
Abstract
We investigated the efficacy of Xpert (Abbott Vascular, Abbott Park, IL) nitinol stents for the treatment of infrapopliteal lesions in patients with Critical Limb Ischemia (CLI). Between May 2005 and November 2007, 94 CLI patients (70 male, mean age 73.5 years) received 134 Xpert stents in 102 limbs. Seventy-nine patients (71.2%) were scored as Rutherford Category 4, 31 patients (27.9%) as Category 5 and 1 patient (0.9%) as Category 6. Primary endpoint of this study was defined as 2-year duplex derived primary patency. Secondary endpoints were 2-year limb salvage rate and the absence of reintervention after the index procedure. Kaplan Meier analysis reported 2-year primary patency and limb salvage rates of 54.4% and 90.8%, respectively. Stratification by lesion location did not reveal any significant differences in 2-year primary patency rates in proximal and distal below the knee lesions. Our results suggest that treatment with nitinol Xpert stents can be considered effective for treating CLI patients, with satisfying patency outcome.
Recent advances in endovascular technologies with new guidewires, low-profile peripheral balloons, and dedicated stents for below the knee (BTK) use have generated an increasing interest in interventional treatment of infragenicular lesions in patients with critical limb ischemia (CLI). The primary goal in these cases is aimed at restoring straight in-line blood flow to the foot in at least one vessel. 1 So far, excellent limb salvage rates after percutaneous transluminal angioplasty (PTA) have been confirmed by several publications, giving limb salvage rates of above 90%. 2–4 However, the published primary patency rates are less satisfying, although, in general, the treatment of complex longer lesions has a worse prognosis. 2,3,5–7 Reluctance in implanting stents in these small-diameter vessels has been attributed to concerns regarding early thrombosis and late luminal loss from intimal hyperplasia. As a result, stent implantation is generally reserved for cases with a suboptimal outcome after PTA (ie, > 50% residual stenosis or flow-limiting dissection). The recent development of self-expanding nitinol stents for BTK use intends to maintain the flow dynamics in the infrapopliteal arteries, lower lumen loss, and improve patency rates. Their low vessel to wall ratio can avert intimal hyperproliferation following implantation, and routine use following infragenicular angioplasty may improve outcome.
Initial experience showed encouraging results in primary patency and clinical outcome after 6 months. 8,9 We recently reported 1-year angiographic and clinical results of 47 patients with CLI treated with a nitinol self-expanding stent system (Xpert, Abbott Vascular, Abbott Park, IL) specifically designed for BTK use. 10 The 1-year angiographic primary patency and limb salvage rates were 76.3% and 95.9%, respectively. We followed up the 47 patients from our previous study until 2 years after intervention for morphologic, clinical, and hemodynamic outcome by duplex ultrasonography and clinically driven target vessel revascularization. We included 47 more patients (total 94) treated subsequently using the same inclusion criteria to assess the 2-year efficacy of the Xpert nitinol stent in the treatment of CLI patients.
Methods
Between May 2005 and November 2007, 102 limbs were treated in 94 patients with CLI (70 men; mean age 73.5 years). One hundred eleven infragenicular arterial lesions were treated by primary stent implantation, and the data were entered into a registry. This prospective study was conducted in two institutions (AZ-St Blasius Hospital, Dendermonde, and Imelda Hospital, Bonheiden, Belgium), and its protocol was approved by the Ethics Committee of the two participating hospitals. All patients gave written informed consent prior to the procedure.
The study included 94 patients with CLI (Rutherford category 4–6) and angiographically proven stenotic (> 50%) or occlusive disease of the infrageniculate vessels, with a maximum lesion length of 10 cm and a reference vessel diameter of 2.0 to 4.5 mm. An overview of the inclusion and exclusion criteria is given in Table 1. The baseline clinical data, including Rutherford categorization and common comorbidity incidence, are given in Table 2.
Inclusion and Exclusion Criteria
PTA = percutaneous transluminal angioplasty.
Baseline Clinical Data
BMI = body mass index; Cr = Creatinine.
Technique
Typically, access was obtained in a retrograde fashion via the contralateral common femoral artery. A 6F sheath (Destination, Terumo, Tokyo, Japan) 90 cm in length was placed with the tip in the proximal or midpopliteal artery. After obtaining appropriate angiographic views of the popliteal and tibial vessels, lesions were crossed intraluminally. The guidewire of choice for standard lesion passage was a stiff 0.014- or 0.018-inch hydrophilic wire, often with the support of a 4F to 5F multipurpose or glide catheter. Reestablishment of one named vessel with in-line flow to the foot was the primary goal. In diabetic patients, two-vessel flow to the foot was sometimes necessary owing to poor pedal collateral circulation. Primary stenting with one or two Xpert stents was achieved, followed by postdilation with a balloon adjusted to the vessel size to avoid overdilation. Coexisting femoropopliteal lesions were treated with balloon angioplasty and nitinol stent placement when necessary.
Device
The device used in the study was the Xpert Self-Expanding Stent System (Abbott Vascular). This nitinol stent is available in diameters ranging from 3 to 8 mm and lengths from 20 to 80 mm. The diameter of stents used in BTK procedures is usually up to 6 mm. The 4F introducer sheath–compatible nitinol stent system is specially designed for small vessel application. Once implanted, the stent offers good flexibility and low straightening force to ensure wall apposition and delivers equivalent radial force. The system is 0.018-inch-wire compatible and comes in 90 cm and 135 cm catheter lengths.
Anticoagulation
Patients were given 100 mg/d of aspirin and clopidogrel 75 mg daily for 4 days or one loading dose of 300 mg the day before the procedure. Unfractionated heparin (150 IU/kg) was given during the procedure. The postprocedure antithrombotic regimen consisted of clopidogrel 75 mg daily for at least 1 month and aspirin 100 mg daily, indefinitely. Nadroparin (0.6 mL) was administered daily for 3 weeks.
Follow-Up
Measurements on pre- and postprocedural angiographic images were performed using on-site x-ray analysis software (Advantage Workstation 4.2, General Electric Medical Systems). The minimum lumen diameter (MLD) in millimeters and the stenosis rate (%) for each lesion before and after the procedure were calculated. Clinical follow-up was scheduled at 1, 6, 12, 18, and 24 months, according to an established protocol for longitudinal postoperative care of CLI patients. During the follow-up visits, the patency of the treated lesion areas was assessed based on duplex ultrasonography peak velocity ratios (PVRs). Clinical assessment included classification according to the Rutherford categories and evaluation of wound healing status in case of ischemic ulcers and minor amputations. Patients with clinical deterioration (≥ one Rutherford category) and/or restenosis on duplex ultrasonography (PVR ≥ 2.4) were scheduled for angiographic control. Any endovascular or surgical BTK reintervention was recorded. The initial 47 patients had an additional angiographic control at the 1-year follow-up (the results were reported in a previous report). 10
End Points
The primary end point of the study was the loss of duplex patency 2 years following the procedure. The patency of the treated areas was assessed based on duplex PVRs. PVR is the ratio of the peak systolic velocity (PSV) at the lesion segment over the PSV at the proximal reference vessel. Patients not receiving any endovascular or surgical BTK reintervention and not exhibiting significant restenosis on duplex ultrasonography (PVR ≥ 2.4) were regarded as having primary patency. The secondary end points were the 2-year limb salvage (defined as a lack of major amputation) and the absence of reintervention after the index procedure. Serious adverse events, defined as death, amputation, and the need for revascularization, were recorded according to standard classifications. 11
Statistical Analysis
Life tables were calculated using the Kaplan-Meier estimate method for the follow-up data of the entire patient group and for a period starting on the date of the procedure through to the most recent follow-up visit. To define independent prognostic factors associated with the studied covariates, stepwise regression analysis was performed with use of the Cox proportional hazards regression model. The log-rank test was performed to compare the different modalities. A p value < .05 was considered to indicate statistical significance. All calculations were performed using MedCalc (Medcalc Software, Mariekerke, Belgium) statistical software version 9.2.0.1.
Results
Successful stent implantation was performed in all lesions without periprocedural complications. The mean operating time was 62 minutes (range 20–200 minutes). A mean of 120 mL (range 45–320 mL) contrast dosage was injected, with a mean fluoroscopy time of 14 minutes (range 1–60 minutes). One hundred thirty-four Xpert nitinol stents were implanted in 111 lesions. The mean reference vessel diameter was 3.45 mm (range 2.0–4.5 mm). The mean preoperative degree of stenosis was 88.7% (range 50–100%), and the mean lesion length was 33.2 mm (range 6–100 mm). Thirty-seven occlusions (33.4%) and 74 stenoses (66.6%) were treated. Of the 111 lesions treated, 84 (75.6%) were in the proximal portion of the arteries and 17 (15.3%) in the mid- or distal section. Calcification, dissection, ulceration, or thrombus at the lesion site was found in 59 (53.2%), 4 (3.6%), 1 (0.9%), and 12 (10.8%), respectively. Lesion location distribution over the popliteal artery (P3), tibiofibular trunk, anterior tibial artery, peroneal artery, and posterior tibial artery was 12 (10.8%), 26 (23.4%), 36 (32.4%), 20 (18%), and 17 (15.3%), respectively. Forty-six patients (48.9%) were treated for concurrent inflow occlusive disease (femoropopliteal lesions). One hundred thirty-four Xpert nitinol stents with a mean diameter of 4.48 mm (range 3.0–6.0 mm) were implanted. The mean stented length was 41.77 mm (range 20–100 mm). An overview of the different stent sizes is given in Table 3.
Overview of Xpert Stent Sizes
After 2 years, data could be collected for 69 of 111 lesions (62%) in 60 of 102 (58.8%) limbs. The mean MLD before the procedure was 0.47 mm (range 0–2.25 mm) and following the procedure was 4.08 mm (range 2––6 mm), corresponding to a mean stenosis rate of 88.7% and 4.05%, respectively. Kaplan-Meier estimate showed a 2-year survival rate of 71.9% (Figure 1). During follow-up, there were 26 deaths, but none could be attributed to the interventional treatment. Two-year primary patency, secondary patency, and limb salvage rates (%[± standard error]) were 54.4% (± 6.0), 82.2 (± 4.4), and 90.8% (± 3.5), respectively, according to Kaplan-Meier estimates (Figure 2, Figure 3, and Figure 4). Reinterventions were required in 25 limbs (41.7%) and included an angioplasty of the site of restenosis or occlusion in all cases. Freedom from major surgery was 94.5% (± 2.4) (Figure 5).
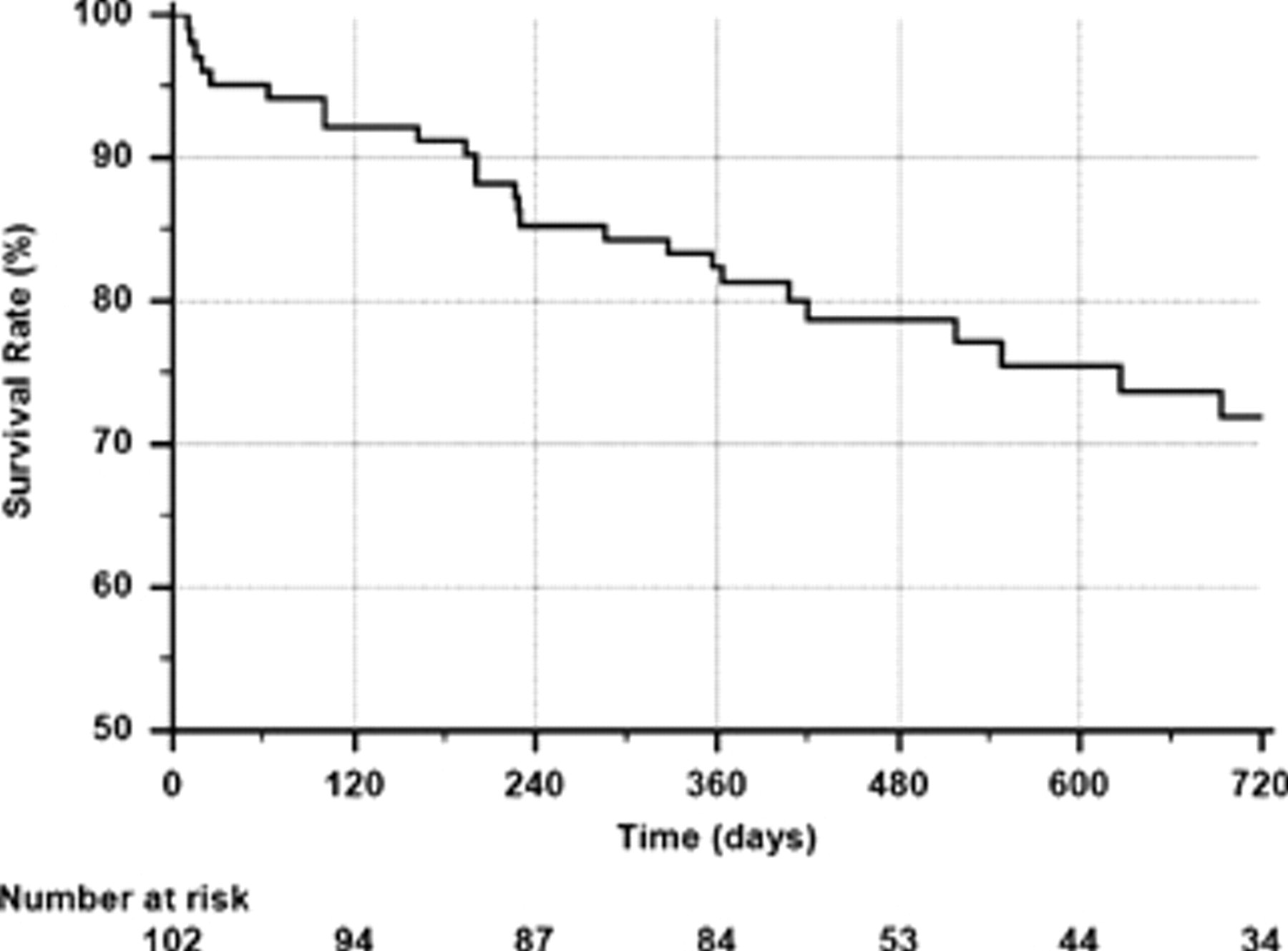
Kaplan-Meier estimate of survival.

Kaplan-Meier estimate of primary patency.

Kaplan-Meier estimate of secondary patency.
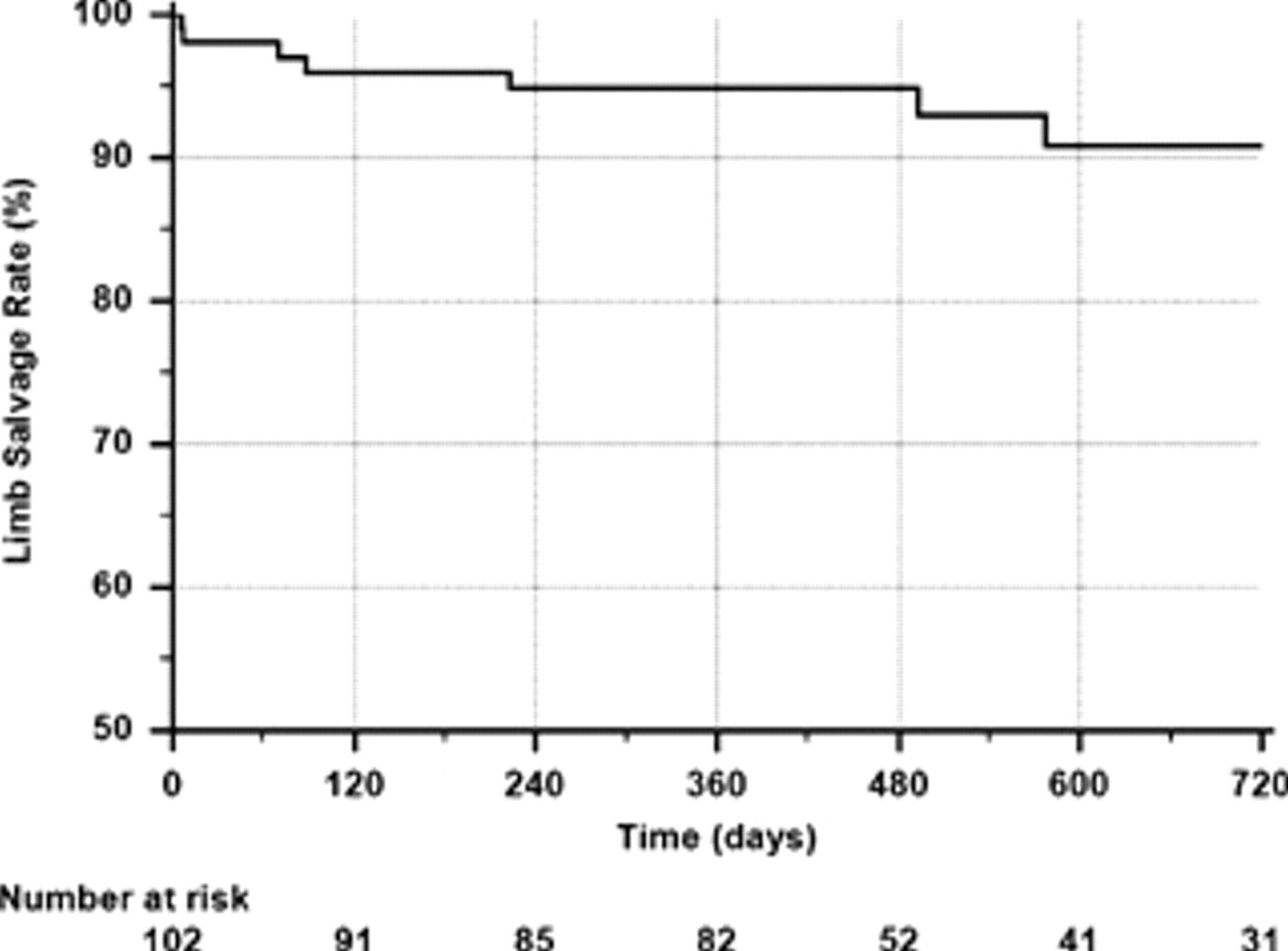
Kaplan-Meier estimate of limb salvage.
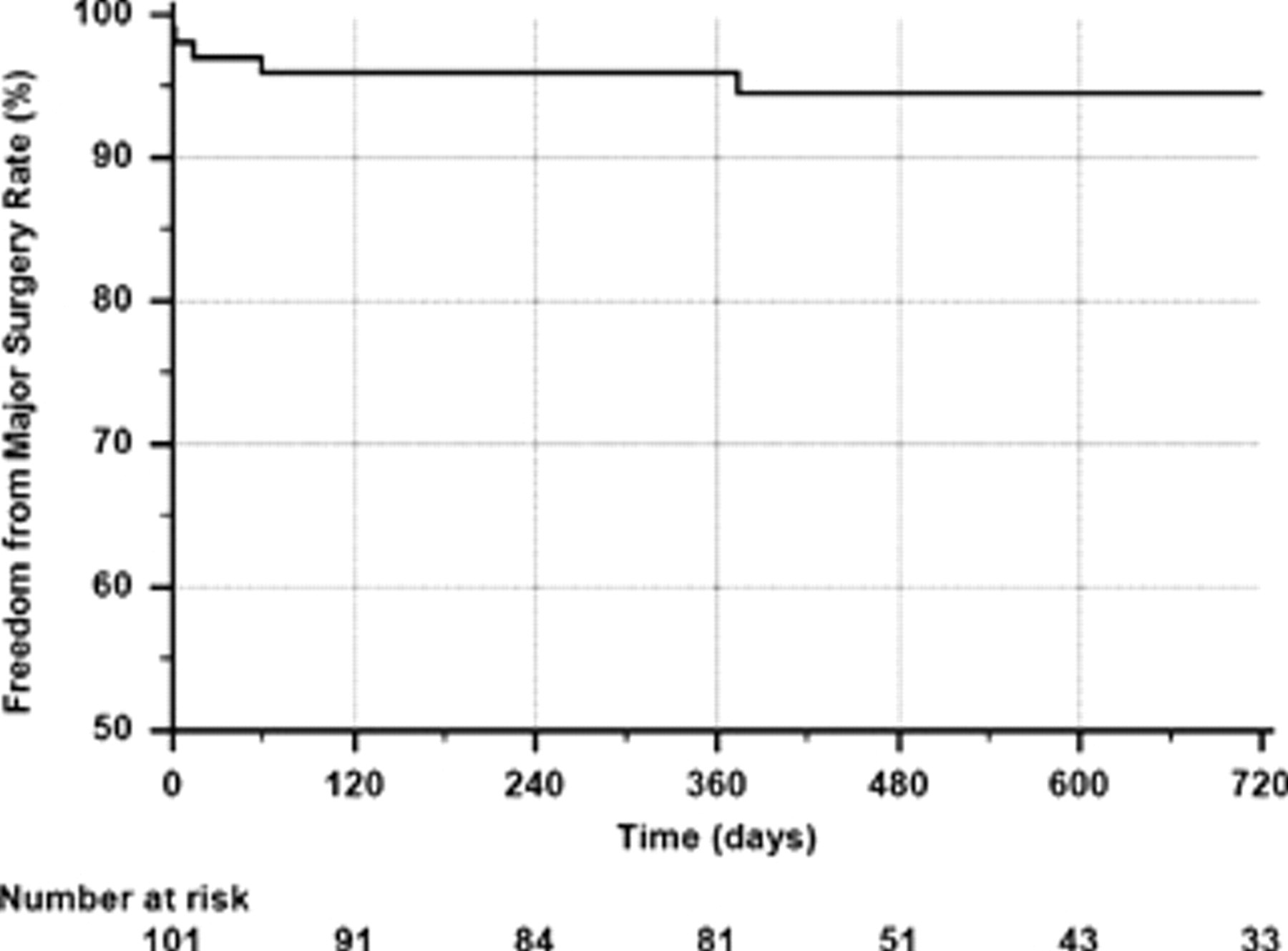
Kaplan-Meier estimate of freedom from major surgery.
Stratification by lesion location revealed no significant difference in 2-year primary patency rates in proximal and distal BTK lesions (56.8% vs 52.3%; p = .2) (Figure 6). Cox proportional hazards regression adjustment for diabetes, obesity, renal insufficiency, smoking, lesion calcification, initial lesion grade, lesion position, number of runoff vessels, and length of stent used identified no independent predictive factor for primary patency. Cox proportional hazards regression analysis for the same covariates demonstrated lesion position as the only independent predictive factor for limb salvage. Patients with proximally located lesions had higher limb salvage rates at 2 years (95.1% vs 81.1%; p = .0317) (Figure 7).
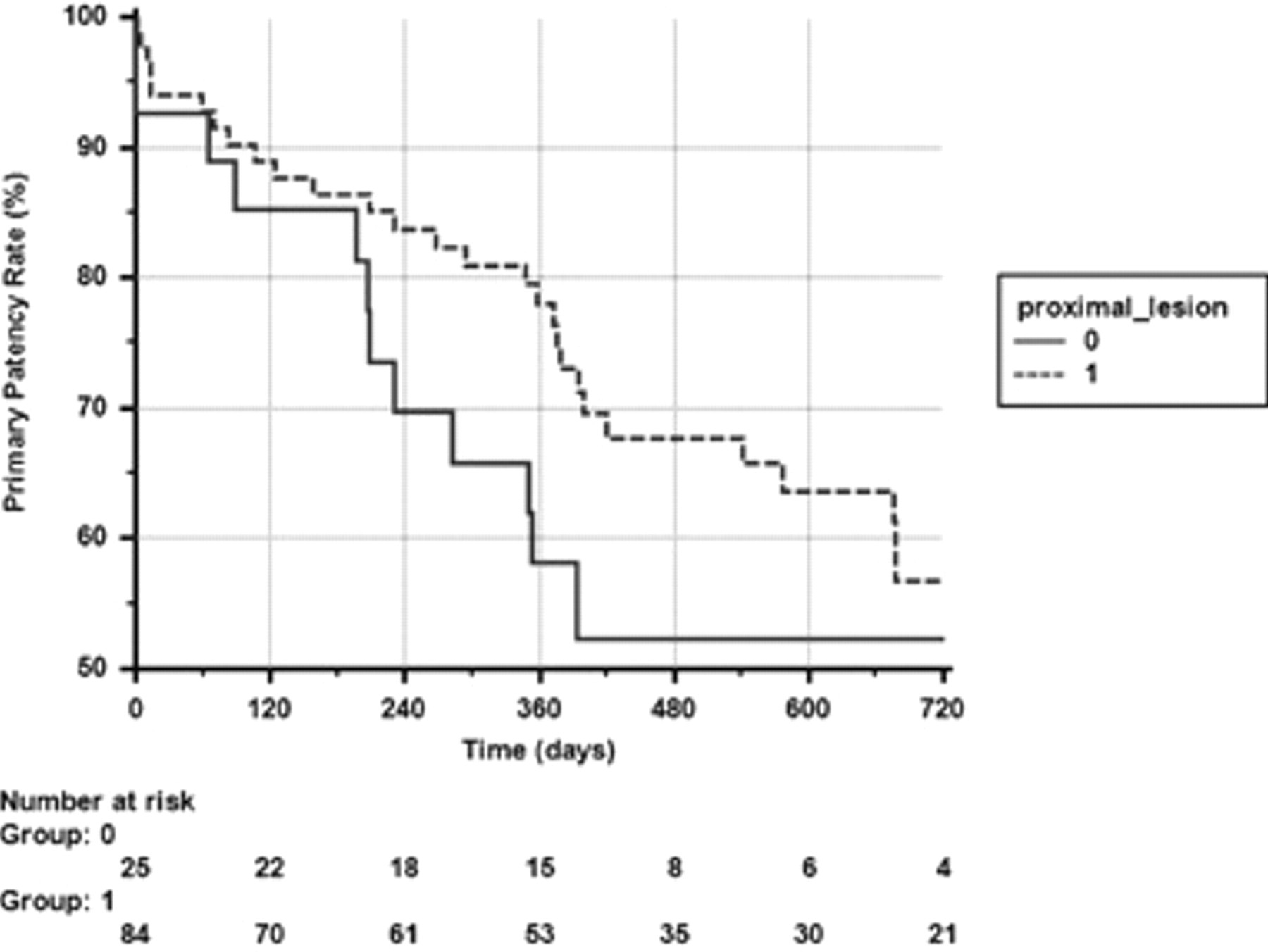
Kaplan-Meier curves by lesion location revealed no significant difference in 2-year primary patency rates in proximal and distal below the knee lesions.
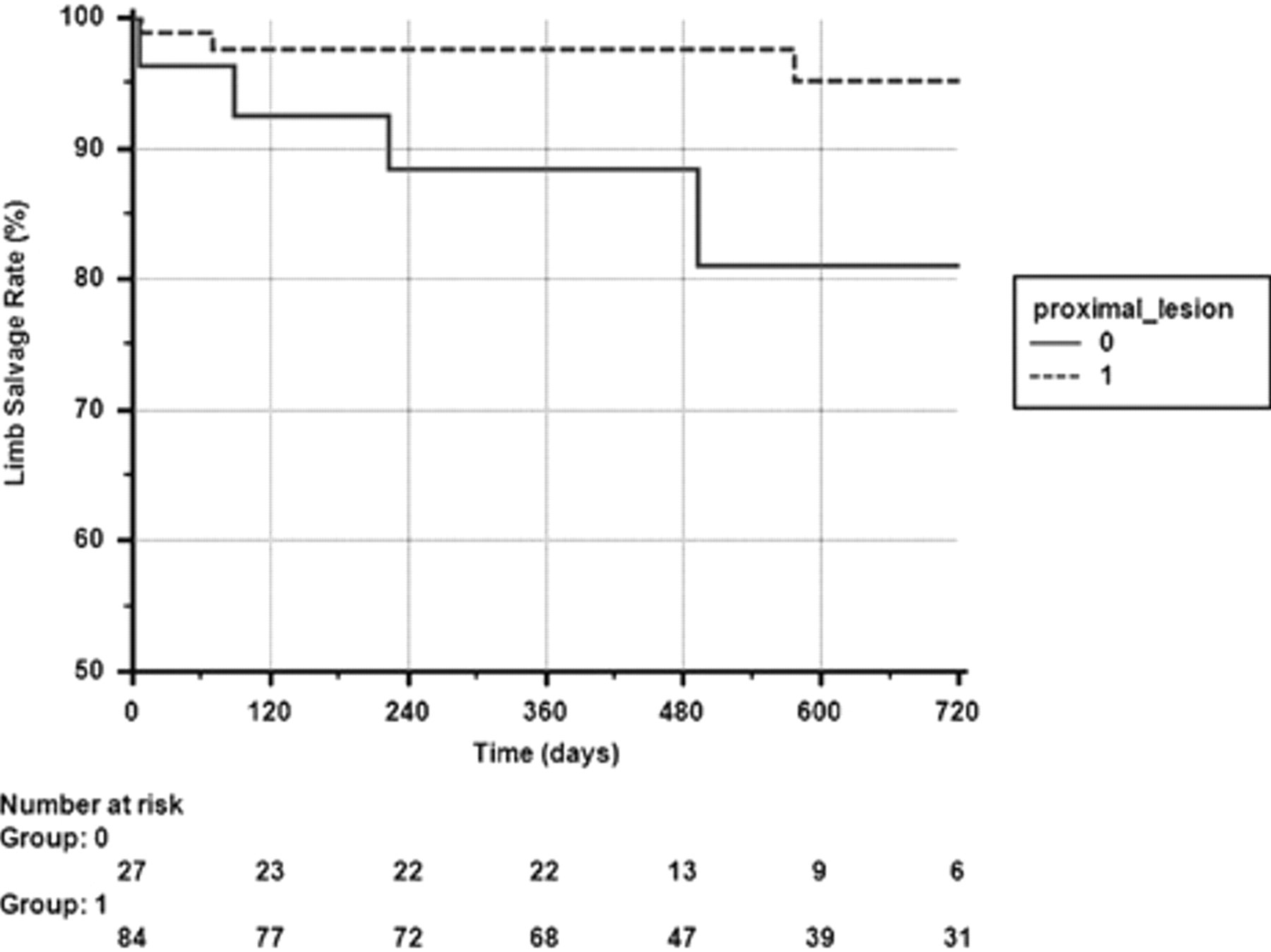
Kaplan-Meier estimates of limb salvage rates in patients with proximal and distal lesions.
Discussion
CLI consumes a considerable amount of health care resources, and the most current treatments are still characterized by high rates of primary amputations, multiple reinterventions, and a high rate of procedure-related complications. 12 It is possible that the problem will be even more prominent in the future owing to the aging population and the increasing incidence of diabetes. CLI-associated amputations cause significant mortality, impart important social and physical limitations, and require extensive resources for rehabilitation. 13 It would be more prudent to deploy such resources in an aggressive approach to salvage affected limbs in CLI patients.
This is the first report of midterm patency and clinical outcome for BTK lesions treated with a self-expanding nitinol stent in a large cohort of CLI patients. These encouraging results further support the growing opinion that the endovascular approach may be the primary treatment for CLI, employed prior to surgery, as happens in our current practice. In favor of a more liberal application of percutaneous revascularization techniques in CLI patients are the results of the BASIL trial (Bypass versus Angioplasty in Severe Ischemia of the Leg). 14 The investigators of this randomized controlled study demonstrated similar outcomes between endovascular therapy and bypass surgery in selected patients with CLI up to 2 years following treatment and the reduced cost of the endovascular approach. Arguments in favor of the endovascular approach include (1) the minimally invasive nature of the interventions, (2) the safe application in a cohort of physiologically compromised patients with many comorbidities, (3) the reduced hospitalization time and potential reduction in the cost of treatment, (4) the preservation of surgical options if failure in the future necessitates bypass, and (5) the application of the procedure in patients who are poor candidates for traditional surgical bypass (eg, no available vein conduits, absent distal target vessels). 2–4,6,15–18
A recent meta-analysis that assessed the long-term outcome after popliteal-to-distal bypass grafting in CLI patients demonstrated 2-year primary patency, secondary patency, and limb salvage rates of 76.8%, 81.6%, and 85.2%, respectively. 19 The durability of infragenicular interventions using the Xpert stent in the present study (2-year primary patency of 54.9%) was limited compared with bypass surgery. The lower primary patency rate may be associated with a higher risk of intimal hyperplasia. But, typically, limb salvage is considered to be the most vital end point in CLI patients, whereas patency seems to be less important. The clinical benefit of the endovascular approach was very gratifying (a 2-year limb salvage rate of 91.8% compared with 85.2% with popliteal-to-distal bypass grafting). This is probably not a significant difference and perhaps can partially be attributed to the higher proportion of patients with tissue loss included in this meta-analysis; however, it also implies that the loss of patency following endovascular treatment can be easily managed with repeated intraluminal interventions. In the current report, 41.7% of the patients had secondary reinterventions, consisting of angioplasties of restenosed or occluded treated lesions. The very high secondary patency rate demonstrated in this study (82.2% at 2 years) represents an advantage over the surgical approach. Although endovascular reintervention is usually a simple and safe procedure, repeat bypass grafting may be troublesome and not always feasible.
PTA in crural lesions has produced heterogeneous results, with patency rates for infrapopliteal lesions ranging between 40 and 78% at 2 years. 2,5,20,21 Recent reports showed that the results of routine stenting following an uncomplicated angioplasty are superior to those of PTA alone. 3,5 It is possible that stent implantation overcomes the early vessel recoil, negative remodeling, and consequent loss of lumen after PTA alone. 22 Rand and colleagues demonstrated in an angiographic controlled study that the outcome after stenting, using a stent with a passive coating, is superior to that after PTA alone in infrapopliteal vessels. 5 On the basis of these data and the very encouraging midterm results of the present study, it seems that angioplasty and stenting may achieve superior outcome compared with angioplasty without stenting in the BTK vascular bed, and this concept should be validated in well-designed, randomized, controlled studies.
A major area of concern related to stent treatment in peripheral arteries is the potential for stent compression or stent fracture. It was reported recently that balloon-expandable stents placed in the infragenicular arteries may be prone to fractures. 23 Similar to the findings in the superficial femoral artery (SFA), where a direct link between stent fractures and lesion reocclusions has been found, the fracture-prone nature of balloon-expandable stents could potentially affect long-term outcomes. 24 Our experience with bare metal balloon-expandable coronary stents in a cohort of 50 CLI patients, who were all diagnosed with infragenicular occlusive disease, showed a duplex ultrasonography–derived primary patency at 12 months for the treated vessel of only 62.8%. 25 Similarly, other studies using bare metal stents supported our findings. Scheinert and colleagues found a 6-month binary restenosis rate of 39.1% using a bare metal balloon-expandable stent, 26 whereas Siablis and colleagues reported 12-month binary in-stent restenosis on angiography of 78.6% after having used a range of commercially available uncoated coronary bare metal stents. 27 Because of these poor results, self-expanding nitinol stents for infrapopliteal use were developed, to deal with crush-resistancy and flexibility issues. In the SFA, the patency rate of stainless steel stents has been shown to be below the restenosis rates of self-expanding nitinol stents. 28 Owing to its reduced strut profile, the Xpert stent design may improve patency by reducing wall coverage up to 20%, independently of stent diameter. Stent design (ie, strut thickness, number of struts per cross section, and strut design) has been shown in histologic restenosis studies to have an important impact on the amount of intimal hyperplasia. 22 A thin strut thickness with a corrugated-ring stent design was found to induce the smallest intimal hyperplasia thickness between tested metal stents. 29
A favorable outcome has been reported in four recent independent studies after implantation of balloon-expandable sirolimus-eluting stents (SESs), with high midterm primary patency and limb salvage rates. 26,30–32 Despite these encouraging primary results, all commercially available SESs at the moment are balloon expandable, and the fracture-prone nature of balloon-expandable stainless steel stents could potentially lead to less encouraging long-term outcomes of SES. 24 Further support for the use of SESs in patients with CLI and BTK lesions will be gained from randomized controlled studies, whereas combining nitinol stent technology with active drug coatings could lead to even better clinical and angiographic outcomes, opening new prospects for future CLI strategies.
Study Limitations
This was a nonrandomized, prospective trial conducted in two centers; thus, the published results have to be interpreted with care. Moreover, the patency of the device was determined by duplex ultrasonography rather than conventional angiography. Another limitation of this study is that, owing to the unavailability of the smallest-diameter stents at the start of the trial, there was a tendency toward oversizing the vessels, potentially negatively influencing flow dynamics. Moreover, analysis of patency and limb salvage on the basis of inflow treated lesions was not performed. Perhaps a large-scale randomized trial comparing nitinol stenting BTK versus either PTA or balloon-expandable stent implantation and using angiographic control instead of duplex ultrasonography would be recommended to validate these findings.
Conclusion
The use of a dedicated nitinol stent (Xpert) for BTK lesions, in the treatment of CLI patients, leads to remarkable midterm clinical and patency outcomes. Kaplan-Meier estimation resulted in very encouraging results in terms of 2-year primary and secondary patency, whereas the salvage rate was comparable to or even better than the published reports of surgical revascularization. These findings might challenge the current perspective of BTK endovascular treatment strategy in favor of primary stent use.
Footnotes
Acknowledgments
We take great pleasure in thanking the staff of the Flanders Medical Research Program, with special regards to Koen De Meester and Erwin Vinck for performing the systematic review of the literature and providing substantial support to the data analysis and writing of the manuscript.
Financial disclosure of authors and reviewers: None reported.