
Abstract
Common bile duct stenosis owing to extrahepatic portal varices is termed “portal hypertensive biliopathy” (PHB) and is a rare occurrence. We report a case of PHB owing to portal vein thrombosis with cavernous transformation successfully managed by mesocaval shunt and endoscopic retrograde cholangiopancreatography (ERCP) biliary stent placement. A 44-year-old male, who presented with hematemesis, melena, jaundice, and abdominal pain, underwent gastroscopy, which revealed bleeding gastric varices. Computed tomography with arterial and venous imaging demonstrated portal vein thrombosis with cavernous transformation and extensive extrahepatic varices within the porta hepatis causing common bile duct obstruction from extrinsic compression. Biliary decompression was achieved with ERCP, and a small common bile duct stone was retrieved. A mesocaval shunt with a 16 mm Dacron graft successfully treated the portal hypertension. PHB is rare. We report a case successfully treated by mesocaval shunt and ERCP.
Extrahepatic portal vein occlusion is a recognized cause of portal hypertension, which commonly manifests as bleeding from gastroesophageal varices. Occlusion of the portal vein with cavernous transformation results in formation of hepatopetal collaterals within the hepatoduodenal ligament, which may exert sufficient extrinsic pressure to narrow the common bile duct. 1 The term “portal hypertensive biliopathy” has been used to describe common bile duct narrowing and scarring owing to extrahepatic gastroesophageal varices. 2 We report a case of portal hypertensive biliopathy caused by portal vein thrombosis with cavernous transformation successfully managed by mesocaval shunt and endoscopic retrograde cholangiopancreatography (ERCP) biliary stent placement.
Case Report
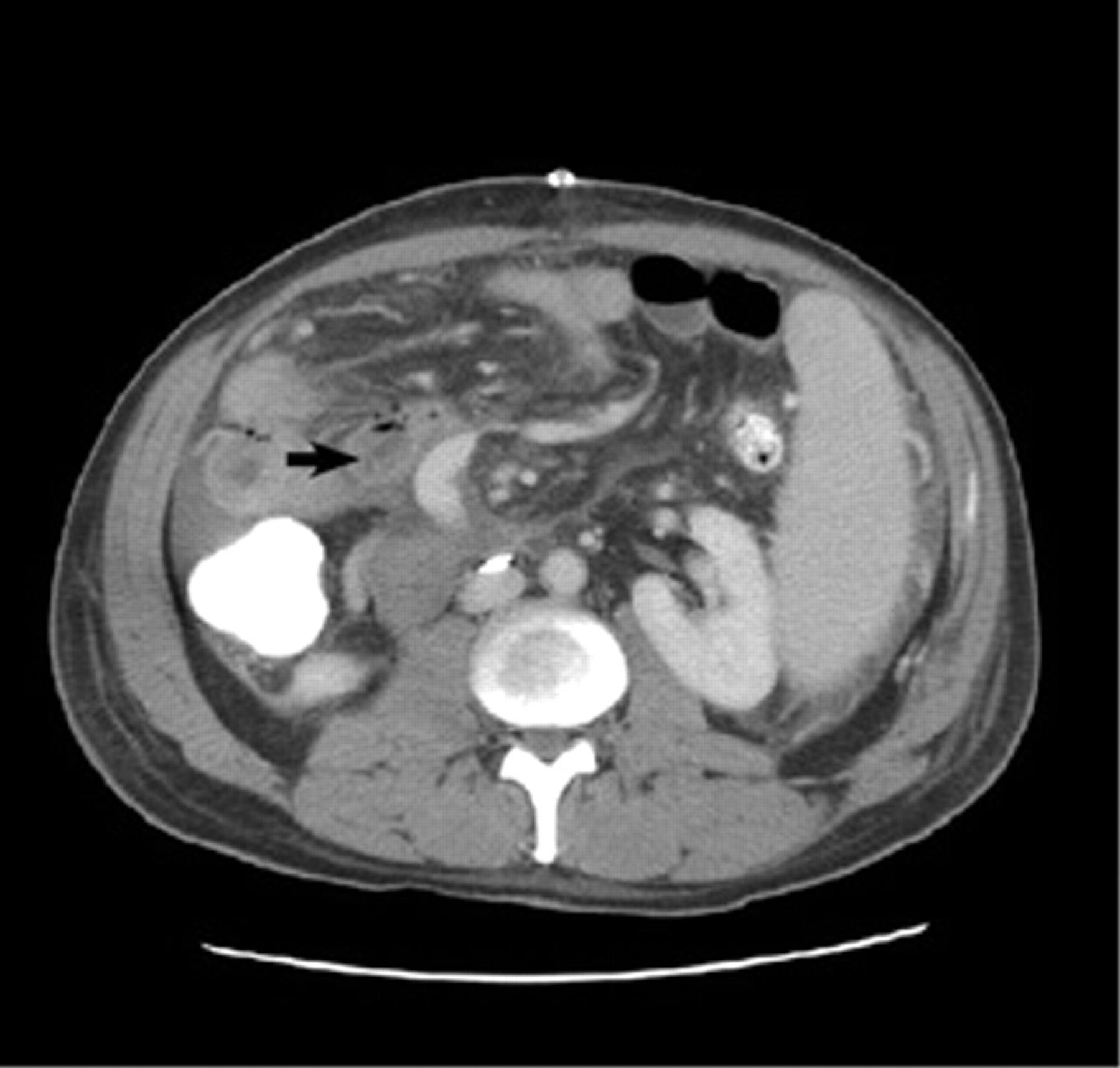
A 44-year-old male presented with hematemesis, melena, jaundice, and abdominal pain of 6 months' duration. At admission, his serum bilirubin was 300 μmol/L (normal < 20 μmol/L) and serum alkaline phosphatase was 900 U/L (normal < 130 U/L); the other liver function tests were normal. Gastroscopy revealed bleeding gastric varices, which were injected with Histoacryl glue. A computed tomographic (CT) scan with arterial and venous phase imaging demonstrated portal vein thrombosis with cavernous transformation and extensive extrahepatic varices, which caused extrinsic compression of the common bile duct and obstruction (Figure 1).

Coronal computed tomographic scan. Note extensive porta hepatis varices (arrow).
The patient was transferred to Royal Prince Alfred Hospital, Sydney, Australia, and a portal venogram documented extrahepatic, portal, and splenic vein thrombosis (Figure 2). ERCP demonstrated a smooth stenosis of the middle third of the common bile duct 1.5 cm in length, proximal to which the biliary channels were dilated (Figure 3). The narrowed segment of the bile duct corresponded in location to the site of the cavernous transformation of the porta hepatis identified on CT. ERCP was performed and successfully retrieved a small common bile duct stone, and a biliary stent was placed, which alleviated the common bile duct compression. A mesocaval shunt with a 16 mm Dacron graft was performed to provide long-term treatment for the portal hypertension and bleeding. At discharge, the serum bilirubin and alkaline phosphatase were normal, and a CT scan demonstrated a patent mesocaval shunt (Figure 4). The patient remains asymptomatic, with no further gastrointestinal hemorrhage, jaundice, or abdominal pain.

Portal venogram demonstrating occlusion of portal and splenic veins.
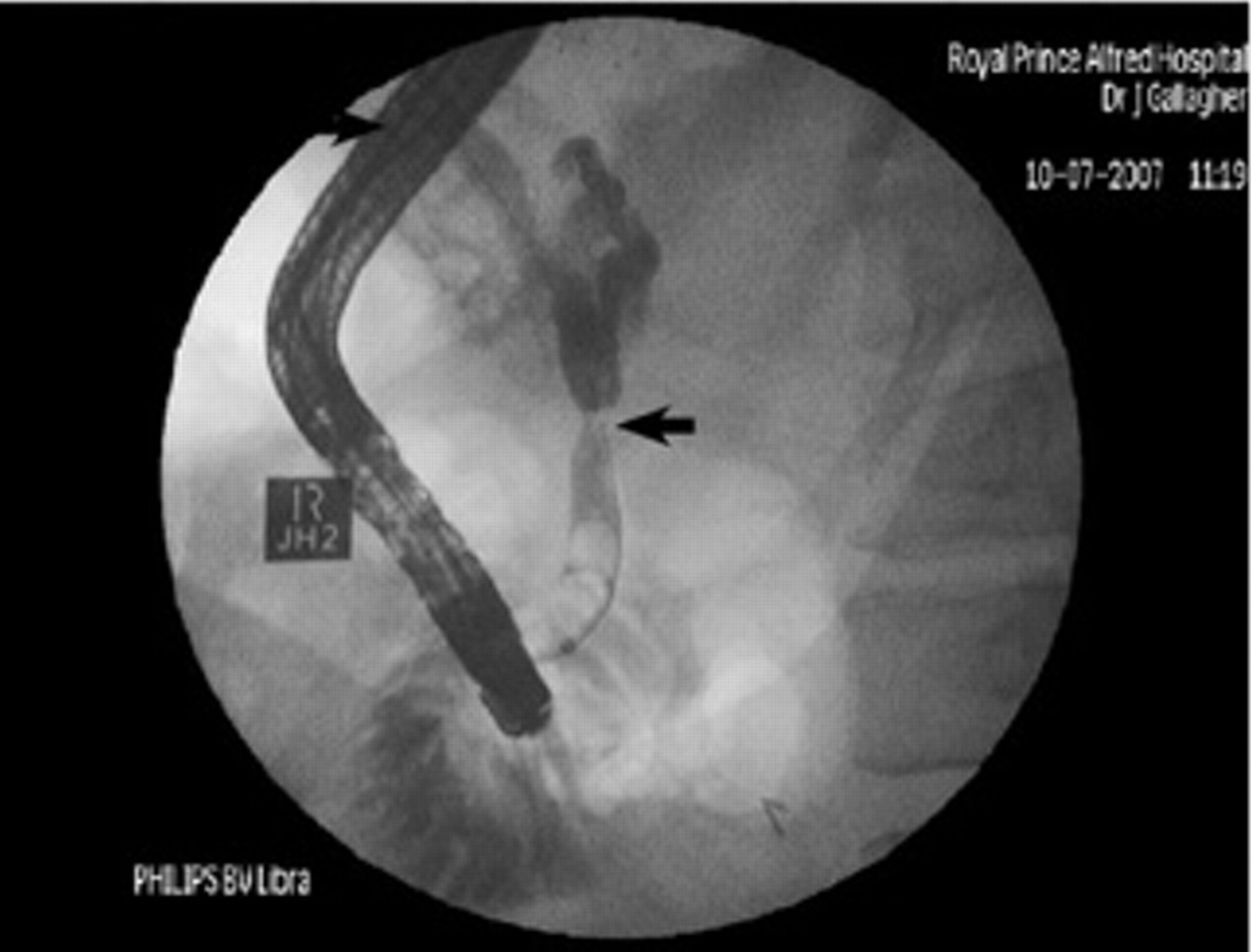
Endoscopic retrograde cholangiopancreatography demonstrating mid–common bile duct stricture (arrow) secondary to extrinsic compression by varices.
Computed tomographic scan 1 month after surgery demonstrated a patent mesocaval shunt (arrow).
Discussion
Patients with extrahepatic portal vein obstruction are known to have a high frequency of duodenal, rectal, and other ectopic varices. 3 The extrahepatic bile duct is surrounded by two venous systems: the paracholedochal veins of Petren 3 run parallel to the duct wall, and the epicholedochal plexus of Saint 4 is on the surface of the common bile duct. Engorgement of these veins from portal hypertension may produce extrinsic compression and defects in the common bile duct wall. 4,5 This ischemic scar formation does not cause symptoms in the majority of patients as the changes are patchy and diffuse. However, once a fibrous stricture or bile duct stone develops, symptoms occur, and the associated radiographic findings have been termed the “pseudocholangiocarcinoma sign.” 1 These biliary strictures that develop may be due to ischemia and bile duct injury or prolonged extrinsic compression of the biliary tree from varices. 2
Symptomatic patients are usually adults, indicating that portal biliopathy is a progressive disease. Common bile duct obstruction in these patients manifests as either jaundice, abdominal pain, or cholangitis, with jaundice being the most common. Previous reports of portal hypertensive biliopathy have focused mainly on the risks of excessive hemorrhage during surgery to relieve common bile duct obstruction and hemobilia after percutaneous transhepatic cholangiography. 6,7
A direct approach to the common bile duct in the presence of portal hypertensive varices within the hepatoduodenal ligament may lead to profuse hemorrhage and should be attempted only after previous portosystemic shunting has been performed to decompress the varices. 8 Today, obstructive jaundice caused by stricture of the common bile duct can be treated by ERCP placement of a biliary stent. The stent, however, may need to be exchanged several times to maintain bile duct patency. Choledocholithiasis in patients with portal biliopathy is rare, especially when stones are found in the common bile duct, but not the gallbladder, indicating the potential role of extrinsic compression and biliary stasis as the etiology of the common bile duct stones. 9
In the presence of portal hypertension, any operation to relieve biliary obstruction may be fraught with hazard because of the potential for significant hemorrhage. Therefore, any consideration for biliary surgery should be preceded by a decompressive portosystemic shunt. In this case, ERCP with stent placement offered a minimally invasive alternative to operative biliary decompression operation while the mesocaval shunt decompressed the portal hypertension, thereby giving the patient a durable result.
Summary
Obstructive jaundice occurring in a patient with portal hypertension is rare. We report a case of portal hypertensive biliopathy successfully treated by ERCP with biliary stent placement and mesocaval shunt.