
Abstract
Although iliac artery (IA) endarterectomy has largely been replaced by bypass and endovascular options, open endarterectomy continues to play an important role in selected patterns of occlusive disease. The objective of this report is to present a contemporary clinical series of patients having undergone IA endarterectomy. Specifically, we define patterns of disease amenable to open endarterectomy and provide an updated technical note of this procedure. A retrospective study on 23 patients with IA occlusions unsuitable for radiologic intervention (TransAtlantic Inter-Societal Consensus [TASC] C and D lesions) underwent extraperitoneal IA endarterectomy. Twenty-five primary IA endarterectomies were performed. Of these, five required more extensive endarterectomy, three of the distal aorta and two of the contralateral IA. Sixteen of the 25 endarterectomies required common femoral artery endarterectomy and 6 required iliofemoral bypass. The average follow-up was 26 months. Procedure-related mortality occurred in one patient (4.3%). Within 4 months, one patient underwent an aortofemoral bypass and two patients required major amputation. Primary patency rates were 96% at 3 months and 88% at 1, 2, and 3 years. This series shows that in selected patterns of aortoiliac occlusive disease, endarterectomy remains an important alternative to consider.
In 1946, the Portuguese surgeon Cid dos Santos attempted an embolectomy on a superficial femoral artery (SFA). 1 By mistake, he entered the wrong arterial plane and performed the first recorded endarterectomy. Following a successful series of operations by Wylie in 1952, 2 aortoiliac endarterectomy became a standard surgical procedure for aortoiliac atherosclerotic occlusive disease. 3,4 Common iliac artery (CIA) endarterectomies were originally performed through a transperitoneal approach for diffuse disease extending from the infrarenal aorta to the external iliac artery (EIA). Extraperitoneal approaches have included vertical incisions splitting the inguinal ligament and separate inguinal and oblique iliac fossa incisions. 5 The introduction of prosthetic grafts enabled aortofemoral bypass grafting to become the gold standard technique, particularly with EIA disease. Femorofemoral crossover grafts, first described in 1952 by Freeman and Leeds, 6 became a suitable alternative in high-risk patients.
In 1964, Dotter and Judkins described the role of angioplasty in the lower limb. 7 Inflatable balloon catheters dilating stenoses advanced the role of catheter-based interventions, 8 and nowadays, the availability of stents has improved the durability of angioplasty. The TransAtlantic Inter-Societal Consensus (TASC) published guidelines on the classification of lower limb peripheral arterial disease in 2000, which was revised in 2007. 9,10 Radiologic intervention is recommended for TASC A and B lesions. Some TASC C lesions (bilateral CIA occlusions, bilateral EIA stenoses, unilateral EIA and common femoral artery [CFA] stenoses or occlusions) can be treated with modern interventional techniques, although open surgical management is well established. TASC D lesions (infrarenal aortoiliac occlusion, diffuse aortic and bilateral iliac disease, multiple stenoses or occlusions of unilateral IA and CFA, or bilateral CIA and EIA occlusions) represent the most complex lesions and are mostly managed with open surgery.
Although the success of bypass and endovascular interventions has resulted in a reduction in the number of iliac endarterectomies, a selected group of patients who may benefit from this approach remains, specifically, those patients whose disease pattern or comorbid conditions do not allow for bypass or endovascular options. The objective of this article is to describe a contemporary series of iliac endarterectomy focusing on patterns of disease that may be amenable to this option and to provide a technical update on the extraperitoneal approach to this important procedure.
Method
Patient Selection
All patients who underwent extraperitoneal common and/or external iliac artery endarterectomy between 2001 and 2005 at our center were included in this retrospective study. Preoperative imaging included transfemoral angiography (n = 13), computed tomographic angiography (n = 6), and magnetic resonance angiography (n = 4). Two patients had unsuccessful iliac angioplasty attempts prior to endarterectomy. At the time of surgery, all patients were deemed unsuitable for endovascular treatment of their iliac lesions either owing to disease extent (all patients had TASC C or D lesions, and angioplasty was thought likely to have a limited primary patency rate and would require further interventions) or to infection risk. Follow-up of patients was calculated up to April 2006 (owing to limited accessibility to data).
From the clinical notes, the following were recorded: age, sex, past medical history, smoking history, symptoms, operative procedure performed, operation duration to the nearest quarter of the hour, blood transfusion history, postoperative complications, vascular follow-up, and hospital inpatient length of stay.
Surgical Technique
Via a “hockey stick” incision (gridiron incision extended medially in a curved fashion) in the iliac fossa (Figure 1), the aorta and common iliac arteries were exposed using an extraperitoneal approach. When appropriate, the presacral sympathetic plexus was identified and dissected away from the aortic bifurcation, preserving it. A longitudinal arteriotomy was made, and endarterectomy was performed using a dissecting spatula. The cleavage plane between the media and intima was dissected, and the atherosclerotic plaque was removed (Figure 2). The arteriotomy was closed with 6-0 polypropylene. Polytetrafluoroethylene (PTFE) grafts were used when a CIA to CFA bypass was indicated. Separate longitudinal incisions were made infrainguinally for endarterectomy on the SFA and profunda femoris artery (PFA), sometimes with the addition of a PTFE patch.

“Hockey stick” incision in the left iliac fossa with additional infrainguinal longitudinal femoral artery exposure incision.
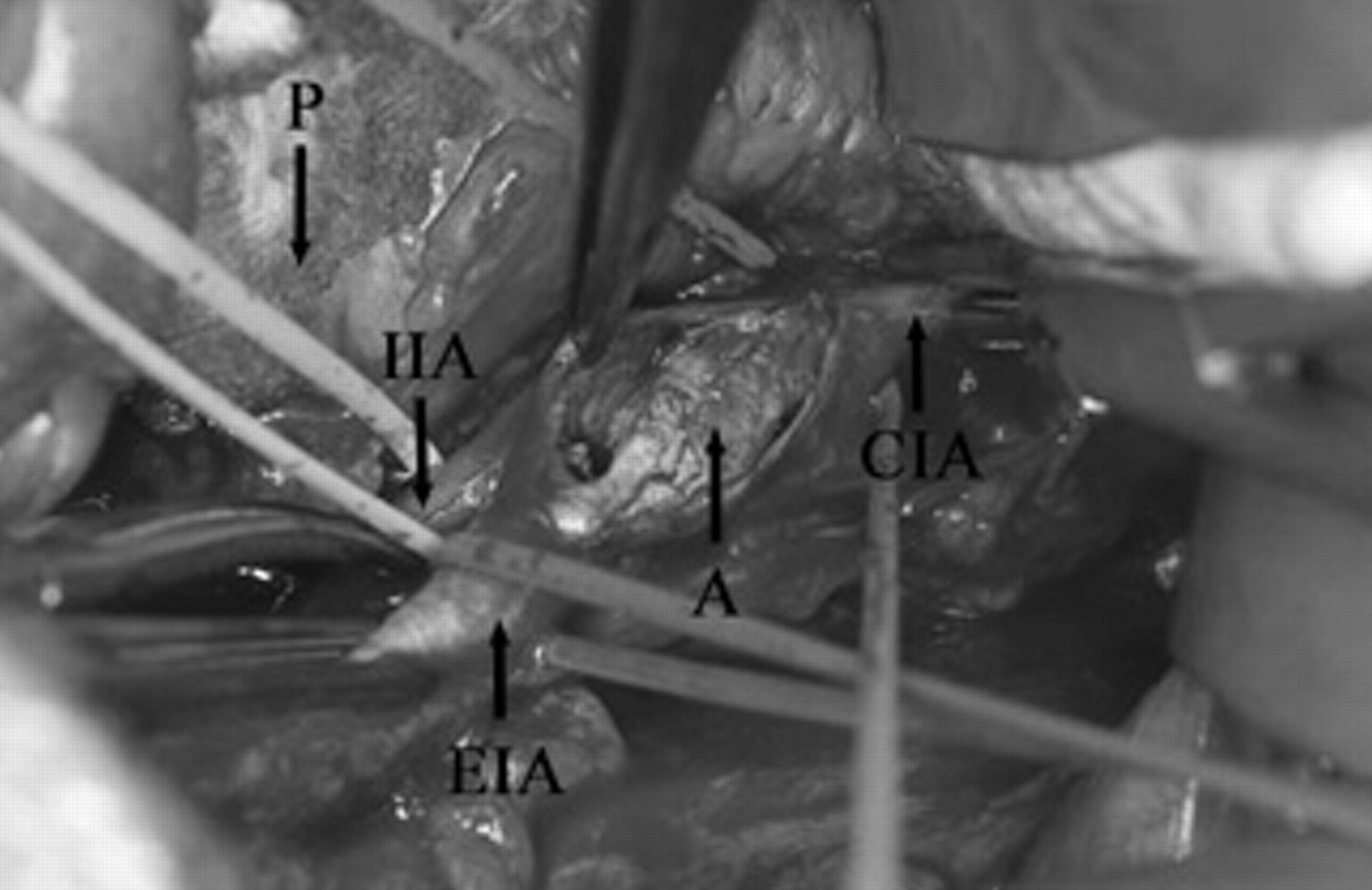
Extraperitoneal exposure of the common iliac artery (CIA), internal iliac artery (IIA), and external iliac artery (EIA) with arteriotomy and removal of atheromatous plaque (A). P = peritoneum.
Results
Twenty-three patients (4 female and 19 male) were included in the study, with an average age of 63 years (age range 47–82 years). Two of these patients had undergone bilateral IA endarterectomy but at separate time intervals; thus, 25 IA endarterectomies were studied.
Six patients were diabetic. Eighteen patients were smokers at the time of admission. Three patients had chronic renal failure, one of whom was on hemodialysis. Three patients had known ischemic heart disease, and 16 patients were on antihypertensive medication.
Indications for operation were as follows: critical limb ischemia (n = 15; rest pain n = 8 and tissue loss n = 7), claudication (n = 5), atheroembolic disease (n = 2), and emergency retrieval of a misplaced iliac stent (n = 1). Two patients with failed femorofemoral crossover grafts in situ, one of which was infected and removed, underwent endarterectomy.
Twenty-five endarterectomies were performed and categorized into three groups: (1) combined CIA and EIA endarterectomy (n = 18; 72%); (2) EIA endarterectomy (n = 4; 16%); and (3) aortic and CIA endarterectomy (n = 3; 12%). In two cases, endarterectomy of the contralateral CIA was undertaken, but the contralateral limb was not included in the study. Surgical adjuncts were performed in complement to these groups of iliac endarterectomy as follows: CFA endarterectomy (n = 16; 64%); iliofemoral bypass (n = 6; 24%); CIA PTFE patch angioplasty (n = 5; 20%); EIA or femoral artery PTFE patch angioplasty (n = 6; 24%); femoral artery vein patch angioplasty (n = 6; 24%); and endarterectomy of the contralateral CIA (n = 2; 8%) (Table 1).
Operations Performed
CFA = common femoral artery; CIA = common iliac artery; EIA = external iliac artery; IA = iliac artery; PTFE = polytetrafluoroethylene.
The average operation time was 3 hours (1¾–5 hours). Average blood transfusion was 0.8 units (range 0–4) intraoperatively and 0.4 units (range 0–3) postoperatively. This included one patient who required 3 units for epistaxis following surgery. The average discharge day was day 11 following surgery (range 3–26).
Seven operations (six longitudinal femoral incisions and one hockey stick iliac incision) were complicated by superficial wound infection, and all responded to antibiotic therapy. Two of these had iliofemoral bypasses and two had IA PTFE patches in situ. One patient suffered a lymph leak from the wound, which subsequently settled. One patient suffered a transient ischemic attack postoperatively but made a full neurologic recovery within 24 hours. Two patients were diagnosed with acute respiratory distress syndrome, and both made a full recovery. One patient developed an incisional hernia and is awaiting surgical repair of this. Nonfatal complications within 30 days of surgery occurred in 12 operations (48%). A full recovery was made in all (except for the incisional hernia) (Table 2).
Complication and Mortality Rates
One diabetic patient underwent endarterectomy of the aorta and CIA and a separate endarterectomy of the CFA, SFA, and PFA with an iliofemoral bypass. Despite a patent graft, his foot ulceration deteriorated, resulting in a healed above-knee amputation.
One patient had bilateral CIA and EIA endarterectomies 4 months apart, both for critical ischemia, and is included in the study as two operations. Aortofemoral bypass surgery was considered high risk in view of her ischemic heart disease, chronic obstructive airway disease, and renal failure. Two months following the second operation, the iliofemoral bypass thrombosed. Thrombectomy was unsuccessful, and a below-knee amputation was performed. Complicated by sepsis, the patient died from pneumonia 60 days after the initial operation. Another patient suffered symptom recurrence 4 months following CIA and EIA endarterectomies. She subsequently underwent an aortounifemoral bypass complicated by respiratory failure requiring a tracheostomy and intensive care. She was discharged 30 days following surgery. These two cases describe the only two limb occlusions that occurred. The life table analysis summarizes limb primary patency rates (Table 3), which were 96% at 3 months and 88% at 1, 2, and 3 years. Primary assisted and secondary patency rates are not available as successful interventions or revisions did not occur.
Primary patency Life-Table Analysis
The average patient follow-up was 26 months. Procedure-related mortality occurred in one patient (4.3%). Four patients died between 3 and 25 months following surgery (mean 13 months) owing to nonrelated pathologies: ischemic heart disease, alcoholic liver disease, gastrointestinal bleeding, and small bowel ischemia. In two of these patients, a lung carcinoma and renal cell carcinoma were also found after their endarterectomies.
Conclusion
The advantages of a retroperitoneal approach as described by Yang and colleagues include reduced respiratory complications owing to a less painful incision, reduced postoperative ileus, and reduced formation of intra-abdominal adhesions. 11 In our study, acute respiratory distress syndrome occurred in two operations (8%), and bowel obstruction was not reported. The additional complications of transient ischemic attacks and incisional hernia reported here reflect the comorbidities of our patient population and possible indications for avoiding aortic surgery. Our average patient discharge is longer than expected for a limited iliac endarterectomy; however, 3 aortic, 2 contralateral CIA, and 16 CFA endarterectomies were also performed.
An advantage of IA endarterectomy is the variety of additional adjuncts that may be applied during the procedure (see Table 1). In this context, endarterectomy provides operative flexibility, allowing for adjustments to be made according to operative findings; for example, iliofemoral bypass can be performed if the backflow is inadequate. IA endarterectomy offers an alternative for managing IA occlusion, although CFA exposure or a limited bypass may still be required. In our series, seven operations (28%) avoided CFA exposure and its associated complications.
Further advantages of IA endarterectomy over aortofemoral bypass include avoiding aortic exposure and cross-clamping to reduce cardiac stress (except where the contralateral limb or aorta is endarterectomized), avoiding surgical exposure of the femoral triangle (except where the CFA is endarterectomized), and reducing the incidence of graft–enteric fistula and anastomotic aneurysm formation. The avoidance of a foreign-body Dacron graft has advantages against infection, although in this series, six (24%) iliofemoral grafts and, (20%) iliac artery and six (24%) femoral artery PTFE patches were necessary. Graft infections cause 42% of deaths and 25% of amputations. 12 Oblique arteriotomy incisions may avoid the need for a patch. 13 Endarterectomy may improve erectile function by opening stenotic hypogastric artery orifices. Comparison of aortounifemoral bypass and iliofemoral endarterectomy shows similar primary patency rates of 79% and 89%, respectively, at 8 years. 14 Revision aortofemoral bypasses have a greater morbidity than primary bypasses, and their avoidance with an initial endarterectomy enables subsequent bypass to be performed in the absence of a previous graft. Unilateral iliac disease and avoidance of midaortic exposure owing to anesthetic risk were indicators for endarterectomy rather than aortofemoral bypass in our series.
The disadvantages of a femorofemoral crossover graft compared with IA endarterectomy include foreign-body insertion, significantly reduced 8-year primary patency rates of 74% versus 89%, 14 contralateral hemodynamic steal syndrome, and femoral triangle complications (hematoma, lymphocele, infection). The advantages of a femorofemoral crossover graft include less invasive surgery and an improved morbidity rate in sick patients. Lorenzi and colleagues reported a 30-day mortality of 4.2% for femorofemoral crossover grafts and 0.7% for iliac endarterectomies and/or iliofemoral bypass. 15 A comparison between aorto- or iliounifemoral and femorofemoral crossover grafts showed no difference between secondary patency rates at 22 months. 16
Indications for aortoiliac endarterectomy include claudicants with occlusive disease limited to the aorta and CIA, women with small arteries deemed unsuitable for bypass surgery, male patients with hip and leg claudication and erectile dysfunction, high–infection risk claudicants, and following the removal of an infected graft. 17 We would add to this list patients under 55 years, 18 unilateral iliac disease, acute stent migration, patients unsuitable for radiologic intervention (owing to sepsis, some TASC C and D lesions), and patients in whom aortic cross-clamping is considered a high anesthetic risk. Earlier studies have advocated IA endarterectomy only if the disease did not extend distal to the CIA bifurcation. 3,10,18 EIA endarterectomy can be challenging owing to its smaller size, its difficult exposure, and its adherent muscular media. Recurrent EIA disease requires reoperation in 20% of limbs at 5 years and 32% at 10 years. 3 In 18 (88%) of our patients, endarterectomy of the EIA was performed, mostly as a short continuation of the CIA endarterectomy. Contraindications to aortoiliac endarterectomy include a narrow lumen, tortuosity, extensive calcifications, and previous endarterectomy. 19
The ring strip cutter (MollRing Cutter, Vascular Architects Inc, San Jose, Calif) and Vollmar ring stripper enable retrograde endarterectomy of iliofemoral occlusions under local anesthesia. 20 They avoid prosthetic material, anastomotic complications, and extraperitoneal dissection. They are less suitable for aortic and CIA disease and were thought to be inadequate in our patient population.
Although our management of TASC C and D lesions has been collectively described, separate analysis would allow comparisons with other studies. The distal runoff is a known independent predictor of primary failure after open surgical management of TASC C lesions, 21 although angiographic runoff scores (proposed by the Ad Hoc Committee on Reporting Standard, Society for Vascular Surgery/International Society for Cardiovascular Surgery) were not calculated in our study.
Technological advances are improving the endovascular management of TASC C and D lesions, although 24% of patients may still require a femoral endarterectomy or patch plasty. 22 It is important to stress that endarterectomy is not the preferred treatment for all iliac lesions but is recommended for selected cases. As 65% of our patients had critical limb ischemia, a definitive procedure was sought rather than attempting repeated angioplasties. We report a contemporary series of open iliac endarterectomy applied to patients with TASC C and D lesions who were not candidates for endovascular intervention. Applied selectively to patients with these patterns of disease and with the use of surgical adjuncts tailored to the patient's needs, and based on operative findings, endarterectomy continues to provide good long-term patency with limited morbidity and mortality.