
Abstract
The purpose of this study was to investigate the results of a staged treatment of symptomatic focal nodular hyperplasia (FNH), consisting of first embolization and then resection. A 36-year-old woman presented with pulmonary embolism caused by an inferior caval vein thrombosis owing to external compression by FNH in liver segment I (5.2 × 6.7 cm). She was treated with anticoagulants. The FNH lesion was first reduced by radiologic embolization of the feeding branch of the right hepatic artery. A 41% size reduction was obtained, and the symptoms disappeared. FNH resection was performed 5½ months later. The thrombus had disappeared, and the anticoagulant therapy could be stopped perioperatively. A symptomatic FNH lesion was treated successfully in two stages.
We describe a patient who presented with inferior caval vein thrombosis owing to external compression by focal nodular hyperplasia (FNH) in liver segment I.
The incidence of deep venous thrombosis is 56 to 160/100,000/year. 1 According to Virchow's postulates, three factors are of primary importance for the development of venous thrombosis: abnormalities of blood flow, abnormalities of blood, and vessel wall injury. The risk factors for thrombosis are shown in Table 1. 1
Risk Factors for Thrombosis
For the diagnosis of deep venous thrombosis and pulmonary embolism, D-dimers have a sensitivity of 92%. Ultrasonography and venography can be used for the diagnosis of deep venous thrombosis with a sensitivity of 87% and 91%, respectively. Ventilatory perfusion scanning, fluoroscopy, and spiral computed tomographic (CT) angiography can be used for the diagnosis of pulmonary embolism with a sensitivity of 63%, 81%, and 87%, respectively. 2
Deep venous thrombosis is normally treated with anticoagulant therapy. Heparin and, increasingly, low-molecular-weight heparin work immediately. The patient can start with coumarins in countries where a necessary thrombosis service is present. The duration is 3 months in the case of transient risk factors and longer in other cases. 3 In case of a contraindication for anticoagulant therapy, an inferior caval vein filter can be placed. 4 Inferior caval vein filters may be only modestly efficacious in reducing the recurrence of pulmonary emboli and do not affect mortality. 3 Thrombectomy may be efficacious in well-chosen patients, principally active patients with an acute iliofemoral thrombosis. 5 The first line of treatment is often catheter-directed thrombolysis or percutaneous mechanical thrombectomy with catheter-directed thrombolysis. 1 Patients who have a contraindication to thrombolysis can be treated with a surgical thrombectomy. 5 Randomized controlled trials are necessary to investigate whether the outcomes are superior, especially with respect to the postthrombotic syndrome consisting of edema, pain, and dermatitis and in a late-stage ulceration. 1,5
FNH is characterized by hyperplastic liver parenchyma divided in noduli by septa, 6 with a prevalence of 0.4 to 0.8%. 7 Usually, the lesion is solitary (80%), smaller than 5 cm, without a capsule, and asymptomatic. In less than one-third of patients, abdominal pain is present, and spontaneous bleeding is rare.
Laboratory investigation shows increased α-fetoprotein, and sometimes liver enzymes, especially γ-glutamyltransferase (GGT), are increased. Radiographic imaging can best be performed with CT, magnetic resonance imaging (MRI), or angiography. 6,8 With classic ultrasonography, FNH is not very easily distinguished. FNH is clearly visible in the arterial phase of a CT scan with intravenous contrast as a hypervascular lesion with a typical hypodense central scar. Using MRI, FNH is present as a hypo- or isodense lesion on T1-weighted images and iso- or hyperdense on T2-weighted images. After the administration of gadolinium, the same image is observed as with CT. Angiography shows a hypervascular lesion with a coiling feeding artery. In the event that radiographic imaging is not conclusive, a biopsy can be performed, where histology shows a central scar with coiling arteries.
Treatment of FNH is performed only when symptomatic or in uncertain cases, such as when a malignancy cannot be excluded. 7 FNH can be treated by surgery (open or laparoscopic), embolization, or a combination of both. 9 Open surgery of benign liver tumors has a mortality rate below 5% 7,10 and a morbidity rate of 11 to 25% in specialized centers. 10,11
Case Report
A 36-year-old woman without a medical history presented with complaints of fatigue and dyspnea on exertion. She used oral contraceptives, and her family history was positive for venous thrombosis with respect to her mother and grandmother. However, research as to the cause of this thrombosis had never been performed.
The general practitioner performed a blood test showing elevated GGT, and ultrasonography showed a liver process. The patient was then referred to the hospital for further analysis.
The patient's physical examination was normal. A radiograph of the thorax had no abnormalities. CT demonstrated that the process in the liver was FNH as a typical focal homogeneous contrast-enhanced lesion with a central hypodense area was present. The lesion was 5.2 × 6.7 cm in diameter and located in segment I of the liver, causing compression of the inferior caval vein (Figure 1). As a side result, a thrombus was present in the inferior caval vein and the right common iliac vein. The hepatic inflow into the inferior caval vein was not disturbed. Extensive pulmonary embolism was present. Another ultrasound investigation and venography confirmed the diagnosis of a thrombus of 12 cm present in the inferior caval vein and the right common iliac vein.

Computed tomographic scan at the time of diagnosis. Extended pulmonary emboli are present. A, Focal nodular hyperplasia (FNH) in segment I of the liver typically with focal homogeneous contrast enhancement and a central hypodense area, size 5.2 × 6.7 cm. B, Compression on the inferior caval vein by the FNH lesion resulted in thrombus formation (arrow) in the inferior caval vein and in the right common iliac vein. Collateral blood flow exists, mainly via the gonadal veins.
With angiography, vascularization of the tumor was established, which showed that the process was fed by a branch of the right hepatic artery (Figure 2).
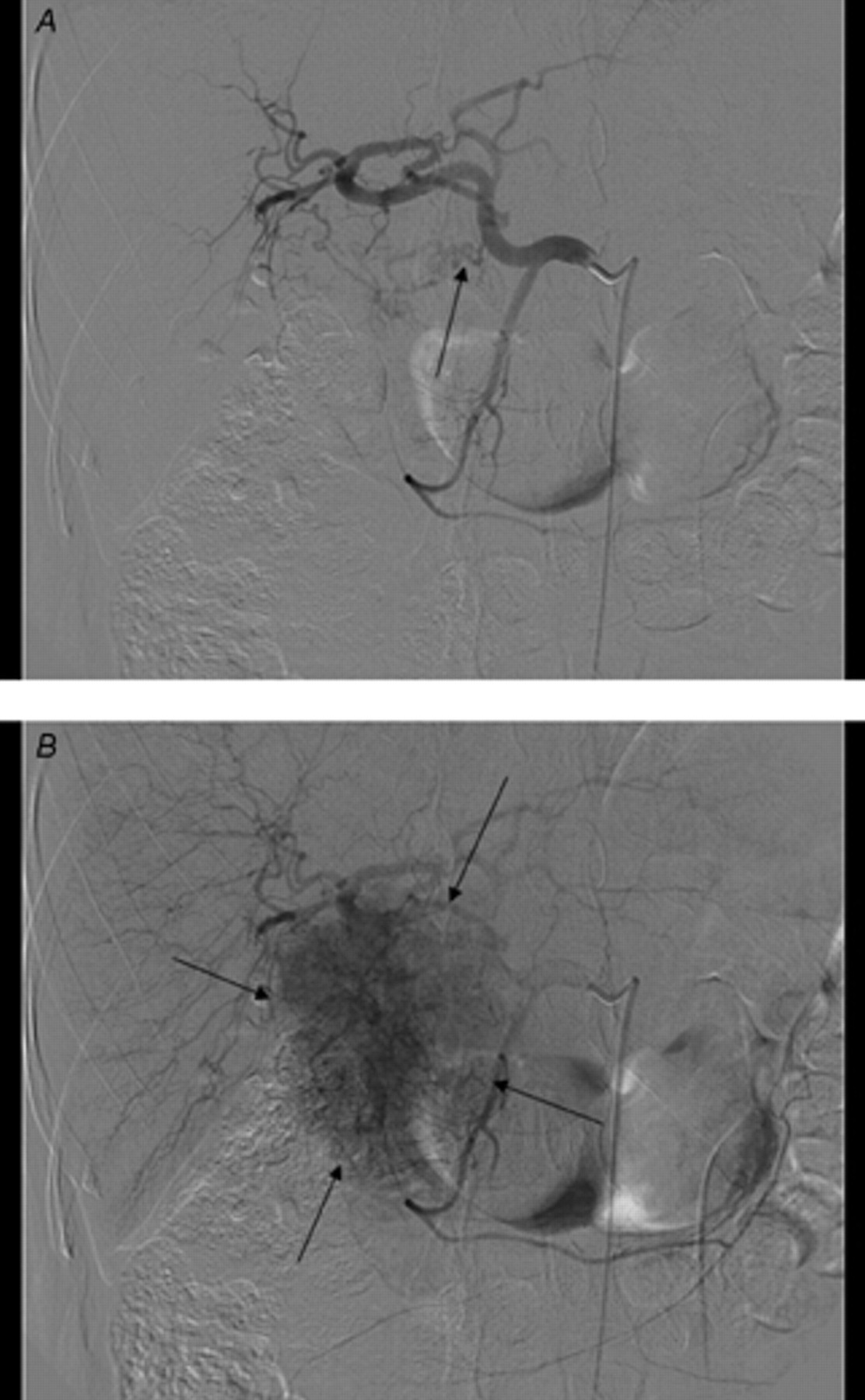
A, Angiography with catheterization of the common hepatic artery. The focal nodular hyperplasia tumor is fed by a twisting branch (arrow shows the starting point of the feeder) of the right hepatic artery. No liver branch from the superior mesenteric artery is present. B, The lesion stains prominently (arrows point to the lesion stains).
Laboratory investigation for congenital or obtained causes of thrombophilia did not show any abnormalities. D-dimers were increased (3.05 instead of 0.5), protein C activity was 124% (range 70–140%), protein S activity was 101% (range 58–108%), plasminogen activity was 143% (range 74–124%), activated protein C (APC) was 0.99, and lupus anticoagulant was negative. A factor V Leiden mutation could be excluded because APC was normal (≥ 0.9). The patient was treated with immobilization, heparin, and coumarins. Four days after admission to our hospital, she complained of a painful right calf. Physical examination was still without any abnormalities. As soon as the international normalized ratio was between 2 and 2.5, heparin was discontinued. One month after the symptoms began, selective embolization of the feeding branch of the right hepatic artery was performed with polyvinylalcohol particles (Contour 250–350 micron, Boston Scientific, Natick, MA). Some smaller suppliers could not be catheterized and so could not be embolized. After the procedure, good devascularization of the tumor was obtained, and the patient was discharged within 2 days.
A four-phase CT scan 3½ months later showed that the FNH had decreased to 4.1 × 5 cm, and the thrombus in the inferior caval vein and the right common iliac vein had disappeared (Figure 3).

A, A four-phase computed tomographic scan 3½ months after right hepatic artery embolization shows the reduced perfusion and size (4.1 × 5 cm) of the focal nodular hyerplasia (arrow). B, The thrombus in the inferior caval vein has dissolved (arrow).
Five and a half months after the beginning of the symptoms, the patient underwent surgery. Anticoagulant therapy could be stopped perioperatively. The tumor was present at the level of the inferior caval vein in segments I and VII, and the duodenum was adherent to the process (Figure 4). The right part of the liver was mobilized and the duodenum was released, and cholecystectomy was performed. The FNH lesion was lifted from the cava, and direct branches were clipped. With the help of a Cavitron ultrasonic surgical aspirator (Valleylab Inc, Boulder, CO), the area adherent to segment I and subsequently to segment VII was dissected and the vessels were clipped. After removal of the specimen, the wound surface of the left hemiliver was coagulated with argon beam coagulation and covered with TachoSil (Nycomed, Melville, NY). A drain was left in situ, and the patient remained in the intensive care unit for 1 day. Coumarins were reinitiated postoperatively. The gastric tube, bladder catheter, epidural anesthetic catheter, and drain were removed on the third day. The course was uneventful, and the patient was discharged from the hospital by the sixth day.
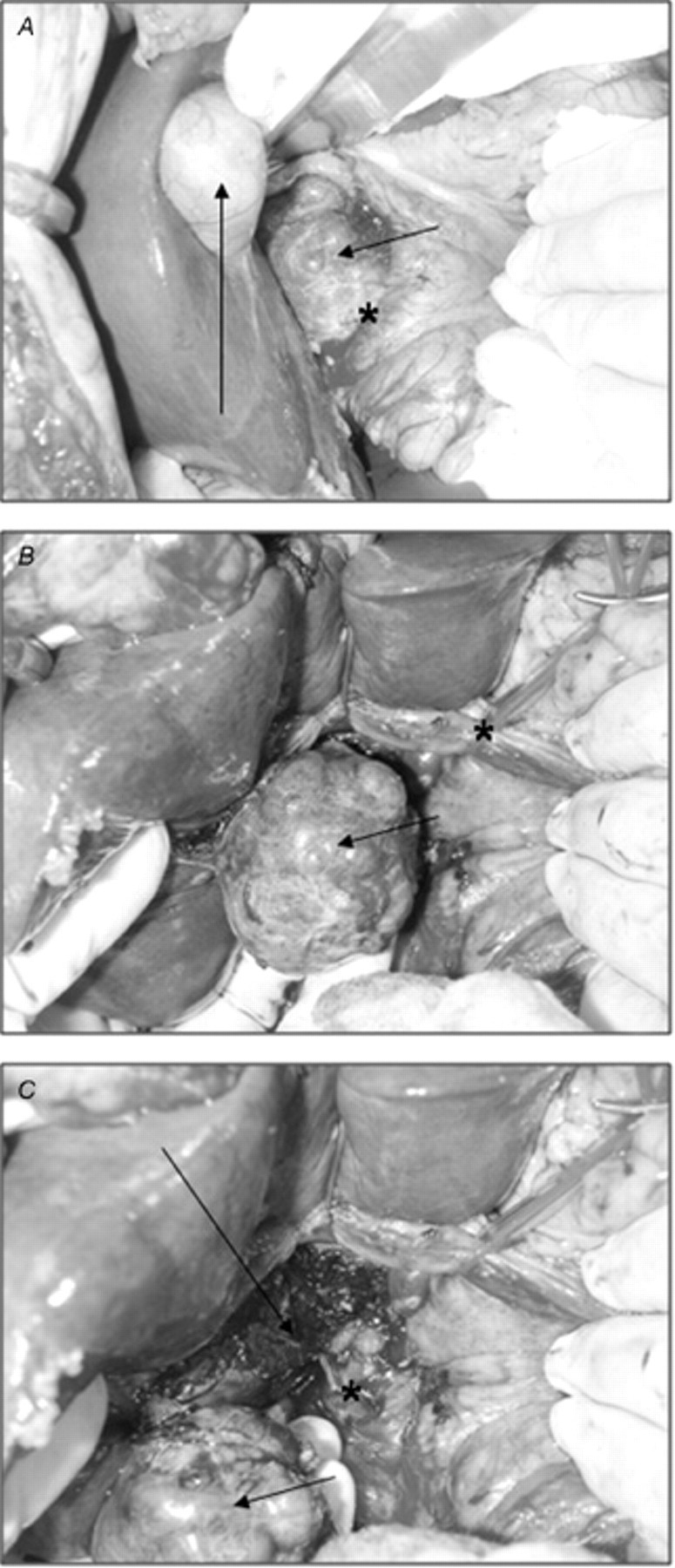
Surgical images. A, Long arrow: gallbladder; short arrow: the focal nodular hyperplasia (FNH) lesion in segment I of the liver. The lesion is adherent to the duodenum (asterisk). B, Short arrow: the tumor. Adhesions of the FNH to the duodenum have been dissected. With the aid of the Cavitron ultrasound surgical aspirator, the lesion is dissected from segments I and VII. The hepatoduodenal ligament is encircled with a vessel loop (asterisk). C, Short arrow: the released tumor; long arrow: the liver dissected area, mainly from segment I. Direct branches to the inferior caval vein have been clipped (asterisk).
Pathologic investigation showed a gallbladder with extensive cholesterolosis. The specimen of segment I was almost completely occupied by FNH in which ischemic areas with necrosis were present, caused by vascular occlusions owing to embolization. No signs of malignancy were present.
Coumarins were continued for 3 months after the operation. Five months after the operation, the patient had recovered uneventfully.
Discussion
We describe a rare case of FNH resulting in inferior caval vein thrombosis in a patient with a positive family history of venous thrombosis. The strategy was to first decrease the size of the tumor, using selective arterial embolization, and then at a later stage to perform a resection. The reason for this staged approach was the absolute necessity for anticoagulant therapy and the large size of the FNH lesion. The lesion was decreased by 41%, and the thrombus disappeared, after which, an uncomplicated segment I resection could be performed. Given that the thrombus had disappeared, anticoagulant therapy could be ceased perioperatively.
In our patient, the thrombus had existed too long to perform catheter-directed thrombolysis. As an alternative, percutaneous mechanical thrombectomy could have been performed with an inferior caval vein filter to prevent further pulmonary embolism. Given that we were not fully informed about the composition of the thrombus, with a small chance of being malignant, we did not want to displace the thrombus. A surgical thrombectomy is a procedure with high morbidity. The implantation of an inferior caval vein filter, perioperatively, was not necessary because the thrombus had fully dissolved.
The embolization procedure was performed 1 month after the symptoms began; this could have been done earlier in the course of the disease. The complex case was, however, extensively discussed before a definitive plan was made. The embolization procedure was continued by a surgical resection to prevent new complications as serious complications had occurred from the FNH at this location. The interval between the embolization and the resection was guided by the shrinkage of the FNH and the disappearance of the thrombus at follow-up CT. This interval should be judged for each case individually.
Since the 1980s, only a few case reports have been published concerning the embolization of FNH lesions in symptomatic patients to reduce the tumor. 12–17 Embolization is less invasive than surgery and carries a lower morbidity and mortality. 13 The disadvantage of embolization is that the reduction of the lesion takes months. 14,16,17 A coiling procedure can be complicated by a postembolization syndrome, characterized by high fever, an increased C-reactive protein level, and the presence of air pockets in the vicinity of the tumor (on CT scan). 9,13,17 Accidental tissue necrosis owing to dislocation of the particles or permeation of liquid embolic material in the capillary bed has been described. 13
The bleeding risk, owing to the marked vascularization 9,12 and the size of the tumor, can make surgery difficult. The bleeding risk and the size of the tumor can be decreased by first coiling the feeding artery. 9,12–14,16,17 The combination of embolization and surgery, as described here, has only been published once before. 9 Wilhelm and colleagues performed an embolization before laparoscopic FNH resection in two patients to minimize blood loss. 9 The operation was performed immediately after the embolization, so reduction of the tumor was not studied. As far as we know, our report is the first on a staged approach, in which the definitive resection was performed after embolization to reduce the bleeding risk and, most importantly, to decrease the size of the tumor.
Conclusion
Inferior caval vein thrombosis can be caused by compression from the outside; in this patient, an FNH lesion was responsible. FNH is asymptomatic most of the time, but when symptomatic, there is an indication for treatment. A staged procedure, consisting of coiling the feeding artery to decrease the tumor size, followed by resection is a valid option in these cases. An additional advantage may be the disappearance of the thrombus before surgery.
Footnotes
Acknowledgment
Financial disclosure of authors and reviewers: None reported.