
Abstract
Intraoperative control of bleeding during any surgical procedure is vital for achieving a positive patient outcome. Hemostasis can be achieved through practical and effective systemic or topical approaches. A variety of hemostatic methods can be employed, ranging from simple manual pressure application with one finger to electrical tissue cauterization, systemic administration of blood products, and systemic administration or topical application of procoagulation agents. The key to surgical success is critically dependent on knowledgeable use of a method appropriate for the level of bleeding experienced by the patient. Topical agents can be effective as adjuncts to aid in hemostasis when bleeding is not controllable with pressure application, vessel ligation, or electrocautery. Such adjunctive hemostatic treatments include topical gelatins, collagens, oxidized celluloses, thrombin and fibrin sealants, synthetic glues, and glutaraldehyde-based glues. As with the use of systemically delivered hemostatic agents, topical treatments also carry risks with their use, and their efficacy has not been extensively studied in large randomized, placebo-controlled prospective studies. The effective use of topical agents is highly dependent on the surgeon's experience or preference and their availability in the surgical setting. In this article, we review the currently available topical hemostatic agents, compare their efficacy, and give general recommendations for their use in the operating room.
History of Topical Hemostatics
Woven cotton gauze has been used since the inception of surgery as a tool for hemostasis. Beeswax and petroleum jelly were introduced in 1886 as mechanical agents of hemostasis, mostly for use on trabecular vascularization of bone. 1 In 1915, fibrin from sheep blood was effectively used to aid in hemostasis and was shown to have better hemostatic effect than cotton gauze. 2 Even though thermal energy has been used to obtain hemostasis since ancient Egypt, it was in the 1920s that Cushing reported its use in neurosurgery. 3 Oxidized cellulose was introduced in 1942 as a hemostatic agent, 4 and gelatin foam and sponge made their debut in 1945. 5 Hait developed microfibrillar collagen as a new hemostatic agent in 1970, and since then, several other collagen products have been developed as hemostatic agents. 6 The last two decades have witnessed the introduction of combination products that include matrices and biologic agents such as thrombin and fibrin.
We generally categorize the different topical hemostatic agents in three major groups: mechanical, absorbable, and biologic hemostats. Mechanical agents include gauze sponge, sutures, and clips. Absorbable hemostatic agents include cellulose, gelatin foams, collagen, and biodegradable matrices that absorb blood and activate platelets and subsequently induce coagulation through contact activation. Thrombin and fibrin sealants encompass biologic hemostatic agents and exert their action by initiating coagulation both biologically and through contact.
Mechanical Hemostasis
When bleeding is encountered in any surgical procedure, the first line of defense is manual pressure to the bleeding area. Mechanical pressure can be applied using gauze sponges. This buys the surgeon time to carefully evaluate the extent of vascular injury, mobilize tissue surrounding the bleeding vessel for better exposure, and assemble necessary sutures and special instruments for the repair of the injury. Electrocautery, sutures, and clips are the traditional mechanical hemostatic tools used. Argon beam coagulation is also another relatively new hemostatic tool that is commonly applied during hepatic resections or large raw surface bleeding.
A new bipolar sealing technology recently received clearance from the US Food and Drug Administration (FDA) and is used to hemostatically seal and coagulate bleeding from soft tissue and bone.
7
This technology works by simultaneously integrating saline and radiofrequency energy, allowing thermal energy to gently reach targeted tissues. One potential advantage of this device is that it keeps tissue temperature below 100°C, which prevents the burning associated with the use of conventional electrocautery. On a molecular level, the technology modifies specific types of fibrous collagen by remodeling its triple-helix structure, initiating a biomechanical process that permanently stops bleeding by narrowing the lumen of the vessel (Figure 1). The technology can be used to paint broad tissue surfaces to both prevent and treat active bleeding or used to spot treat individual bleeders. The technology is primarily used to reduce blood loss during total joint and spine procedures. A monopolar version of the technology, used primarily for liver resections, is also available.
7
Bipolar sealing technology. A shows a bipolar sealing device with a close-up of the device electrodes and saline. B shows tissue effect as a function of tissue temperature secondary to external heat application with a cautery device. By operating near 100°C, the user captures the positives of electrosurgery (ie, hemostasis), without the negatives of operating at excessive temperatures–-sticking, smoking, and superficial eschar that limit the hemostasis effectiveness.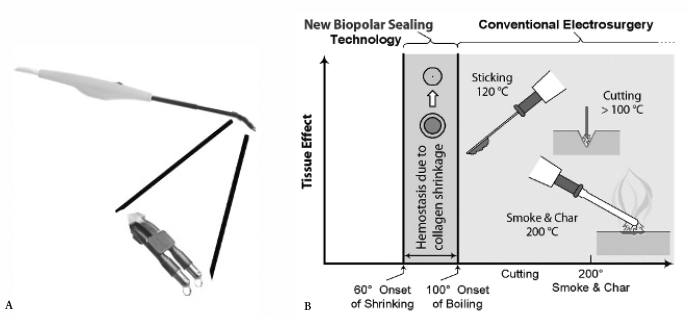
Absorbable Hemostatic Agents
Oxidized Cellulose
Oxidized cellulose was first introduced in 1942. 4 A small piece of sheet is applied to the bleeding area, at which point, clotting is believed to be initiated through contact activation, although the exact mechanism is not known. It creates a low pH environment and red cell lysis, with subsequent oxidization of hemoglobin. This results in its dark coloration after contact with blood. Its low pH characteristics are important, so one should not consider using other biologically active topical agents, such as thrombin, as they become inactivated.8,9 Oxidized cellulose has been shown in animal studies to dissolve within 2 weeks, with complete dissolution by 6 weeks.4,8 Even though the material dissolves in a short period, absorption of the residue could take a long time. One case report showed the presence of oxidized cellulose fibers histologically near a coronary bypass graft anastomosis 5 years after the procedure. 10 It is therefore recommended to leave only the minimum amount of cellulose material necessary for hemostasis.
Gelatin Foams
Gelatin foams were introduced as topical hemostatic agents in 1945. 5 Gelatin foam is made from animal skin gelatin whipped and baked into its sponge form. 5 The gelatin foam is available as an absorbable gelatin sponge and as a compressed sponge. On contact with blood, it expands and provides a physical matrix for clotting to be initiated and propagated. For gelatin foam to work successfully, a functional coagulation cascade is necessary.5,11 Unlike oxidized cellulose, it has a neutral pH and therefore can be used in conjunction with topical biologic agents, such as thrombin, to aid in hemostasis. It is absorbed within 4 to 6 weeks. 5
Microfibrillar Collagen
Hait developed microfibrillar collagen as a new hemostatic agent in 1970. 6 Microfibrillar collagen is available commercially in flour, sheet, or gel form. Collagen is a tissue-derived biomaterial with high tensile strength and good cell compatibility. 12 It has a high affinity to water and is easily absorbed by the body. It works both by contact activation and platelet aggregation, which subsequently results in platelet degranulation and activation of the coagulation cascade. 13 This product needs to be applied to the bleeding area with dry instruments, and manual pressure should not be applied because microfibrillar collagen will stick to the gloves of the operator. 14
Collagen has good cell compatibility, which allows for cell adhesion, growth, and migration. All of these properties make it a good topical agent to use for hemostasis. Collagen is known to have a low antigenicity. Telopeptides, the sites with the highest inter-species variability, are proteolytically digested in commercially available collagen,15,16 rendering the product even less immunogenic; however, there have been a few clinical evaluations of immunogenicity after implantation of collagen in patients. In a prospective randomized study, 5 of 68 patients implanted with a collagen-coated vascular graft developed antibovine collagen antibodies, demonstrating the potential of bovine collagen to stimulate an immune response. 17
In an in vitro evaluation, Wagner and colleagues classified absorbable hemostatic agents in the following descending order of effectiveness: microfibrillar collagen, collagen sponge, gelatin sponge, and oxidized cellulose. 18 Voormolen and colleagues compared microfibrillar collagen with oxidized cellulose in cerebral lesions in rabbits and found that microfibrillar collagen established hemostasis more rapidly and was resorbed faster than oxidized cellulose. 19
Biologic Hemostatic Agents
Bovine and Human Thrombin
Thrombin is a naturally derived enzyme that has been widely characterized for its roles in hemostasis, inflammation, and cell signaling. Thrombin has been purified from numerous sources and used as a clinical aid for topical hemostasis for more than 60 years.20,21 Owing to both its ease of use and apparent effectiveness, thrombin is used routinely as an aid for topical hemostasis in nearly all types of surgery, including cardiovascular, orthopedic, neurologic, general, gynecologic, and dental procedures.20,22 Bovine-derived thrombin has potent biologic activity in its ability to convert fibrinogen to fibrin, activate platelets, and induce vascular contraction; however, it has also been shown to induce a robust immune response following human exposure.23,24 Numerous reports have documented an array of clinical events that follow bovine thrombin exposure, which include the development of antibodies against thrombin, prothrombin, factor V, and cardiolipin.23–25 Plasma-derived human thrombin and recombinant human thrombin were recently approved by the FDA and are available on the market (<http://www.fda.gov/bbs/topics/NEWS/2008/NEW01779.html>). In January 2008, the FDA approved the first topical thrombin solution manufactured using recombinant deoxyribonucleic acid (DNA) techniques.
Gelatin and Thrombin
A combination of bovine gelatin and pooled human thrombin has been developed as a flowable topical hemostatic agent. As the product comes out of the applicator, it starts to polymerize and maintains a thick consistency. Whenever the material comes in contact with blood, it starts sticking where there is fibrinogen. 27 It does not stick to other surfaces, so it allows the surgeon to apply pressure with gauze or hemostat on top of the product on a bleeding surface. This product has wide applications, including cardiac and vascular surgery.27,28
Fibrin Sealants
Fibrin sealants are two-component products that combine heat-treated pooled plasma thrombin (mostly human) and fibrinogen (usually plasma derived). The ingredients in these sealants interact during application to form a stable clot composed of fibrin (Figure 2).
28
Fibrin sealants have gained significant market visibility in the surgical environment over the last 5 to 10 years. They have approved indications for use in cardiac surgery, splenic trauma, and liver surgery and for sealing colonic anastomoses.28–31 Their approval in the United States was delayed because of concerns of viral disease transmission as the products are purified from human plasma. The products undergo rigorous preparation, including ultrafiltration, heat treatment, and solvent detergent cleansing to remove any viruses. To date, there have been a few scattered reports of possible hepatitis transmission.32,33
A represents the physiologic structure of fibrin strands in a plasma clot, whereas B represents that of a clot formation using a fibrin sealant. Note the similarities in structure. Copyright, Baxter Healthcare Corp.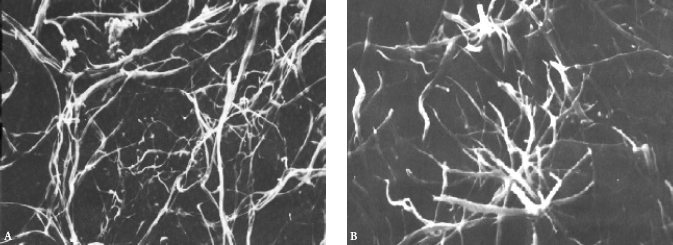
Different formulations are available on the US market. The first fibrin sealant was approved for use in the United States in 1998. It consists of heat-treated pooled plasma thrombin and fibrinogen. It is manufactured with an antifibrinolytic aprotinin (bovine) as it is not a plasminogen-free material. Recently, this formulation was modified to eliminate the need for thawing and refrigeration. A new second-generation fibrin sealant that is aprotinin free is now available that has replaced the original first-generation fibrin sealant. This second-generation formulation is also available in a premixed form, which reduces the cumbersome mixing that used to be required prior to its use in the operating room.
Other Agents
A two-component surgical adhesive composed of purified bovine serum albumin and glutaraldehyde is another topical hemostatic option. 34 The solutions are dispensed by a controlled delivery system that includes either a reusable delivery “gun” or a disposable syringe. Once dispensed, the adhesive solutions are mixed in a predefined ratio in the applicator tip, where a crosslinking process is initiated. The glutaraldehyde molecules covalently bind (cross-link) the bovine serum albumin molecules to each other and, on application, to the tissue proteins at the repair site, creating a flexible mechanical seal that is independent of the body's clotting cascade. This glutaraldehyde-based glue begins to polymerize within 20 to 30 seconds and reaches its bonding strength within 2 minutes. This product is useful for dissections around big blood vessels as it is easy to use and apply. 34 There have been some reports of systemic absorption through suture lines that subsequently cause glutaraldehyde particle emboli. 35
Suggestions for Use
Which agent to use for what type of bleeding is dependent on the surgeon's experience, material availability, and type of surgical procedure. It is critical to put some thought into both the effectiveness and potential risks of each type of product prior to using them because no product is without risk or cost. When we encounter bleeding, we generally start by applying manual pressure with the aid of a finger, gauze, or a sponge stick. For small and discrete bleeding that is not controlled by electrocautery or suturing, usually application of an oxidized cellulose or microfibrillar collagen will work. Application of topical thrombin on gelatin foam may aid in bleeding that is not controlled by the gelatin foam alone. One should remember not to use thrombin concurrently with oxidized cellulose as the thrombin will be inactivated in the acidic pH. In infected tissues and areas of abscess, oxidized cellulose is good to use, secondary to its ability to be active in an acidic environment.36,37
For large raw surface areas with small venous oozing, such as the retroperitoneum after nephrectomy or hematoma evacuation, the fibrin sealants are good products to use. They can be applied to large surface areas and will be able to control small venous oozing. For arterial bleeding, we recommend using topical gelatin containing human thrombin as it could be used in conjunction with manual pressure. Glutaraldehyde-based glue also has indications for large vessel dissection bleeding, but care must be taken to avoid systemic absorption through suture lines. One should also avoid using this topical hemostatic formulation around nerve tissues as glutaraldehyde tans tissues.
38
Figure 3 shows a general schematic of our approach to a bleeding patient.
Algorithm for use of topical hemostatic agents when bleeding is encountered.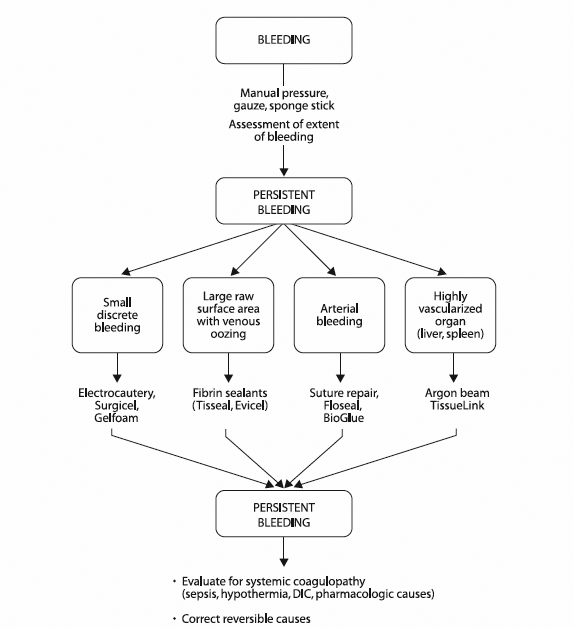
Conclusion
Topical hemostatic agents have existed for over a century and have helped with hemostasis in the operating room. Their use is highly dependent on the surgeon's experience or preference and availability. There are minimal to no level 1 data supporting the evidence behind their efficacy; rather, they are supported mostly by animal studies and small case-control studies. The availability of these agents should never replace a surgeon's pursuit of excellent surgical aesthetics.