
Abstract
The purpose of this article is to report the feasibility and preliminary results of the treatment of isolated iliac artery aneurysms (IAAs) with Anaconda limbs (Vascutek Ltd., Inchinnan, Renfrewshire, Scotland). A prospective cohort is reported of consecutive IAAs treated by two senior surgeons from May to December 2006. One or more Anaconda limbs were used, and internal iliac arteries were embolized if necessary. Twelve IAAs in 11 patients were treated. The average IAA diameter was 4.3 ± 1.1 cm, and the average diameter of stent used was 14 ± 2.5 mm, with an average total length of 97 ± 25 mm. At a mean follow-up of 12 ± 4 months, there were no graft-related complications, graft occlusions, or requirements for reintervention. Endovascular treatment for isolated IAAs under local anesthesia using Anaconda limbs is feasible, safe, and effective. However, as with all new technology, longer follow-up data are necessary.
Isolated iliac artery aneurysms (IAAs) are rare and comprise less than 7% (95% confidence interval 3–14) of all intra-abdominal aneurysms, with a prevalence of 0.3% from autopsy studies. 1,2 IAAs affect males more than females, at a 7:1 ratio, and increase in frequency with age, with the highest incidence being in the seventh and eighth decades. 3 The most common etiology of IAAs is atherosclerosis. Other causes include mycosis, infection, pregnancy, collagen vascular disorders such as Marfan syndrome, surgical trauma, and even excessive athletic effort (bicycle racing). 3
The natural history of IAAs is not well known owing to their relative infrequency. Approximately half of patients are symptomatic at presentation because of rupture, distal embolization, thrombosis, or compression of surrounding organs. 4 The risk of rupture at 5 years is reported to be from 14 to 70%, with an associated mortality of 60%. 3 Further, the diagnosis is often made difficult owing to the absence of a palpable mass. 1,3 Elective repair has been recommended for IAAs greater than 3 cm in maximal diameter. 1–5
Small prospective studies comparing endovascular versus open elective repair for isolated IAAs suggest that endovascular repair may be the preferred first-line approach. 6,7 However, no endograft device currently exists that is specifically designed to treat IAAs. Instead, covered stents or limbs of endovascular grafts for the treatment of abdominal aortic aneurysms have been used. The main issues with these devices have been short lengths requiring multiple stents and a subsequent decrease in lumen diameter and differential longitudinal compliance, graft failure from angulation and repeated movement owing to iliac tortuosity, and dislodgment of the stents at the landing and overlapping zones. 8–12 In some instances, IAAs have been treated with aortobi-iliac (ABI) or aortouni-iliac (AUI) stent grafting to secure the stability of the stents and achieve sealing at the landing zones. However, this subjects an anatomically “normal” proximal aorta to the risk of stent graft deployment. Overall complication rates of endovascular approaches to IAAs range from 10 to 23%. 3 These complications include endoleaks, lower extremity ischemia owing to thrombosis of the stent or distal arterial embolization, pelvic ischemia from disruption of hypogastric flow, and access-site complications, which include infection, hematoma, and pseudoaneurysm. 3
The purpose of this study is to report the feasibility and preliminary results of the treatment of isolated IAAs with a new endovascular stent, called the Anaconda limb (Vascutek Ltd., Inchinnan, Renfrewshire, Scotland). This endograft is made of thin polyester and is externally supported by separate nitinol rings.
Methods
After institutional ethic approval, a prospective cohort was enrolled of consecutive IAAs treated by two senior vascular surgeons at tertiary academic vascular referral centers from May to December 2006.
All patients underwent volumetric contrast-enhanced computed tomography (CT) with a 64-slice scanner. Image postprocessing was done using the Aquarius (TeraRecon Inc., San Mateo, CA) workstation (version 3.5). The length of the segment of artery to be covered and the diameter of the artery at the level of the anticipated landing zones were measured using center-line reconstructions.
Inclusion
IAAs were included if the diameter was > 30 mm, there was at least 5 mm length of proximal neck, there was a distal landing zone of at least 30 mm, and there was absent or treatable stenotic inflow disease. Access vessel diameter had to be a minimum of 6 mm to allow passage of the 18F delivery system. We excluded patients with acute ischemia or rupture at presentation.
Surgical Technique
For the endovascular repair of all IAAs, we used one or more Anaconda limbs in straight or reversed flare configurations (Figure 1).
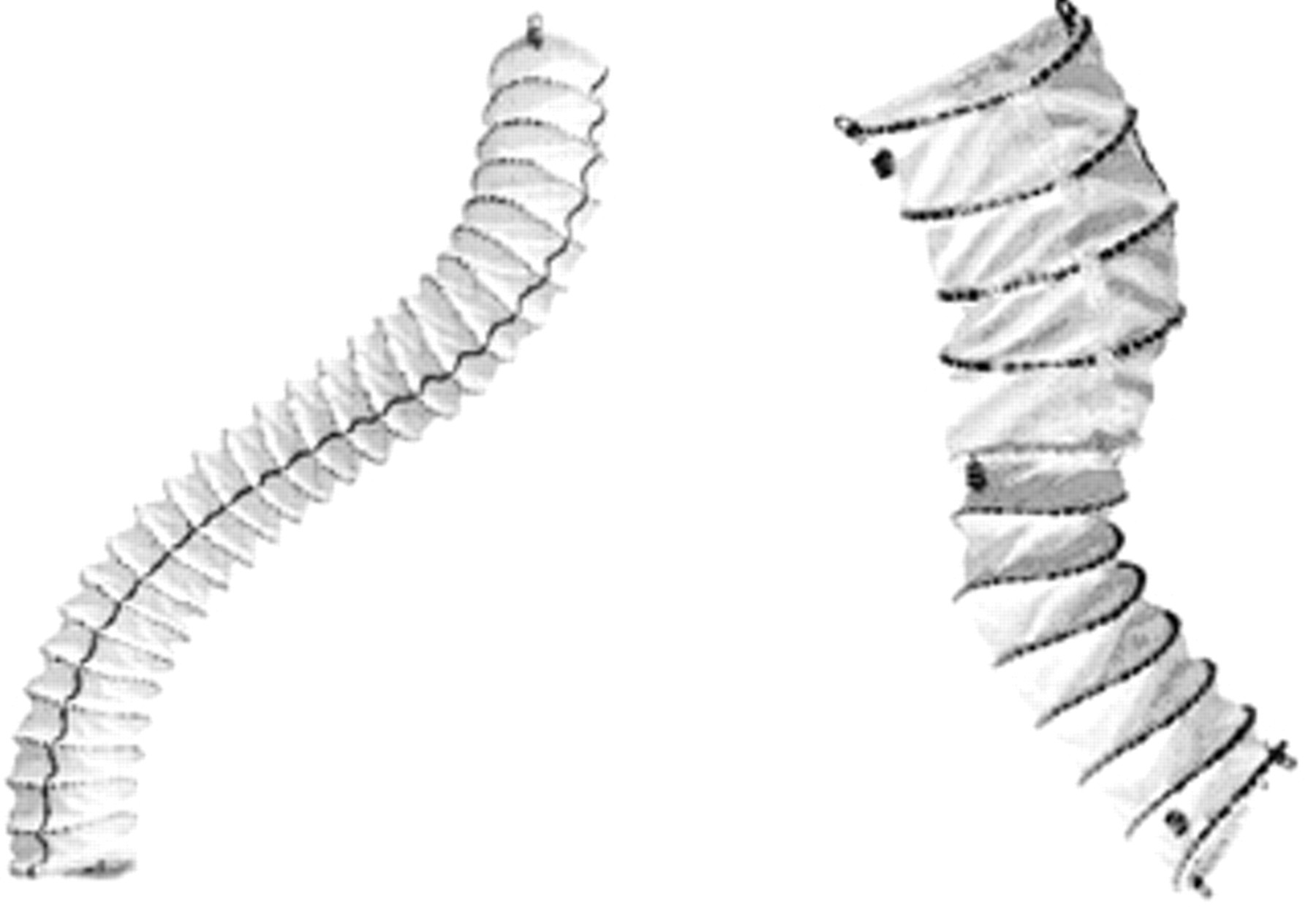
Anaconda limbs in straight and reversed flare configurations.
All procedures were performed in the operating theater using a C-arm. With the patient in the supine position and under local anesthesia, both legs and abdomen were prepared and draped. We surgically exposed the common femoral artery (CFA) through a 4 to 5 cm horizontal incision 3 cm above the inguinal crease and then placed a double polypropylene purse-string suture in the adventitia of the CFA. 13 Six thousand units of heparin was administered before endovascular manipulations.
The internal iliac artery, if necessary, was embolized in a standard fashion through an ipsilateral or a contralateral approach using Tornado and/or Nestor coils (Cook Medical, Bloomington, IN). If a contralateral approach to embolization was used, angiograms were obtained through a straight graduated catheter placed in the contralateral CFA. If an ipsilateral approach was used, a double puncture in the ipsilateral CFA allowed access for angiography.
The delivery system of the Anaconda limb was advanced in the iliac system over a platinum soft-tipped wire (Sorin Group, Milano, Italy). Once the Anaconda limb was unsheathed, a confirmatory angiogram was obtained either through the delivery system of the stent graft or through the 9F sheath repositioned in the common iliac artery. If necessary, a second stent was inserted. Patients with proximal neck lengths from 5 to 10 mm had concurrent placement of a contralateral “kissing” Anaconda limb as well as extension of the proximal portion of both stents up into the distal aorta to create a “double-barrel” seal. Completion angiograms included inflow and outflow to rule out distal embolization and/or dissections. Once all hardware was removed, closure of the artery was achieved by tightening the double purse-string suture, and the wound was closed in a standard fashion.
Postoperative Care
Follow-up included CT angiography at 2 weeks and every 6 months postprocedure with three-dimensional rendering and fly-through analysis.
Results
Twelve IAAs in 11 patients were treated electively during the consecutive 8 months from May 2006: 10 patients had atherosclerotic common iliac aneurysms, and 1 patient had two common iliac pseudoaneurysms after a remote aortobilateral iliac bypass for aneurysmal disease. The median age of the patients was 72 ± 7 years (range 62–82 years). All were men, and all were American Society of Anesthesiologists class 3. 14 Six patients required internal iliac embolizations. The average IAA diameter was 4.3 ± 1.1 cm (range 3.0–6.3 cm). Six aneurysms were treated with two stents, whereas the remaining six aneurysms were treated with a single stent. The average diameter of stent used was 14 ± 2.5 mm, whereas the average total length of stent(s) used was 97 ± 25 mm.
The average hospital stay was 2.6 ± 1.2 days (range 1–6 days), and there were no graft-related complications or graft occlusions at discharge from hospital. At a mean follow-up of 12 ± 4 months, there were no graft-related complications, graft occlusions, further sac enlargement, or requirements for reintervention. One patient with concurrent aneurysmal dilation of the proximal portion of the ipsilateral internal iliac artery demonstrated a type II endoleak despite the placement of distal (anterior and posterior division) coils and continues to be followed.
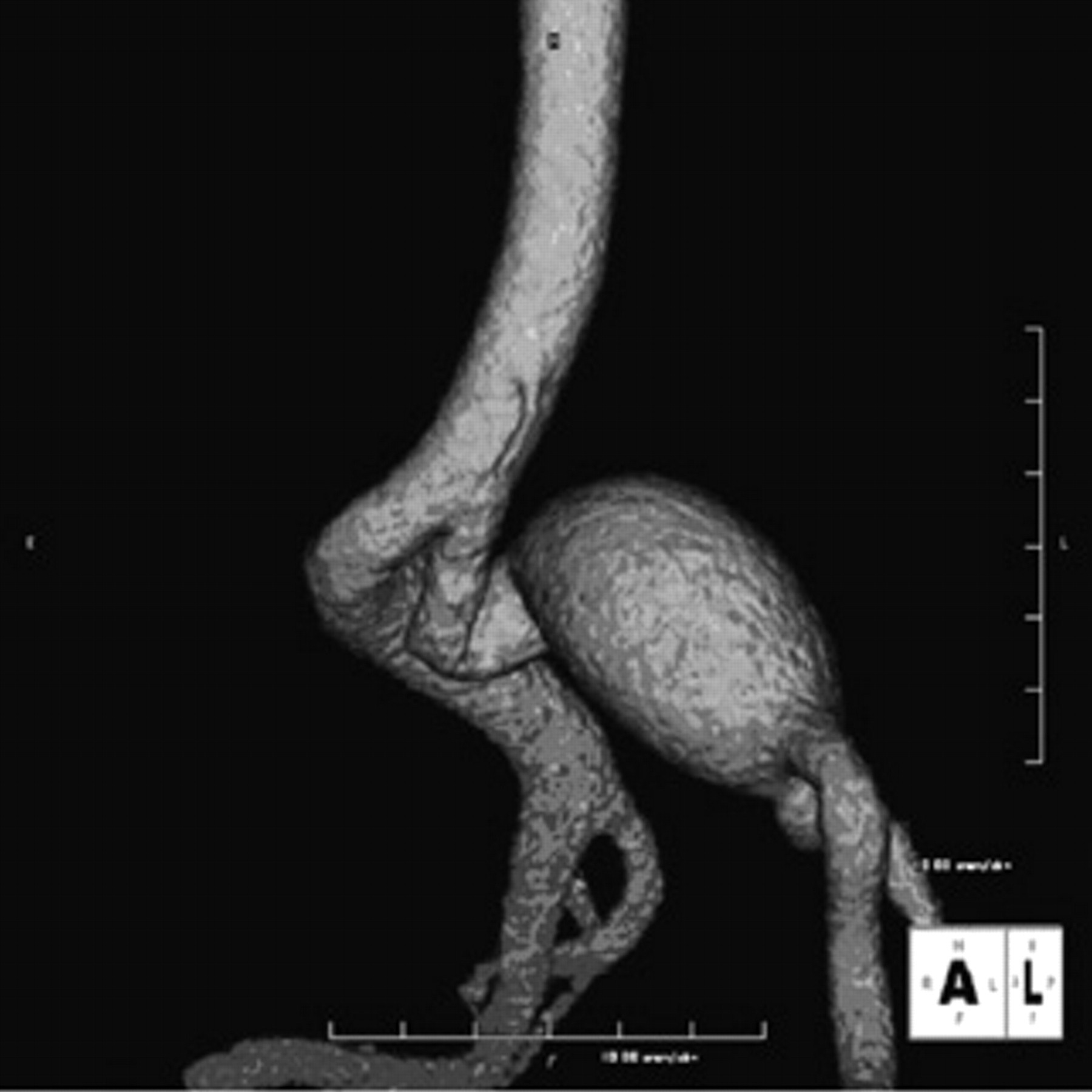
Figure 2 and Figure 3 show an isolated IAA treated with embolization of the internal iliac artery and stenting with a reversed flare Anaconda limb. Figure 4 and Figure 5 display, respectively, the luminal appearance of the Anaconda limb and of the external iliac artery just distal to it. The native artery has a ribbed appearance, similar to that of the Anaconda limb. Severe angulation of the proximal neck of one IAA is demonstrated in Figure 6. After embolization of the ipsilateral IAA, the aneurysm was excluded with a straight Anaconda limb, as shown in Figure 7.

Right common iliac artery aneurysm.

The right common iliac artery aneurysm has been treated with embolization of the internal iliac artery and stenting using an Anaconda limb.

Fly-through view of the Anaconda limb in an iliac artery aneurysm.

Fly-through view of the external iliac artery just distal to the landing zone of an Anaconda limb.
Isolated iliac artery aneurysm with an angulated proximal neck.

Isolated iliac artery aneurysm with an angulated proximal neck after embolization of the internal iliac artery and repair of the aneurysm with an Anaconda limb.
Discussion
Open surgical repair of isolated IAAs in good surgical risk candidates has traditionally been the standard of care. 1–5 Open repair involves the interposition of prosthetic grafts through a retroperitoneal or transperitoneal approach. However, outcomes for open elective repair of isolated IAAs have not been extensively studied. 1–5 The main risks that have been reported with the open repair include lower extremity ischemia from distal embolization or stenosis, visceral and pelvic wall ischemia from disruption of hypogastric flow, aneurysm reperfusion and rupture, arterioenteric fistula, graft infection, and adjacent ureteral and iliac vein injury. 3 The technical challenges of these deep pelvic procedures and the often associated pelvic ischemic syndromes have resulted in reported complication and overall mortality rates ranging from 11 to 33%. 3,15
The use of covered stents to deal with IAAs has been shown to be feasible in several studies. 8–12 A systematic review of the English literature in 2005 identified six retrospective studies reporting on 117 IAAs treated by an endovascular approach. Perioperative mortality was 1% (range 0–4%), but no long-term data were available. 3 The overall incidence of perioperative complications was 20% (range 10–23%), with the most common complication being an anastomotic endoleak occurring in 4% of patients (range 0–7%). 3 Two more recent retrospective studies have reported on 132 additional IAAs treated with endovascular repair. 8,15 Boules and colleagues treated 34 patients (75%) with unilateral iliac stent grafts, 8 (18%) with bifurcated aortic stent grafts, and 3 (7%) with coil embolization alone and reported a mean postoperative length of stay of 1.3 ± 1.0 days. 8 Perioperative major complications in this series included one early graft thrombosis and one groin hematoma. Late complications included one additional graft thrombosis and one late death after amputation. Five endoleaks were noted (four type II, one indeterminate) at 1 month, with four other endoleaks (one type II, one type III, two indeterminate) identified on later CT scans. At 2 years, primary patency was 95% (Kaplan-Meier analysis), and freedom from secondary interventions was 88% (Kaplan-Meier analysis). Chaer and colleagues retrospectively reviewed their experience of 52 patients with IAAs treated with endovascular repair, including 39 patients (75%) with either a stent graft limb or covered stent, 13 patients (25%) with a bifurcated aortic device, and 1 patient (2%) with coil embolization alone. 15 They compared their results with those of a concurrent series of 19 patients with an open repair. The length of stay was 1.3 ± 1.0 days, which was significantly less than that observed for open repair (5.2 ± 2.3 days). Complication rates were similar between the open and endovascular groups, although pelvic ischemia, including the one fatality related to bowel infarction, was uniquely observed in the endovascular group. Limb thrombosis (4%) and endoleaks (6%) required secondary interventions in the endovascular group, with a freedom from secondary intervention rate of 91% and 81% at 1 and 2 years, respectively. No postoperative ruptures, aneurysm-related deaths, or aneurysm expansion was observed. None of the reported series have consistently reported on the type of stent graft or limb used during endovascular repair of IAAs.
The treatment of isolated IAAs with aortic stent grafts is not uncommon. 8,15 However, the use of ABI or AUI endografts may subject an anatomically “normal” proximal aorta to the risks of stent graft deployment, including perirenal complications, renal embolization, or occlusion. AUI devices require the placement of an extra-anatomic femorofemoral bypass graft, which has the inevitable increased risks of groin wound infection and graft infection complications. With ABI devices, the contralateral limb is often constrained by the narrow distal aorta observed in most of these patients and fails to fully open, potentially increasing the risks of failed intraoperative stump cannulation and postoperative limb thrombosis. The Anaconda limb technique, which also has a direct cost advantage over aortic stent grafts, allows for the exclusion of a limited diseased segment and avoids the aforementioned risks. Additionally, the use of the iliac limb does not preclude the later use of an AUI or ABI graft if further aneurysmal dilation, attachment-site endoleak, or stent migration occurs.
The unique concentric nitinol ring design of the Anaconda limb affords great flexibility and seems to provide ideal characteristics for the treatment of isolated IAAs. The stent adapts very well to tortuous and angulated iliac anatomy and allows in vivo length adjustment during deployment. In addition, the proximal one or two rings of the Anaconda limb (either reversed flare or straight configuration) can be placed just proximal to the origin of the iliac artery during deployment, resulting in full expansion of these rings, which “rivet” the device into position and prevent its downward displacement during the cardiac cycle. If the neck of the IAA is short (5–10 mm in length), consideration may be given to our technique of using a “kissing” Anaconda limb, inserted from the contralateral side. This has the effect of buttressing the iliac aneurysm limb and results in an excellent seal provided that the aorta is of normal caliber.
Our work shows the feasibility of using Anaconda limbs to treat isolated IAAs, with excellent perioperative results that are comparable to those reported in the literature. Furthermore, the Anaconda limb was not associated with limb thrombosis in our series, something that has been observed by other investigators using more rigid devices that are not as well suited to the rigors of iliac deployment. Endovascular repair can be performed under local anesthesia; consequently, the time to ambulation and length of stay in hospital are short, with minimal complications. Our medium-term results show the durability of these endostents, which were not associated with any occlusions, reinterventions, or other aneurysm-related complications.
Although the strength of this study lies in its systematic and consistent approach to the management of consecutive patients and in the use of a device that is better suited to iliac deployment, the inferences that may be drawn are limited by the fact that isolated IAAs are rare; therefore, our sample size was small. This may explain the absence of complications in our medium-term follow-up period. A longer follow-up period with more patients will be necessary to establish the durability of this type of repair.
Conclusion
Endovascular treatment for isolated IAAs under local anesthesia using Anaconda limbs is feasible, safe, and effective. The Anaconda device has unique features that may prove ideal for use in the treatment of iliac aneurysmal disease. However, as with all new technology, longer follow-up data are necessary to establish the durability of this type of repair.
Footnotes
Acknowledgment
Financial disclosures of authors and reviewers: None reported.
Presented at the Association of International Vascular Surgeons 26th Annual Meeting, Club Med, Chamonix, France, March 9–16, 2008.