
Abstract
The prospect of surgery without blood loss is an emerging reality. Use of a blood conservation strategy is gaining increasing recognition as a sound and practical approach, especially for the majority of large blood loss surgeries. However, critical situations still occur in which transfusions are necessary or unavoidable for the short-term survival of the patient. The decision-making processes for determining when to transfuse, which blood products to give, and how much are presented here with an evaluation of the risks of transfusion and a discussion on blood conservation strategies. Modalities that may be used in such strategies include restricted phlebotomy, the implementation of restrictive transfusion triggers, acute normovolemic hemodilution, intraoperative and postoperative blood salvage, and refined operative techniques to achieve meticulous hemostasis. In addition, the proper use of erythropoiesis-stimulating agents well before surgery can reduce the number of units transfused. The risks and costs of allogeneic blood transfusions underscore the need for and value of blood conservation techniques. Increasingly, hospitals are adopting blood conservation strategies as part of their routine practice. Blood conservation is a rapidly evolving field in which active research is expanding our understanding of the molecular, physiologic, and clinical aspects of hematopoiesis, circulatory response, coagulation enigmas, artificial oxygen carriers, and the impact of anemia on organ function. Ongoing research offers the possibility of replacement or elimination of allogeneic blood transfusions in a variety of clinical settings.
Is “bloodless” surgery an option? The short answer is a resounding “Yes.” For the majority of large blood loss surgeries, blood conservation is a sound and practical approach; however, surgeons may find themselves in situations in which transfusions are necessary for short-term survival. This article addresses the issues of deciding when to transfuse, determining which blood products to give and how much, and evaluating the risks of transfusion, followed by a discussion of blood conservation strategies.
Transfusion Triggers
Traditionally, physicians tended to adhere, albeit poorly, to rigid yet arbitrary triggers based on hematocrit or hemoglobin (Hb) levels to decide whether or not to transfuse their patients. For decades, the conviction was that Hb values < 10 g/dL and hematocrit < 30% would indicate a need for transfusion to ensure enough tissue oxygenation, especially in the surgical patient (the so-called 10/30 rule).
1
The theory behind this practice was simple. Not considering the oxygen solubility in plasma, oxygen delivery to the tissues (DO2) depends on the concentration of Hb, oxygen saturation (SaO2) of Hb, and cardiac output (CO) as follows:

Given that Hb is almost entirely saturated with oxygen, the simplest way to increase DO2, other than to increase CO, would be to increase the Hb level. 2 However, multiple studies challenge the practice by showing that mild to moderate and even severe anemia is well tolerated in surgical patients without increased morbidity or mortality. 1
Acute normovolemic anemia or hemodilution (as seen in acute bleeding with adequate fluid replacement) is associated with decreased systemic vascular resistance, increased heart rate, and stroke volume, resulting in increased CO. 3 Reduced blood viscosity has a pivotal role in increasing venous return (preload) and decreasing cardiac afterload. 4 Also, inotropic sympathetic stimulation further increases the CO. 5 Referring to the equation, this would increase DO2 to tissues in spite of a decreased Hb. 3 Moreover, normovolemic anemia is associated with microcirculatory changes and a shift of the Hb dissociation curve to the right, resulting in increased oxygen extraction at the tissue level. The above equation does not account for these observations.6–8 Most, if not all, surgical patients undergo anesthesia, which may reduce the compensatory increase in CO, although the anesthetized state can also reduce oxygen consumption. 9 Clearly, a simple equation cannot predict what happens in a complex physiologic system.
Controversy still exists on the lowest tolerable Hb level for patients in general and during surgery. Studies have shown that extremely low preoperative Hb levels (< 6 g/dL, especially with surgical blood loss > 2,000 mL) relate to much higher mortality rates in patients refusing transfusions, especially those with cardiovascular disease10,11; however, the uncontrolled retrospective nature of these studies and the lack of specific interventions undermine the quality of the evidence and make it difficult to draw any firm conclusions.
A large pivotal multicenter clinical trial on critically ill euvolemic patients showed that a restrictive transfusion strategy (transfusion if Hb < 7 g/dL, maintenance range 7 to 9 g/dL) is as effective as and possibly superior to a liberal transfusion strategy (transfusion if Hb falls below 10 g/dL; maintenance range 10 to 12 g/dL), although it is inconclusive, with the possible exception of cases with acute myocardial infarction and unstable angina. Although overall mortality rates were similar between the two groups, mortality was significantly lower in restrictively transfused patients who were younger (< 55 years of age) and less acutely ill compared with their liberally transfused peers. 12
Although a general restrictive transfusion strategy is advisable for all patients, determining the lowest acceptable Hb for each case is necessary. In the presence of coronary artery disease, signs of inadequate myocardial oxygen supply in spite of adequate cardiac medication, normovolemia, and other blood conservation techniques usually indicate a transfusion. 13 Given the limited cardiac reserve capacity in these patients, tachycardia can be detrimental and needs prompt treatment. Of note, the increase in CO in anesthetized patients is mostly due to an increase in stroke volume as opposed to heart rate. Tachycardia in the setting of acute anemia under anesthesia can be a sign of hypovolemia and should be treated as a first course with volume replacement. 13 Aortic stenosis and heart failure can interfere with anemia compensatory mechanisms as well, but patients with mitral valve insufficiency usually tolerate anemia well. 14
It has been suggested that the main compensatory mechanism in response to normovolemic hemodilution in elderly patients is increased oxygen extraction and raised arterial oxygen tension as opposed to solely increased CO. Thus, decreasing Hb can reduce DO2 to organs significantly. 15 However, studies have not demonstrated that older age in the absence of cardiac disorders would impair tolerance to acute hemodilution (Hb level of 9 g/dL). 16 Despite the paucity of available data, added caution should be applied to patients older than 80 years of age.
More often than not, Hb/hematocrit transfusion triggers fail to identify patients who can benefit the most from transfusion. Transfusion triggers should be based increasingly on physiologic parameters. As better methods for monitoring patients’ circulation, physiologic condition, and organ function emerge, they will continue to replace Hb and hematocrit as the basis for making transfusion decisions.
Table 1 presents the suggested indications for intraoperative and postoperative blood transfusion based on physiologic triggers.13,17 To use these triggers, parameters should be measured after establishing normovolemia, treating preexisting tachycardia, and optimizing anesthesia. 13 In the absence of physiologic signs of hypoxia, transfusion can be considered (but not necessarily given) with Hb levels < 6 mg/dL in the general population, < 7 mg/dL in patients older than 80 years old or in febrile or hypermetabolic patients, and < 8 mg/dL in patients with coronary artery disease or congestive heart failure.
Indications for Blood Transfusion in Surgery *
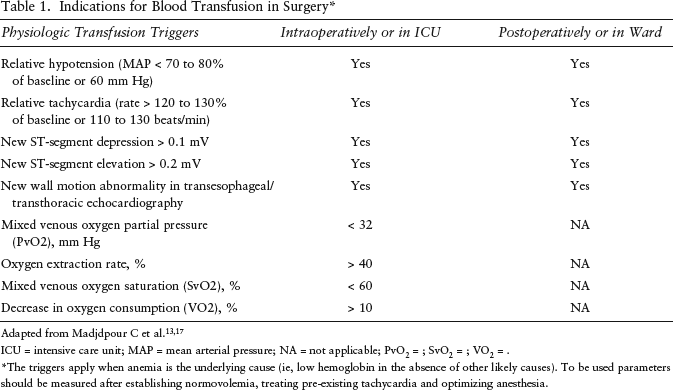
ICU = intensive care unit; MAP = mean arterial pressure; NA = not applicable; PvO2 =; SvO2 =; VO2 = .
The triggers apply when anemia is the underlying cause (ie, low hemoglobin in the absence of other likely causes). To be used parameters should be measured after establishing normovolemia, treating pre-existing tachycardia and optimizing anesthesia.
Most platelet units are used prophylactically (in patients with thrombocytopenia at risk of spontaneous bleeding or prior to surgery) as opposed to therapeutic use in patients with active bleeding with low platelet counts. A common and largely unsubstantiated practice is to prophylactically transfuse otherwise stable, nonbleeding patients at platelet counts of 20 ∞ 10 9 /L. Recent studies have questioned this trigger and suggested using a count of 10 ∞ 10 9 /L as the threshold. 18 The accepted threshold for unstable nonbleeding patients is 20 ∞ 10 9 /L. For patients undergoing simple, noncomplex, surgical, or other procedures, the recommendation is to maintain the platelet count at > 50 ∞ 10 9 /L and > 100 ∞ 10 9 /L for complex surgical cases, such as open heart or neurosurgery. These levels are recommended during the procedure and for a brief period (1–3 days) following the procedure. 19 In case of microvascular bleeding unresponsive to other therapies in patients with a recent history of taking aspirin or other platelet inhibitors, clinicians should suspect platelet dysfunction and consider platelet transfusion even at higher platelet counts. 20
Fresh frozen plasma (FFP) and cryoprecipitate have limited indications. FFP is mainly indicated for replacement of multiple coagulation factor deficiencies following massive hemorrhage. FFP administration is guided by the prothrombin time (PT) and partial thromboplastin time (threshold of 1.5 times the normal control plasma). 21 In the absence of active bleeding, FFP is not indicated in disseminated intravascular coagulation (DIC) or for reversal of warfarin anticoagulation. Some recommend FFP for prevention of bleeding in patients with liver disease and prolonged PT. 22 Elevation of PT alone is not an indication of the need for FFP administration.
Cryoprecipitate is mostly used as a rapid source of fibrinogen in massive hemorrhage with fibrinogen < 1 g/L. Owing to its smaller volume, it can be thawed faster than FFP and used first. However, following transfusion of FFP, if the fibrinogen level remains < 1 g/L, the patient can receive more cryoprecipitate. 21 FFP or cryoprecipitate should not be used for the treatment of single coagulation factor deficiencies with available virus-free fractionated factor. 22
Available Blood Products
A 500 mL unit of whole blood contains approximately 450 mL of blood and has a hematocrit of about 35%, with an expected mean 24-hour red blood cell (RBC) viability of at least 75% after transfusion. 23 Since the plasma is not removed from the blood, in the past, whole blood was primarily used in massive bleeding where volume expansion was desirable, together with an increase in Hb. Currently, whole blood is more commonly fractionated into RBCs (also called packed RBCs), FFP, platelets, and cryoprecipitate, and each component is used when it is specifically indicated. Although component therapy has largely replaced whole blood transfusion, limited use of whole blood is still seen in certain situations, such as component-refractory coagulopathy in cardiac surgery, multifactorial coagulopathy in liver disease, traumatic brain injury, and disasters in which logistics are the limiting factor. Whole blood is also used in massive transfusion (usually > 10 units of blood within 24 hours), 24 especially in military settings, to reduce donor exposure and decrease component-induced coagulopathy while achieving volume resuscitation and improving oxygen delivery. 25
By far the most commonly used blood product is RBCs. After centrifugation and removal of other fractions, RBCs are mixed with specific preservative solutions to a final hematocrit of 60 to 70%. Depending on the preservatives, RBCs can be stored at 4°C for 35 to 42 days prior to use. 23 With this prolonged storage, biochemical changes such as depletion of adenosine triphosphate (ATP) and 2,3-diphosphoglycerate (2,3-, DPG), loss of proteins, loss and peroxidation of membrane phospholipids, and release of potassium, Hb, and other biologically active molecules into extracellular space will occur.26,27 These changes reduce the function and viability of the RBCs and are collectively called “RBC storage lesion.” 27 Transfusion of long-stored RBCs (> 10–14 days) has been linked to increased length of stay and higher rates of mortality, infection (pneumonia), and multiorgan failure in observational studies. Although these are strong associations, controlled trials are necessary for validation. 26
When frozen in cryoprotectant solutions, such as glycerol, RBCs can be stored for years (10 years at –80°C). On thawing, cells should be washed immediately to remove the glycerol. Thawed and deglycerolized RBCs have the same function and viability as fresh RBCs, but owing to an open wash cycle, they should be transfused within 24 hours. 28 The use of a closed wash system to maintain sterility can further extend the storage time of deglycerolized RBCs. 29 Although the long storability of frozen RBCs is an advantage for maintaining stable inventories, complexities, cost, and logistic issues prevent this product from being routinely used. This approach has been mainly limited to preserving inventories of rare blood groups and phenotypes, highly washed RBCs for transfusion-dependent patients, and patients with diverse circulating antibodies and occasionally to storing universally compatible or surplus RBCs. Use of frozen RBCs is expensive, and its use is expected to continue to decline. 29
Blood transfused to immunosuppressed recipients, neonates, and donors’ first-degree relatives is irradiated to inactivate the white blood cells and prevent graft-versus-host disease (GVHD). 30 Both long-term storage and irradiation of RBCs can result in release of potassium, Hb, and other biologically active molecules from RBCs, which can infrequently result in adverse events such as cardiac arrhythmias and/or cardiac arrest. Washing RBCs can remove or reduce these factors and is recommended by some for stored and irradiated RBCs. 31 Washed RBCs should be used in patients with IgA deficiency to prevent rare but devastating anaphylactic transfusion reactions. 32
Following development of leukoreduction filters, use of leukoreduced (or leukodepleted) RBCs has been on the rise in recent years. Many complications related to blood transfusion have been linked to the presence of white blood cells (WBCs). Removal of WBCs is shown to reduce the frequency and severity of non-hemolytic febrile transfusion reactions (NHFTRs), as well as the risk of cytomegalovirus (CMV) transmission, human leukocyte antigen (HLA) alloimmunization, and platelet refractoriness. Other benefits of leukoreduction include reducing the risk of multiorgan dysfunction, mortality, immunomodulation, and infection. Reduced risk of GVHD disease is another potential benefit, but irradiation is the method of choice to prevent this fatal condition. 33 Given the demonstrated and perceived benefits, a number of countries have mandated universal leukoreduction for their blood supply. Studies comparing outcomes before and after universal implementation of leukoreduction have shown marginal reductions in NHFTR, mortality, and antibiotic use. Although a voluntary practice in the United States, most of the blood products currently distributed are leukoreduced. 34
There are two methods for deriving platelets, apheresis, and pooled whole blood (which is subdivided into platelet-rich plasma and buffy coat, based on the preparation method). Both contain 2 1.5 ∞ 10 9 platelets per milliliter. Except in special situations (as mentioned below), there is no evidence supporting the use of one type over another type of platelet, and the choice is usually based on local supply and established practice preferences. 35 Following storage at 4°C, platelets undergo irreversible clustering of surface glycoproteins, resulting in their rapid clearance from circulation after transfusion. Therefore, platelets should be stored at room temperature (20–24°C) to maintain their viability. Room temperature storage makes platelets prone to bacterial growth, with a reported bacterial contamination incidence of 1 in 2,000 to 3,000 products. 35 Platelet-refractory patients who need a human platelet antigen (HPA)- and HLA-matched single donor, neonates with alloimmune thrombocytopenia owing to maternal HPA antibodies, and patients with IgA deficiency require matched single-donor, apheresis-derived platelets. Patients with previous posttransfusion purpura usually respond better to apheresis-derived platelets. 35
All of the coagulation factors are present in FFP in various concentrations. FFP is available from whole blood (recovered FFP) and plasmopheresis. Both types of FFP are clinically equivalent. To reduce the risk of infection transmission in patients likely to receive large volumes of FFP, pathogen-reduced plasma may be used instead. 22 Blood groups should be considered in FFP transfusions, with same-group donors as the first choice. 22 Cryoprecipitate contains fibrinogen, factor VIII, von Willebrand factor, factor XIII, and fibronectin and is derived from FFP cooled to 4þC. 21
Prothrombin complex concentrate is another plasma-derived component containing prothrombin, factor IX, factor X, and usually factor VII. It may be beneficial in patients with persistent massive bleeding and known deficiencies of prothrombin complex factor (eg, warfarin therapy and vitamin K deficiency), but the benefits should be carefully weighed against the risks of thromboembolic disease and DIC. 21 Albumin can be used as a colloid for plasma volume expansion in management of hypovolemia. 21 Single coagulation factors are also available for treatment of specific factor deficiencies, such as hemophilia, but these factors are rarely indicated in patients with normal baseline coagulation. One particular factor, recombinant activated factor VII (rFVIIa), is currently approved for management of hemophilia A or B with inhibitors, inherited FVII deficiency, acquired hemophilia, and refractory Glanzmann thrombasthenia. 21 rFVIIa is increasingly used in treatment of massive bleeding in various surgical scenarios in nonhemophilia cases and is recommended in cardiac, thoracic aortic, and spinal surgery; hepatic resection; hysterectomy; and postpartum bleeding only when significant clotting factor replacement has failed. 36
Risks of Transfusion
Early in the twentieth century, blood transfusions frequently resulted in serious complications prior to the discovery of blood groups. Subsequently, transfusion became a lifesaving procedure, especially in combat situations during the world wars, but also introduced other complications, including transfusion-induced jaundice. The result was the implementation of donor screening measures, and blood safety greatly improved. Ironically, ABO incompatibility and infections have remained rare but significant concerns, and the list of infectious and noninfectious risks of transfusion has unfortunately grown. 37
Blood is routinely tested serologically in the United States for human immunodeficiency virus (HIV) types 1 and 2, hepatitis B virus (HBV), hepatitis C virus (HCV), human T-cell lymphotropic virus (HTLV) types 1 and 2, and syphilis. 38 Blood donors in the United States now undergo screening for Chagas disease as well. 39 During the window period, infections can go undetected with serologic tests. Nucleic acid amplification testing is more sensitive, provides a much shorter window period, and detects West Nile virus ribonucleic acid. It is also used by some centers for HBV DNA detection, as well as in incidental cases of HIV-1 and HCV. Platelet preparations are also routinely checked for bacterial contamination. 38
Thanks to extensive testing, the frequency of acquiring these infections through transfusion is extremely low but is not completely eliminated owing to the window period. Risks are estimated based on mathematical methods and vary across references. Current risk estimates in the United States are less than 1 in 1,500,000 units for HIV-1, less than 1 in 390,000 units for HCV, less than 1 in 200,000 units for HBV, 1 in 1,900,000 units for HTLV 1 and 2, and practically 0 for HIV-2 and West Nile virus. As stated previously, the risk of bacterial infection from platelets is significantly higher.38,40
Of special concern is transmission of newly emerging agents and agents for which there are no routine tests, including prions, hepatitis G virus, TT virus, and human herpesvirus 8.17,23 Rare cases of transfusion-transmitted variant Creutzfeldt-Jakob disease have been documented. 41 CMV can be transmitted through transfusion but rarely results in clinical disease unless introduced to immunocompromised patients who require leukoreduced blood from seronegative donors. 40 Transmission of parasitic infections (babesiosis, leishmaniasis, malaria, and toxoplasmosis) is possible through transfusion but is extremely rare in the United States. 17
Noninfectious complications of transfusion are much more common and important to note. They can be grouped into early-onset (within hours) and late-onset (within days or months after transfusion). Major early-onset complications include NHFTR (0.1 to 2.0% of transfusions; less frequent in leukoreduced components); transfusion-associated circulatory overload (1 in 2,000 RBC transfusions; fatal events 1 per 4.5 million); hemolysis of incompatible RBCs (< 1 in 13,000 RBC transfusions; fatal events in < 1 per 1.3 million); hemolysis from incompatible plasma (1 in 46,000 platelet transfusions; fatal events 1 per 8 million); transfusion-related acute lung injury (probably 1 in 1,000 transfusions but likely to be underreported; fatal events 1 per 3 million); mild allergic reactions such as urticaria (< 5.0% of platelet and 0.5% of RBC transfusions); severe allergic or anaphylactic reactions (1 in 25,000 RBCs, 1 in 2,000 platelet transfusions); and electrolyte and coagulation abnormalities.37,42,43
Late-onset complications of transfusion are even more frequent. Complications related to RBC- antibody formation may occur in more than 10% of patients and include delayed hemolytic transfusion reactions, hyperhemolysis syndrome, hemolytic disease of the fetus and newborn, and difficult crossmatching interfering with future transfusions. 42 Iron overload occurs most often in chronically transfused patients. 42 Immunosuppression or modulation occurs with varying degrees in almost all transfusions and is possibly associated with increased risk of infection, cancer recurrence, and mortality.42,44 Complications related to the formation of HLA antibodies occur in more than 10% of transfusion recipients and include platelet transfusion refractoriness, neonatal alloimmune thrombocytopenia, and difficulty matching for organ transplantation. 42 Complications related to formation of platelet antibodies include platelet transfusion refractoriness, neonatal alloimmune thrombocytopenia, and posttransfusion purpura. 42 Finally, GVHD is a rare but potentially fatal complication of transfusion, especially in immunocompromised patients and recipients of directed donations from relatives. 45
Blood Conservation in Surgery
Transfusion has been associated with negative and unfavorable outcomes, particularly in postoperative infection, systemic inflammatory response syndrome, multiorgan failure, and mortality. 43 Shortage of blood, its increasing cost owing to extensive testing, and logistics are issues plaguing allogeneic blood transfusions. 46 Together with evidence supporting the tolerability of lower Hb levels, these issues are fueling initiatives to conserve blood and limit its use to the most needy patients.
Blood conservation involves using a combination of medications, specific devices, and medical and surgical techniques by an interdisciplinary team committed to avoiding allogeneic blood transfusion.
47
General principles of blood conservation in medical and surgical settings are as follows48–50:
Devising an individual plan of care to minimize blood loss according to clinical management and anticipated procedures for each patient Using a multidisciplinary treatment approach with a combination of techniques to achieve blood conservation Anticipating and addressing complications; the lead clinician should provide proactive management Modifying routine practices based on clinical judgment when appropriate Screening, investigating, and treating anemia, preferably before surgery Minimizing iatrogenic blood loss; including preoperative and postoperative phlebotomies and intraoperative blood loss Implementing a restrictive transfusion strategy as discussed under the Transfusion Triggers section; “tolerance” to anemia (or acceptance of lower Hb) should be implemented by maintaining normovolemia; and transfusion should be based on recommended criteria (see Table 1) Limiting or avoiding preoperative use of anticoagulant and antiplatelet agents Consulting specialists with experience in blood conservation at an early stage if physiologic deterioration or complications occur Rapidly controlling hemorrhage and transferring to an appropriate center if necessary; an emergency management plan should be established in advance
Blood conservation begins in the preoperative period and spans intraoperative and postoperative periods (Figure 1). Preoperative blood management begins by obtaining a comprehensive history and physical examination. Special attention should be given to medication history and any personal or familial history of bleeding disorders.
51
Preadmission testing should be done well ahead of surgery (eg, 30 days) to allow adequate time for identification, evaluation, and management of anemia and its underlying causes and reassessment of anticoagulation and antiplatelet therapies if necessary.47,51 Preoperative anemia is a major risk factor of perioperative transfusion. Moreover, anemia assessment provides added benefit to patients as an inexpensive screening tool for possible underlying comorbidities, including colon cancer and renal dysfunction.
52
Overview of perioperative blood conservation strategies.
50
Modified from Shander and Goodnough (2006).
If anemia (Hb < 13 g/dL in men, < 12 g/dL in women 53 ) is detected, mean corpuscular volume (MCV) should be used to guide the next step. If the MCV is > 100 fL, serum vitamin B12 and folic acid levels should be obtained and further hematologic evaluation should be considered. If the MCV is < 80 fL and iron deficiency is evident (ferritin < 12 mg/mL or transferrin saturation < 15%), the patient should receive iron supplementation and be considered for gastrointestinal evaluation. If the MCV is 80 to 100 fL or < 80 fL without iron deficiency, renal function should be assessed. If the creatinine level is normal and the reticulocyte count is reduced, the patient should be evaluated for anemia of chronic disease. If the reticulocyte count is normal, blood loss and hemolysis should be ruled out. 51
Preoperative increase in RBC mass with erythropoiesis-stimulating agents (ESAs) is an effective measure to avoid transfusion in anemic patients. Since normal iron storage may not be sufficient to support the increased hematopoiesis (a condition known as relative iron deficiency), adequate iron supplementation, folate, and vitamin B12 should be given concomitantly. 54 Following this therapy, equivalents of 1 and 5 blood units are produced in 7 and 28 days, respectively; therefore, to achieve a target of 3 to 5 blood units by the time of surgery to avoid transfusion in complex procedures, a 3- to 4-week treatment period is usually required. 55 Although preoperative use of ESAs is approved for anemic patients, there are recent reports of possible complications (thrombotic events and hypertension). The US Food and Drug Administration recommends using ESAs at the lowest possible dose required to avoid transfusion and withholding ESAs if Hb levels exceed 12 g/dL. 56
Preoperative autologous donation (PAD) usually involves collection of 1 unit of the patient's own blood per week for a 4-week period prior to the surgery. This autologous blood is stored and reinfused to the patient perioperatively if a transfusion is required. 49 Patients should have normal Hb levels to participate in PAD, and many patients undergoing PAD receive ESA therapy and iron to avoid becoming anemic at the time of surgery as a result of aggressive phlebotomies. 49 Despite potential benefits, banked PAD blood shares the same risk of clerical errors with allogeneic transfusion and can result in RBC storage lesion with loss of 2,3-DPG and ATP, reducing the effectiveness and life span of RBCs. Moreover, the procedure is time-consuming and costly and might not avoid exposure to allogeneic blood if patients become anemic owing to the process. Finally, many units of PAD blood are not used perioperatively and are eventually discarded, further undermining the cost-effectiveness of this procedure. As a result, use of PAD is declining.47,50
Blood conservation can be achieved intraoperatively through various techniques and practices. Every effort should be made to reduce surgical blood loss through refined operative techniques and meticulous hemostasis. Various sutures and clips, electrocautery, and coagulator devices have shown varying degrees of ease of use and success in establishing hemostasis. 57 Fibrin sealants have been used effectively for hemostasis in vascular surgery and other procedures, and other hemostatic agents and tissue adhesives are being developed to provide better hemostasis in surgery. 58 Positioning of the patient to elevate the field of surgery, use of tourniquets, local vasoconstrictors, and pharmacologic agents are other effective conservation methods. 47 Finally, anesthetic techniques and practices including controlled hypotension, maintenance of normovolemia, avoidance of hypothermia, blood cell salvage, and acute normovolemic hemodilution (ANH) are effective intraoperative strategies used in blood conservation. 49
In ANH, immediately before or after the induction of anesthesia, a portion of the patient's blood is removed and replaced by colloid or crystalloid solutions to maintain normovolemia while inducing acute anemia. During the surgery, any shed and lost blood is diluted; thus, the actual amount of RBC and plasma loss is decreased. The patient's blood is returned when a transfusion trigger is reached or at termination of surgery, providing a fresh supply of blood and clotting factors. In theory, this practice should reduce the need for allogeneic transfusion. 59 ANH has several advantages over PAD in terms of time, cost, and convenience. It can be done in both elective and emergency procedures, and since the ANH blood units are collected in the operating room and kept by the patient's bed, administrative costs and risks of clerical errors are almost completely eliminated. 59 Although studies have shown mixed results on the efficacy of ANH in reducing allogeneic transfusion, 60 it has been suggested that ANH would be effective in reducing transfusion only in surgeries with significant blood loss. 61 ANH remains a low-cost, useful tool in the armamentarium of blood conservation.
Recovery of the patient's shed blood from the surgical wound and sponges and reinfusion of the blood after washing and filtering is known as cell salvage. This procedure provides another valuable blood conservation technique. Similar to ANH, this technique is most effective in procedures with large anticipated blood loss.47,50 There are concerns about the risk of infection, loss of coagulation factors, hemolysis, and reinfusion of tumor cells in oncology cases or amniotic fluid in obstetrics cases with the use of cell salvage. 50 Although hotly debated, the incorporation and use of leukoreduction filters can reduce some of these risks. 47 Although the potential risk of adverse events is low, cell salvage appears to be effective in reducing the need for allogeneic blood transfusion. 62
Numerous pharmacologic hemostatic agents have been evaluated for intraoperative blood conservation. Aprotinin and lysine analogs (e-aminocaproic acid and tranexamic acid) are commonly used antifibrinolytic agents. When fibrinolysis contributes to bleeding, these agents can promote hemostasis and reduce transfusion requirements. 47 Although aprotinin is generally more effective in this regard, recent reports have raised concerns regarding its safety (higher risk of renal failure and myocardial infarction in retrospective studies). 63 The low cost and acceptable safety profile of lysine analogues make them an efficacious option in blood conservation. 47 Desmopressin is a vasopressin analogue, mainly used to improve hemostasis in hemophilia and platelet disorders. Although some evidence suggests a positive role in blood conservation in cardiac surgeries, most of the studies have found little effect on transfusion requirement, although an increased risk of myocardial infarction has been reported. Thus, its routine use in blood conservation is not supported. 64 Another agent being increasingly used to manage massive bleeding in various surgical scenarios in nonhemophilia cases is rFVIIa, but studies have conflicting findings on its effectiveness in reducing surgical blood loss and transfusion requirements. With safety concerns looming, further studies are required to confirm its role in blood conservation.36,47
During the postoperative period, patients should be monitored for persistent bleeding, and if present, every effort, including reexploration, should be made to stop the bleeding. 49 Cell salvage and reinfusion of washed cells can continue in the postoperative period if required. 65 Blood pressure and body temperature should be kept within normal and/or acceptable ranges. 49 If detected prior to the surgery, treatment of anemia and underlying causes should continue. Newly diagnosed anemia should be treated using a combination of ESAs, iron, folate, and vitamin B12 as appropriate. 65 As recommended in the preoperative period, phlebotomies should be kept to a minimum and anticoagulation or antiplatelet agents should be used sparingly. 49 The same restrictive transfusion strategy, triggers, and considerations listed in Table 1 should also be used in the postoperative period.
It is estimated that as a result of postoperative blood salvage and restricted phlebotomy, 1 blood unit is saved as a result of each activity. Use of restrictive transfusion triggers, PAD, ANH, intraoperative blood salvage, and refined operative techniques or meticulous hemostasis can save 1 or more blood units each. Finally, proper use of ESAs well ahead of surgery can save 2 units of blood. 48 Taken together with risks and costs of allogeneic blood transfusions, these estimates clearly demonstrate the significance and value of blood conservation techniques. It is no surprise that more and more hospitals are adopting blood conservation as their routine practice. Although blood conservation is here to stay and can become an integral part of every patient's care, it is a rapidly evolving field.
One area of active research, artificial oxygen carriers and blood substitutes, possesses enormous potential for the future of blood conservation, with the possibility of replacing allogeneic transfusions in a variety of clinical situations. 66 We excitedly await expansion of our understanding of molecular, physiologic, and clinical aspects of hematopoiesis, circulatory response, coagulation enigmas, artificial oxygen carriers, and the impact of anemia on organ function.