
Abstract
The objective of this study was to determine whether ankle peak systolic velocity (APSV) can predict nonhealing in diabetic foot lesions. Diabetic patients referred for duplex scanning of the lower extremity arteries were included if they had foot lesions such as ulcers, gangrene, or tissue necrosis and had no palpable pedal pulses. End points were healed or healing foot lesions, revascularization, major amputation, or death. One hundred consecutive limbs were included. Forty-three limbs with diabetic foot lesions reached the end point of adequate healing or complete healing, whereas 57 limbs had nonhealing lesions. The APSV was significantly higher in limbs with healed or healing lesions compared with limbs with nonhealed lesions: 53.0 cm/s (41.8–81.6) versus 19.2 cm/s (12.4–26.5), p < .0001. At a cutoff point of 35 cm/s, the APSV showed a sensitivity of 92.9% (95% confidence interval [CI] 82–97), a specificity of 90.6% (95% CI 76–96), a positive predictive value of 92.9%, and a negative predictive value of 90.6% in predicting nonhealing of diabetic foot lesions. There was a significant difference between the APSV before and after revascularization: 20.4 cm/s (12.4–26.3) versus 48.8 cm/s (36.1–80.8), p < .0001. APSV could predict nonhealing of diabetic foot lesions with a high degree of accuracy in this group of patients.
The ankle-brachial index (ABI) is widely used for the assessment of the degree of peripheral ischemia. 1,2 However, this parameter is not accurate in the presence of arterial wall calcification as it gives falsely high results. 3 The toe-brachial index (TBI) has been used as an alternative because digital arteries are less affected by calcification. 4,5 However, the incidence of digital artery calcification among diabetics is still significant. 6 In addition, it is impossible to measure toe pressures in a substantial number of patients presenting with diabetic foot lesions because the toes are affected by ulcers or gangrene or have been amputated, which makes the TBI invalid or impossible to use. 7
We have previously described a new alternative parameter for the assessment of degree of peripheral ischemia: ankle peak systolic velocity (APSV). 8 The rationale of APSV is based on the observation that in ischemic limbs, blood moves at much slower velocity in the distal leg arteries compared with blood in nonischemic limbs. This is noted on angiography as well as on duplex ultrasonography studies. The purpose of this new parameter is to measure the degree of foot perfusion through measurement of blood velocity in the main arteries supplying the foot, namely, the distal anterior tibial artery and the distal posterior tibial artery at the ankle level.
APSV is the mean of the peak systolic velocities measured across the distal tibial arteries at the ankle level. We showed that APSV strongly correlates with the ABI and with the TBI whenever those can be reliably measured. We also demonstrated that APSV correlates well with the clinical classification of peripheral ischemia as described by Rutherford. 9 APSV is not affected by vessel calcification and can be measured in the presence of toe gangrene or amputation; therefore, APSV is advantageous in those situations. APSV is measured during arterial duplex scanning of the lower extremities, which is routinely performed in most centers for the assessment of peripheral ischemia. APSV takes no extra time and adds no extra cost to that of the routine arterial duplex scan.
The objective of the current study was to determine whether APSV could be used to predict nonhealing of diabetic foot lesions.
Methods
Institutional review committee approval was obtained. Patients referred for arterial duplex scanning were examined for the presence of foot lesions and the presence of pedal pulses (dorsalis pedis and posterior tibial pulses). Patients were included in the study if they were diabetic, had absent dorsalis pedis and posterior tibial pulses in the affected leg, and had foot lesions in the form of ulcers, gangrene, or tissue necrosis. The study was initiated in September 2005 and was completed in July 2007 with the inclusion of 100 consecutive limbs. If a patient presented with a foot lesion that did not heal and required revascularization, the patient was entered once initially as a nonhealed lesion and entered once again after revascularization. If the inclusion criteria were applicable to both limbs in the same patient, each limb was entered separately.
This was a prospective study. Data were prospectively collected and maintained on computer. Data were collected regarding age, gender, diabetes mellitus, hypertension, ischemic heart disease, renal impairment, cerebrovascular accident, dyslipidemia, foot lesions, dorsalis pedis and posterior tibial pulses, and full details of duplex scanning, including APSV. Nonischemic lesions and lesions in revascularized limbs were treated by daily dressings and followed up monthly. Wound dressing protocol was standardized. Patients presenting with nonhealing lesions or manifestations of critical limb ischemia such as ischemic rest pain, ischemic ulcers, and ischemic gangrene underwent revascularization procedures by endovascular or open surgical technique. Patients were followed up until they reached one of the end points of the study, which were a healed wound, a healing wound, revascularization by open surgery or endovascular technique, major amputation, or death. A wound was considered completely healed if it was fully covered with intact skin. It was considered adequately healing if it was completely covered with healthy granulations, with absence of tissue necrosis or infection. It was considered nonhealed if it did not show signs of healthy granulations after 1 month of follow-up or if the patient developed manifestations of critical limb ischemia. Treating physicians were blinded to the results of APSV.
During follow-up, data were collected regarding wound status, the details of the revascularization procedure, amputation, if any, and details of duplex scanning, including APSV.
Duplex scanning was performed by one experienced operator (W.T.) using a Toshiba Xario (Toshiba Medical Systems Corporation, Otawara-shi, Tochigi-ken, Japan) or an HP Sonos-7500 (Philips Healthcare Nederland B.V., Eindhoven, the Netherlands). The method of calculating APSV was described in our previous study. 8 Briefly, APSV is the mean of the peak systolic velocities of the anterior and posterior tibial arteries measured at the ankle level. Assessment of APSV was performed as part of the arterial duplex scan. A 5 MHz convex probe was used for the aorta and iliac arteries, and a 5 to 12 MHz linear transducer was used for the infrainguinal arteries. The Doppler angle of insonation was adjusted to 60°. All patients were rested 1 hour before scanning and were examined in the supine position. Recordings were made with the room temperature adjusted to 22°C. Peak systolic velocities of the distal posterior tibial artery at or below the malleolar level and the distal anterior tibial artery just above the ankle joint level were recorded. Peak systolic velocities were averaged over three cardiac cycles. The APSV is the mean value of the peak systolic velocities of the distal anterior and posterior arteries. If a focal stenotic lesion was detected in one of the distal tibial arteries, velocity measurements were taken distal to the stenosis. No alterations were made to the patient's medications prior to scanning.
Data were prospectively maintained on computer. Minitab statistical software (version 13.1, Minitab Inc., State College, PA) was used for analysis. Statistical comparisons were performed using the Mann-Whitney U test for comparing two groups and the Wilcoxon test for comparing the changes to a group for non-normally distributed continuous variables. The chi-square test was used for discrete variables. Logistic regression analysis was performed to identify independent predictors of wound nonhealing. Results were expressed as median and interquartile range (Q 1 –Q 3 ). A receiver operating characteristic (ROC) curve was used to determine the cutoff APSV value with the maximum sensitivity and specificity. A p ≤ .05 was considered statistically significant.
Results
The study included 100 limbs, belonging to 62 patients. Their median age was 63 years (range 42–78 years). All patients were diabetic. The demographic characteristics and risk factor distribution are shown in Table 1.
Demographic Characteristics and Distribution of Risk Factors
Forty-three limbs with diabetic foot lesions reached the end point of adequate healing or complete healing: 7 without revascularization and 36 following revascularization (16 had bypass surgery and 20 had endovascular interventions). Fifty-seven limbs with diabetic foot lesions had nonhealing wounds or showed manifestations of critical limb ischemia; 48 of those had revascularization procedures (20 had bypass surgery, 21 had endovascular intervention, and 7 had both), 2 had primary major amputations, 2 had major amputation following failed revascularization, 1 patient died, and 4 were advised to have revascularization but did not comply and were lost to follow-up.
The median APSV of the 43 limbs with healed or adequately healing lesions was significantly higher than that of the 57 limbs with nonhealing lesions: 53.0 cm/s (41.8–81.6) versus 19.2 cm/s (12.4–26.5), p < .0001 (Figure 1). Logistic regression analysis was performed to identify independent predictors of wound nonhealing. All variables-age, gender, diabetes mellitus, hypertension, ischemic heart disease, renal impairment, cerebrovascular accident, dyslipidemia-except the APSV were found to be nonsignificant in predicting healing versus nonhealing. ROC curve was used to determine the cutoff APSV value with the maximum sensitivity and specificity (Figure 2). At a cutoff value of 35 cm/s, it was found that the APSV showed a sensitivity of 92.9% (95% confidence interval [CI] 82–97%), a specificity of 90.6% (95% CI 76–96%), a positive predictive value of 92.9%, and a negative predictive value of 90.6% in predicting nonhealing of diabetic foot lesions. A subgroup of 30 patients had the APSV assessed before and after revascularization. A significant difference was found between the APSV before and after revascularization: 20.4 cm/s (12.4–26.3) versus 48.8 cm/s (36.1–80.8), p < .0001 (Figure 3). Other patients who had revascularization were not included in this analysis because they had one of the two duplex scans, either the one before or the one after revascularization, performed elsewhere; therefore, they did not have APSV available for comparison. There was no significant difference between the APSV of limbs that had open surgery compared with endovascular revascularization: 53.5 cm/s (40.6–81.7) versus 52 cm/s (41.5–75), p = not significant.

Ankle peak systolic velocity (APSV) of healed lesions versus nonhealed lesions. Median and interquartile range (Q1–Q3) were 53.0 cm/s (41.8–81.6) versus 19.2 cm/s (12.4–26.5) for healed and nonhealed lesions, respectively. Mann-Whitney U test p < .0001.
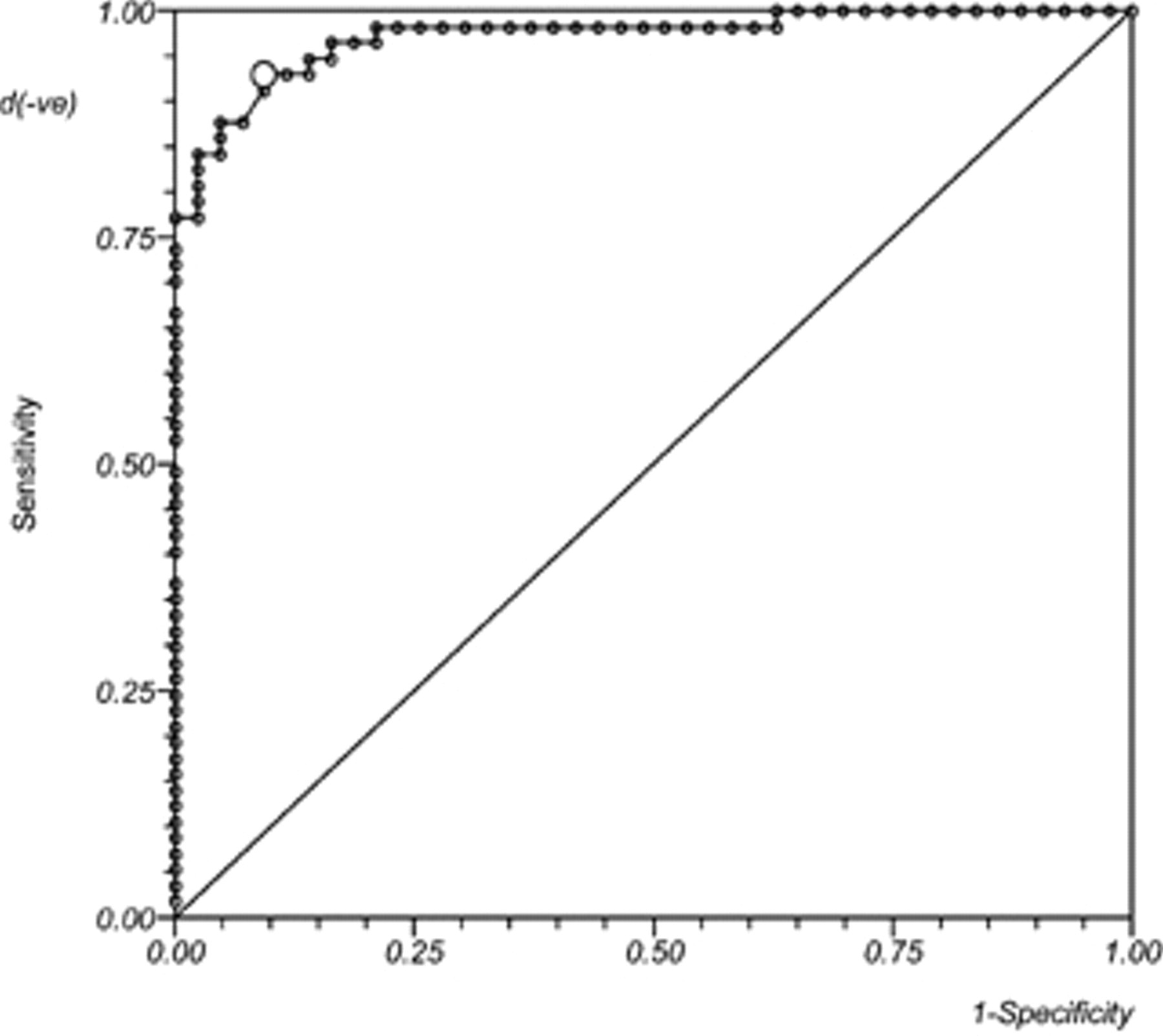
Receiver operating characteristic (ROC) curve analysis. Data set: nonhealed (+ve) and healed (-ve). Area under the ROC curve by extended trapezoid rule = 1.981844. Wilcoxon estimate of area under the ROC curve = 0.972256. DeLong standard error = 0.193308: 95% confidence interval = 0.59338 to 1. Optimum cutoff point selected = 35.1.
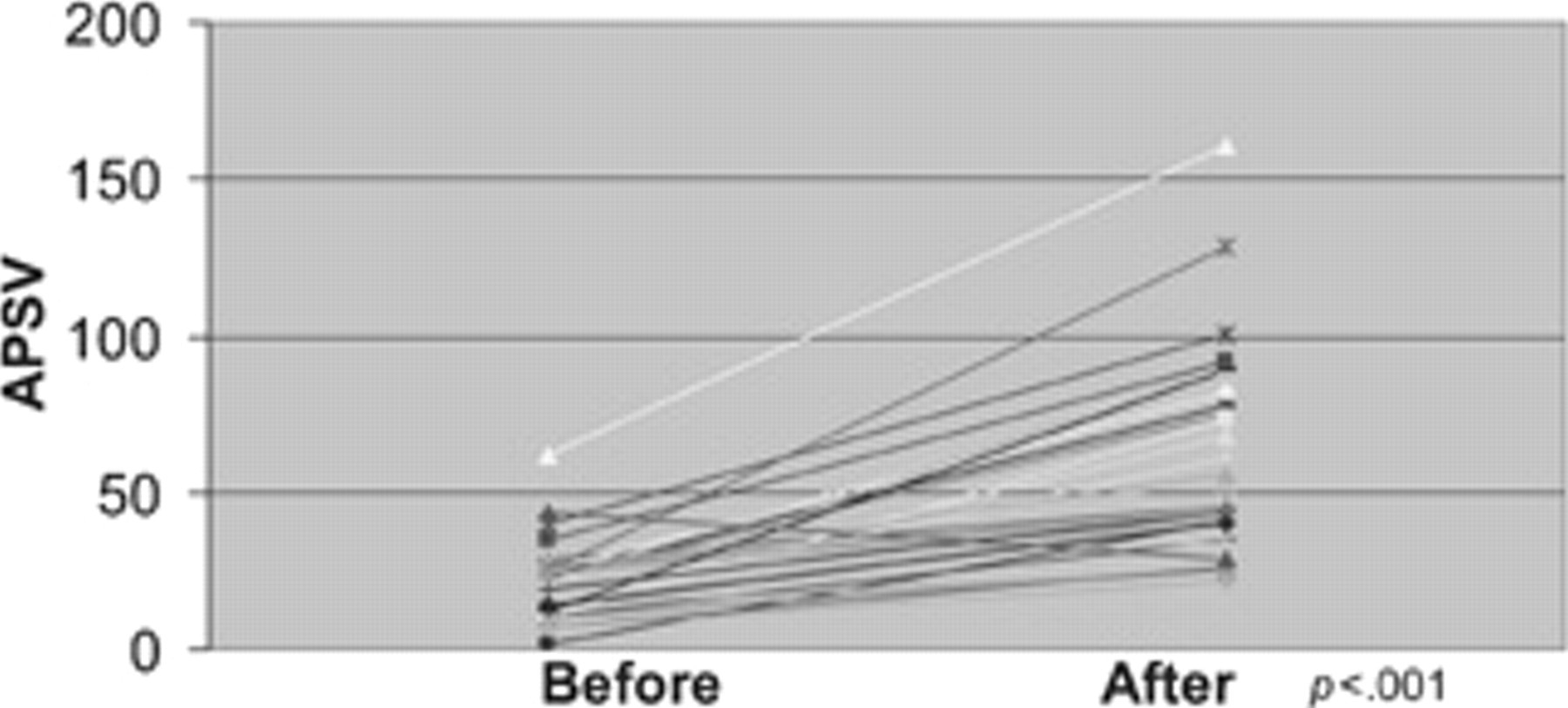
Ankle peak systolic velocity (APSV) before and after revascularization for a subgroup of 30 patients. Median and interquartile range (Q1–Q3) were 20.4 cm/s (12.4–26.3) versus 48.8 cm/s (36.1–80.8) before and after revasclarization, respectively. Paired analysis was performed using the Wilcoxon test, p < .0001.
Discussion
Many noninvasive methods have been described to predict wound healing or nonhealing of foot lesions in diabetic patients. These include ankle-brachial pressure, 10 toe-brachial pressure, 10,11 transcutaneous oxygen, 11 skin perfusion pressure, 12–14 radioisotope clearance, 15 photoplethysmography, 16 and laser Doppler ultrasonography. 13 The utility of the ankle-brachial pressure measurement is limited by the fact that a significant proportion of diabetic patients suffer some degree of arterial wall calcification, which may render ankle pressure measurements impossible to measure or falsely elevated. 17,18 The utility of toe pressure measurement is also limited by the possibility of calcification of the digital arteries in the diabetic patients and by the ulceration or tissue necrosis of the toes of many patients, which may render toe pressure measurements inaccurate or impossible. 7 APSV is not affected by such limitations. 8
Skin perfusion pressure at a cutoff value of 40 mm Hg has a sensitivity of 72% and a specificity of 88% in predicting wound healing. 12 Transcutaneous oxygen measurements at a cutoff value of 34 mm Hg have a sensitivity of 78.6% and a specificity of 83% in predicting wound healing. 19 The sensitivity and specificity of APSV in our study compare favorably with previously reported results of skin perfusion pressure and transcutaneous oxygen.
In this study, APSV was used to predict nonhealing and was not used to predict healing of foot lesions. If foot perfusion is significantly impaired as indicated by a low APSV, healing is unlikely. However, if foot perfusion is adequate, as indicated by a high APSV, wound healing may or may not be achieved because healing may be impaired as a result of other factors, such as infection, diabetes, renal impairment, liver impairment, and nutritional status. Therefore, it would be more appropriate to use the parameter of APSV to predict nonhealing rather than healing.
All patients included in this study were diabetic, as required in the inclusion criteria. Using the ROC curve, it was found that the cutoff value of 35 cm/s gives the highest specificity and sensitivity to predict nonhealing in this cohort of patients. It is possible that the cutoff value may be lower in nondiabetic patients. Further study is required to investigate this point.
In diabetics, both the anterior and the posterior tibial arteries are often diseased or totally occluded, the peroneal artery being the main blood supply to the foot. The peroneal artery supplies the foot through its two terminal branches, which are usually connected to the most distal segments of the anterior and posterior tibial arteries. Those are often patent, even if the two tibial arteries are otherwise severely diseased or occluded. By calculating the APSV through measurements of peak systolic velocity in the most distal segments of the anterior and posterior tibial arteries, which take their supply from the two terminal branches of the peroneal artery, the APSV effectively reflects the foot perfusion supplied through the peroneal artery.
In a 20-year literature review to assess complete ulcer healing as an end point, Hoffmann and colleagues found that this end point was reported in only 0.9% of 1,914 studies involving critical limb ischemia. 20 They questioned the appropriateness of complete ulcer healing as an end point. In this study, we used adequate healing as an end point. This is in agreement with the majority of studies reporting on wound healing in diabetic patients.
The limitations of this study are the relatively small number of limbs studied and that the new parameter APSV was used by its own inventors to investigate its value in predicting wound nonhealing. Larger studies by other groups are suggested.
Conclusion
The findings of this study suggest that APSV has a high degree of accuracy in predicting nonhealing of diabetic foot lesions in this group of patients. Larger studies are required to further support this conclusion.
Footnotes
Acknowledgments
We acknowledge Ruth Kouides, MD, chairman of ViaHealth Clinical Investigation Committee, Rochester General Hospital, for reviewing the statistical analysis.
Financial disclosure of authors and reviewers: None reported.
Presented at the XXI Meeting of the European Society for Vascular Surgery, Nice, France, September 2008.