
Abstract
Successful treatment of prosthetic vascular infection usually requires graft removal with or without replacement. A variety of materials have been used for in situ replacement, with femoral vein being the preferred autologous conduit in the literature for the aortoiliac segment. We present three cases of prosthetic infection treated successfully by in situ replacement with autologous basilic vein harvested from the upper arm. This vessel, which closely matches the iliofemoral arteries in diameter, may be a suitable alternative to femoral vein for in situ replacement of infected iliac and femoral grafts.
Prosthetic graft infection is a serious complication of reconstructive arterial surgery that can cause life-threatening hemorrhage or limb loss. 1,2 Treatment often requires graft removal, with in situ or extra-anatomic bypass to maintain distal perfusion.
Over the past decade, autologous in situ replacement, with the greater saphenous vein in the infrainguinal position and almost exclusively with the femoral vein in the aortoiliac segment, has gained popularity. We present three cases of prosthetic graft infection treated successfully by in situ replacement with autologous basilic vein.
Case Reports
Case 1
A 74-year-old woman with a 4.6 cm infrarenal abdominal aortic aneurysm and short-distance claudication owing to bilateral iliac occlusive disease underwent an aortobifemoral bypass. Two weeks postoperatively, she developed right groin cellulitis, with purulent discharge and systemic sepsis. Cultures grew methicillin-resistant Staphylococcus aureus (MRSA). Following a 4-week course of intravenous vancomycin, the cellulitis and the systemic sepsis settled and the inflammatory markers normalized, but she was left with the right limb of the graft exposed (Figure 1A). Computed tomography (CT) confirmed ascending graft infection, with soft tissue abnormalities, however, limited to the right limb of the graft up to 3 cm above the inguinal ligament; wound cultures still grew MRSA. The right limb of the aortobifemoral bypass was exposed extraperitoneally, proximal to the infected area, as indicated by CT. The graft, found to be well incorporated, was disconnected and anastomosed to the previously harvested left basilic vein, nonreversed (Figure 1B). The distal end of the vein (flaccid, as the valves prevented filling of the conduit beyond the first competent valve) was sutured to the distal stump of the graft and then delivered into the groin after closure of the iliac wound still attached to the distal graft segment. The remainder of the graft was excised, and the basilic vein was sutured to the femoral arteriotomy after valve lysis (Figure 1C) and covered with a sartorius flap (Figure 1D), prior to skin closure.
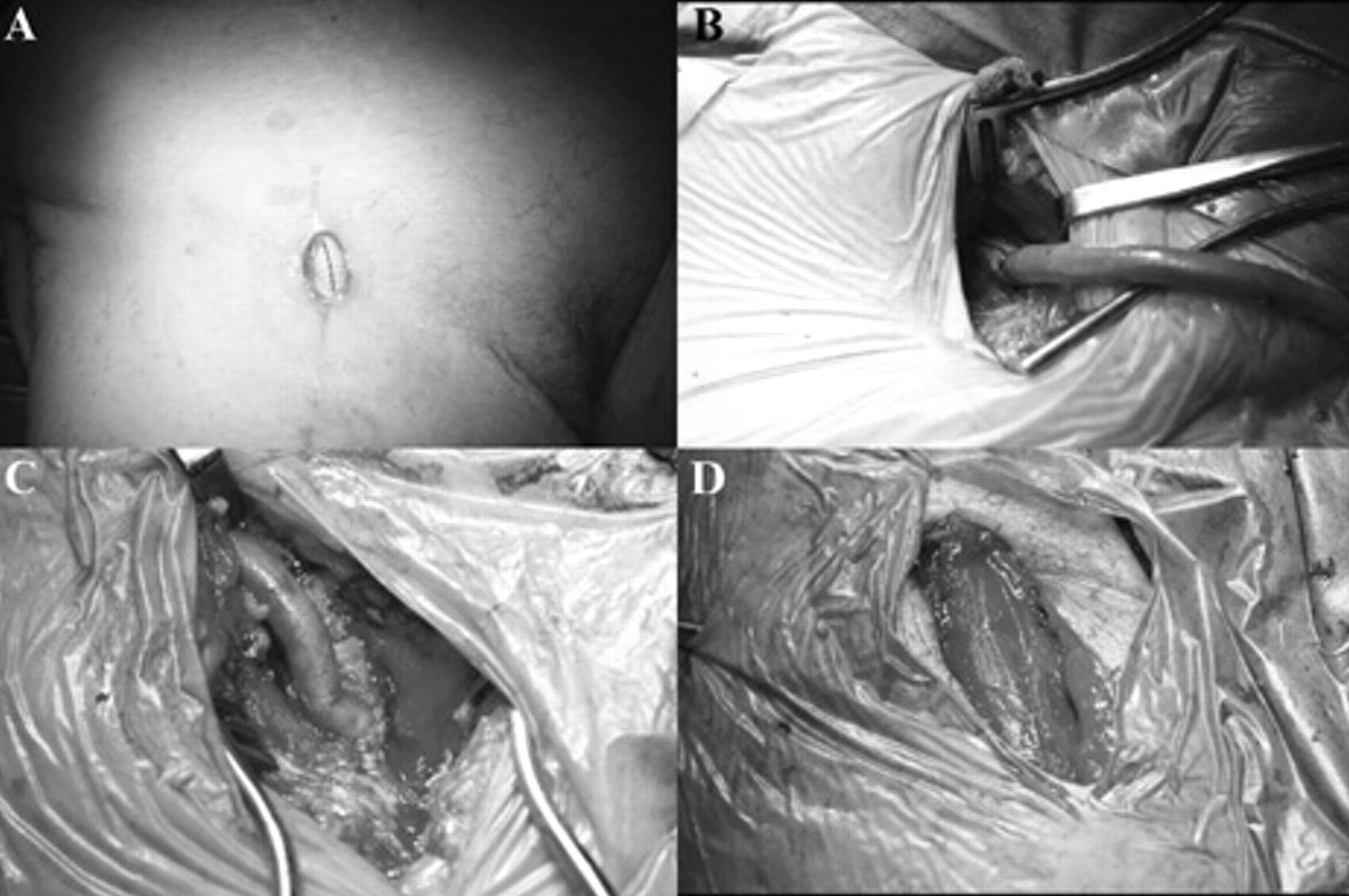
Operative stages in case 1: exposed right aortofemoral limb (A); graft–basilic vein anastomosis (B); femoral anastomosis (C); sartorius flap coverage (D).
Thirty-four months later, the patient was well, with no evidence of recurrent infection, normal inflammatory markers, and palpable pedal pulses.
Case 2
A 79-year-old man who, 1 year previously, had undergone endovascular abdominal aortic aneurysm repair with recanalization of an occluded right common iliac artery, developed a tight stenosis of his right distal external iliac and common femoral arteries, the only runoff vessels to the right endograft limb. The stenosis recurred early after percutaneous angioplasty; thus, the distal external iliac and the common femoral arteries were replaced surgically with a short Dacron graft. Eight months after this procedure, he presented with right groin swelling and a discharging sinus. Cultures from the sinus grew mixed flora (gram negatives); a CT scan (Figure 2) and a white cell scan confirmed the clinical diagnosis of graft infection. The graft was thus excised and replaced with a reversed basilic vein; the wound was closed primarily. The postoperative recovery was uneventful and, at 4 months, the patient was free of local or systemic sepsis.
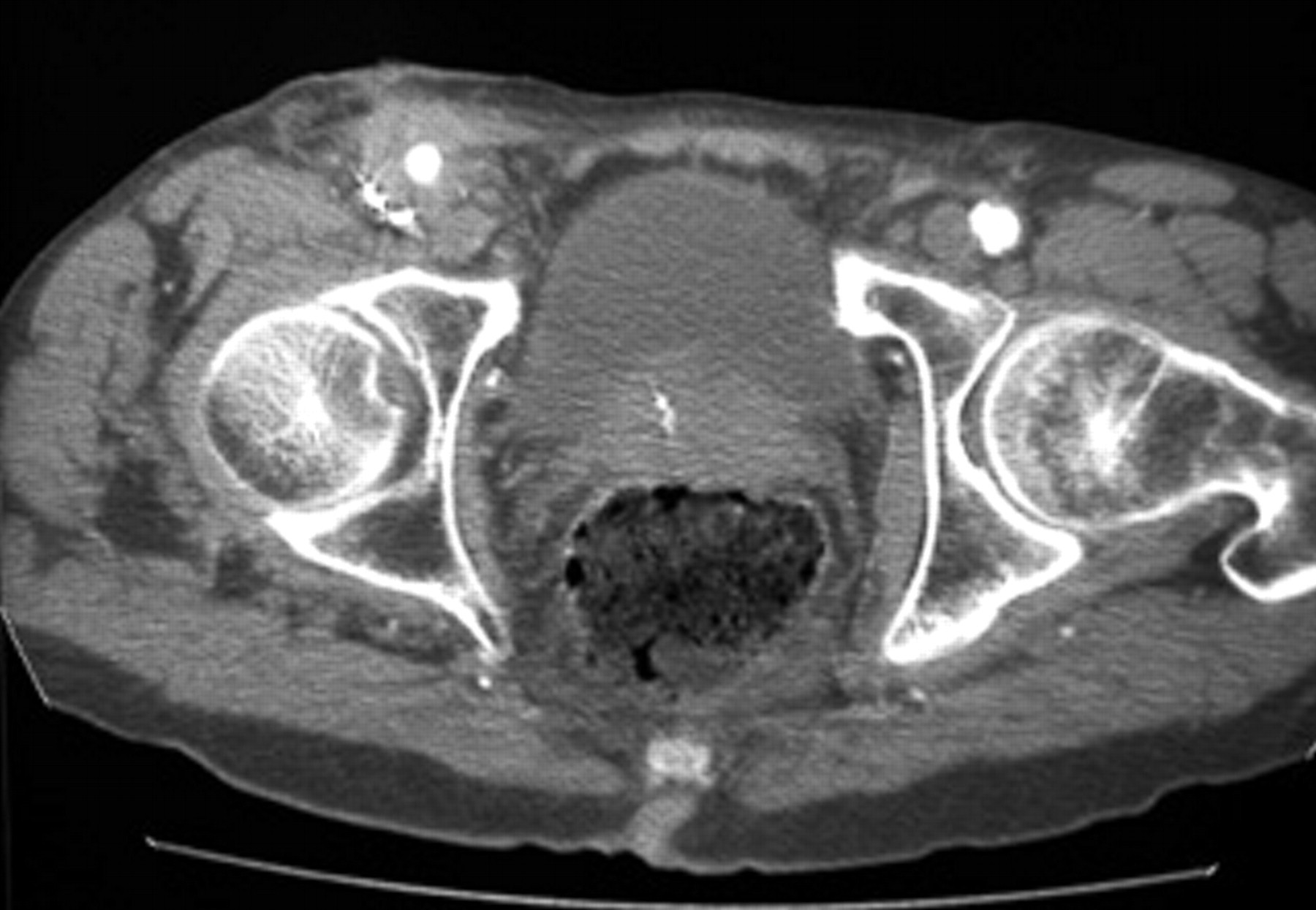
Preoperative computed tomography cross section of case 2 showing perigraft soft tissue abnormalities in the right groin.
Patient 3
A 66-year-old diabetic man with critical ischemia of the right leg underwent, in stages, graft replacement of an occluded common femoral artery (Dacron), below-knee femoropopliteal bypass (polytetrafluoroethylene), and amputation of multiple toes.
Three months after the bypass, the patient developed purulent discharge from his groin and popliteal wounds; culture of the pus confirmed MRSA infection.
The two grafts, which were surrounded by pus, were thus removed, and the common femoral graft was replaced with a short segment of reversed basilic vein, to maintain perfusion of the profunda femoris, and was covered with a sartorius flap. This graft allowed us to delay a major amputation and to perform this electively below, rather than above, the knee 3 months later, after complete eradication of the infection and closure of the popliteal wound. The below-knee amputation healed by primary intention. Six months after graft replacement, the patient was free of infection and rehabilitating with the aid of a prosthetic leg; the patency of the vein graft was confirmed by duplex scan.
In addition to graft replacement, after consultation with our microbiologists, all patients underwent antibiotic treatment guided by tissue cultures for a duration ranging from 2 weeks (case 2) to 8 weeks (case 1). Soft tissue débridement was also performed, and rifampicin powder was used, topically, at the time of surgery in all patients.
Discussion
Our limited experience demonstrates the feasibility of in situ replacement of infected prosthetic vascular grafts with basilic vein. This was successfully performed even in two cases of virulent infection (MRSA) and resulted in a durable outcome in at least one case.
Treatment of prosthetic graft infection often requires surgical removal of the infected graft. In patients with peripheral arterial reconstructions, this may result in severe ischemia and thus major amputation. Several strategies have been proposed to maintain arterial continuity in these circumstances, including extra-anatomic bypass and in situ reconstruction with infection-resistant material such as antibiotic-bonded prosthetic grafts, homografts, or autologous vein. 3 Owing to the relative rarity of prosthetic vascular infection, it is unknown whether one strategy is preferable to others; in situ prosthetic replacement, however, may result in poor outcome in cases of virulent infections such as MRSA. 4 Total replacement of the infected graft is often performed, but partial replacement has been successfully used in localized infections, 5 as in one of our patients. Autologous conduits other than femoral vein appear to be used rarely, 6 and we could not find any reports on the use of arm veins.
The upper arm basilic vein is a large vessel, usually matching in size the iliofemoral arteries, and, being subfascial for most of its course, is largely protected from venipunctures. Intuitively, therefore, it may be used as a conduit for in situ reconstruction of aortic, iliac, and femoral infected grafts.
Arm vein harvest rarely results in significant ill effects, such as limb swelling or pain, 7 and is performed away from the infected field. Conduit length, however, may be a limiting factor when compared with femoral vein grafts, although this may be overcome, in part, by bilateral harvesting.
Conclusion
Our experience shows that the upper arm basilic vein can be used for in situ replacement of infected prosthetic vascular grafts. Its use may be considered when alternative conduits, such as the femoral vein, are not available for use.