (1 case in the right lower extremity). At the VA, 16 GT cases were identified during the same interval, with 1 case affecting the right knee and 1 the left thigh, as described in the case report (12.5%).
Literature Review
Our 29 cases and those from the literature comprise 292 atypical GTs. The demographics of all groups, tumor size, location, and laterality are described in Table 1.
Literature Review on Lower Extremity Glomus Tumors
NA = not analyzed (given the indeterminate number of tumors, the anatomic area of the affected limb could not be properly analyzed).
*We were unable to precisely determine the exact size of tumors given that in 13 patients, the authors did not or could not count them.
†One patient had synchronous multiple leg and thigh tumors.
Among benign solitary lesions, histologic examination reported GT in the vast majority of cases (80), followed by glomangioma (17), cutaneous angioleiomyoma (10), angiomyoma (3), glomangiopericytoma (1), and angioleiomyoma (1).
For the benign multiple lesions, it was impossible to determine the exact number of tumors. In 13 patients, the authors did not or could not count them. The mean age of patients with multiple tumors was significantly younger than that of those presenting with solitary benign GTs (p = .0054). Given the indeterminate number of tumors, the anatomic area of the affected limb could not be properly analyzed. Pathologic examination revealed six glomangioma cases and one case each of diffuse multifocal GT, glomangiomatosis, and glomangiomyoma, whereas the remainder were GTs (n = 29; 2 cases reported by Singh and colleagues could not be retrieved).
For malignant lesions, solitary masses affected 28 patients, whereas multiple ones were present in 5. There were no significant age differences between patients with malignant versus those with solitary GTs (p = .61). However, patients with malignant tumors were significantly older than those with benign multiple ones (p = .0035). A nonsignificant trend for female gender predominance was noted in the malignant group (p = .32). Pathologic evaluation showed infiltrating or malignant GT in 16 patients, glomangiosarcoma in 7, a combination of glomangiosarcoma and GT in 2, glomangiomatosis in 2, 4 cases of atypia of uncertain malignant potential, and 2 symplastic GTs.
Discussion
The first clinical description of a GT was made in 1812 by Wood, who described it as a “painful cutaneous tubercle.” 64 It is noteworthy that although Wood's report of his cases likely corresponds to GTs, there was no pathologic confirmation. In 1924, Masson published the first comprehensive pathologic description. 3 These tumors typically present as a painful, firm, purplish, solitary, subcutaneous nodule. Multiple tumors are often softer and more compressible. 7 Tumor size is generally reported to be small, rarely greater than 1 cm. 1,57,112 Anagnostou and colleagues found that most GTs in their 13-year experience measured less than 5 mm. 112 Our review indicates that when considering lower extremity GTs, the average tumor size is slightly above 2 cm, in contrast to those tumors located in more typical locations, such as the fingers. Symptoms include intense burning pain at the tumor site, which occurs spontaneously or is precipitated by temperature changes or touch. A fear of using the lower extremity may cause severe limb atrophy from disuse, extremity vasomotor disturbances, 113 or flexion restrictions. 6
Unfortunately, GTs are not readily recognized despite severe symptoms. It is reported that the average number of years it has taken to make the diagnosis of GT from the symptom onset is 6.5. 112 Delays as long as 20 4 or even 40 112 years are reported. The delay could subject a patient to chronic point tenderness over the mass site, which can be severely disabling. This pain has been the cause of psychiatric consultation and amputations for pain control. 74 It may also cause severe chronic cold sensitivity, 15 walking abnormalities, 18 or limb hypoplasia. 113
The most important initial step for making the diagnosis of GT is the physician's awareness and clinical suspicion. Several other diagnostic tools have also been used for the most typical presentations. 114,115 Plain radiography may show subtle bony erosions in the affected phalanx. Computed tomography (CT) can accurately assess tiny cortex abnormalities of the distal phalanx. DU may depict a tumor cystic or vascular component. It may show a well-circumscribed hypoechoic area under the nail plate or subtle flow signals within the hypoechoic region. Magnetic resonance imaging (MRI) of the nail unit and the underlying bone may show a well-circumscribed mass. 115 Angiography can be normal or show the tumor as a complex of entangled vessels short-circuiting between the artery and the draining vein, a star-shaped telangiectatic zone, or ballooning of terminal arteries. 36
For atypical tumors, such in GTs of the lower extremities, MRI has been said to be the most helpful diagnostic technique. 116,117 CT has also been extensively used. 118,119 Fine-needle aspiration has also been reported with some success. 120 However, if the classic symptoms of a GT are present and the tumor is not detected by imaging, surgical exploration should be considered. 116
Complete excision is the mainstay of therapy. However, the multiple modes of tumor presentation in a variety of anatomic locations pose inherent management difficulties. Excision with negative margins results in adequate diagnosis and treatment. If malignant features are present, wide excision is needed, with close follow-up for development of metastases. 16 Some have advocated preoperative angiography to delineate tumor extent, whereas others recommended the use of a microscope to ensure complete removal. Electron beam irradiation 121 and sclerotherapy to obliterate these tumors have been used alternatively. 31 Nevertheless, all of these recommendations are anecdotal, given the rarity of these tumors. There are no guidelines pertaining to adequate margins in relation to tumor size or characteristics (solitary vs multiple or benign vs malignant) or the role of adjunctive treatments. Folpe and colleagues studied 52 atypical tumors and defined malignant glomus tumor as deeply located tumors with a size greater than 2 cm or the presence of atypical mitotic figures or moderate to high nuclear grade. 5 They identified metastases in one-third of tumors fulfilling these criteria for malignancy; no metastasis was seen among other types of GT. The malignant tumors are locally aggressive and may deserve wider margins. The rate of recurrence is uncertain owing to the rarity of these tumors. On the other hand, tumors as small as 1 cm may be responsible for the subsequent development of extensive metastases. 66 Patients with extensive metastases appear to have a poor prognosis, although these cases are extremely rare.
Conclusions
There is a generalized misconception about the frequency of GTs affecting the lower extremities. As described in this report, GT is often misdiagnosed initially and can lead to significant morbidity to the patient owing to severe symptoms, despite its benign appearance. Because of symptoms and malignant potential, diagnosis and treatment of GTs are essential. However, owing to its rarity, especially situated in atypical locations, such as the lower extremities, the treating physician must have a high index of suspicion. MRI or CT can be successfully used to make a diagnosis. However, definitive diagnosis and management depend on the surgical specimen and its analysis. Although no guideline exists in terms of adequacy of resection and adjuvant therapies, surgical excision often provides symptomatic relief and can potentially guide further therapies, including the surveillance for recurrence and potential adjuvant therapy. General and vascular surgeons must have a high index of suspicion when evaluating a patient with lower extremity pain with even benign-appearing small lesions to avoid missed or delayed diagnosis of GTs.
Footnotes
Acknowledgments
Our thanks to Ms. Karen Douglas for her assistance in obtaining the references and to Mr. Bill Malone and Drs. Karsten Fryburg, Vladimir Groysman, Anne Herbst, and Ewa Sikorski, in alphabetical order, for their help in translating the articles in foreign languages.