
Abstract

SESSION I: Will Endovascular Technology Indulge All Thoracic Pathology?
Venue: Main Hall
Moderators: Larry Hollier, Mark Morasch
Mark Morasch
Northwestern Memorial Hospital, Chicago, Illinois
Ninety-one percent returned for the protocol-required 30-day visit. There were four deaths (bowel ischemia, respiratory failure, AAA rupture, cardiac tamponade), for a 30-day all-cause mortality of 2.7%. The major adverse event rate was 22% (including two strokes, six cases of paraplegia/paresis), and the major device-related event rate was 7.3%. Eleven subjects required intervention within 30 days for device-related events.
Dieter Raithel, Lefneg Qu
Medical Centre of Nuremberg, Nuremberg Germany
Military Medical University, Shanghai, China
Precise endograft placement in the thoracic aorta is challenging due to the special local anatomy and unique hemodynamic blood flow. We are employing many techniques together to launch the endograft precisely to the target location: various debranching techniques to extend the proximal landing zone, magnified imaging with full exposition of the supra-arch branches and the proximal landing area to achieve a clear and accurate view, screen markers of the landing target for guidance of deployment, 1 to 2 cm proximally to the cranial landing marker before launching in case of any displacement, and steady deployment of the endograft in hypotensive status or within the temporary heart asystole period induced by intravenous adenosine administration. If a balloon angioplasty or a proximal cuff is inevitable, the above-mentioned techniques should be repeated. Debranching techniques were used in 76 cases, and the technical success rate was 100%. Ten cases had immediate proximal type I endoleak, six cases were remedied with proximal cuff, two cases were rescued with trilobe balloon, and two were left untreated. Neurologic complications occurred in eight cases, including five strokes and three paraplegia (two in type IV aneurysms and one transient in type III). The total mortality rate was 6.5%.
Our single-center results have proved the combined techniques for precise thoracic endograft placement to be reliable, effective, simple, and practical.
Jean Pierre Becquemin
University of Paris XII, Henri Mondor Hospital, Creteil, France
Endovascular repair of the aortic arch remains a surgical challenge. This report deals with the lessons drawn from a series of 50 consecutive cases.
Preoperative data, technical success rate, survival, and survival free of major adverse events were prospectively assessed. An all-inclusive composite end point was calculated by toting the 30-day mortality, the stroke rate, and the presence of type I endoleak. These items were compared within three groups divided according to the proximal landing zone (0, 1, or 2 of the Ishimaru classification).
Pre- and postoperative CT scans were analyzed from an Advantage windows console to assess graft apposition and endoleak according to the landing zone and arch angulations.
W. Anthony Lee
University of Florida, Gainesville, Florida
Vincente Riambau
Thorax Institute, University of Barcelona, Barcelona, Spain
The neurologic complications of thoracic endovascular aorta repair (TEVAR), stroke and spinal cord ischemia, are serious problems and carry important personal, family, and social impacts.
Larry Hollier
LSU Health Sciences Center, New Orleans, Louisiana
Paraplegia remains the most worrisome potential complication of endografting of the thoracic aorta. We have seen neurologic injury occur in 3% of the patients who received thoracic or thoracoabdominal endografts. Interestingly, there was no case of acute paraplegia; all presented as delayed onset, one at 24 hours, one at 3 days, and one after 6 weeks.
Neurologic injury can occur from several causes following placement of thoracic endografts. The most obvious would be due to the endograft covering the orifice of a critical intercostal artery that does not have adequate collateral connections along the course of the anterior spinal artery. Another cause of neurologic injury may be related to reduced perfusion pressure of the spinal cord due to intra- or postoperative hypotension, perhaps in the setting of reduced spinal artery pressure from coverage of contributing collateral intercostals. It has been postulated that an additional etiology of delayed-onset paraplegia after TEVAR could be late closure of a type II endoleak with resultant loss of critical arterial supply.
A less well-recognized spinal cord injury is secondary injury due to activated cytokines, as is sometimes seen in patients who undergo visceral debranching at the time of placement of TEVAR.
Vincente Riambau, M. Da Rocha, C. Diaz-Duran, F. Urgnani, X. Montaña
Thorax Institute, University of Barcelona, Barcelona, Spain
W. Anthony Lee
University of Florida, Gainesville, Florida
Peter Naughton, Heron E. Rodriguez, S. Jon, Mark Eskandari, M.D. Matsumura, Melina R. Kibbe, D. Mark, Scott A. Resnick, Mark Morasch, William H. Pearce
Division of Vascular Surgery, Northwestern University, Chicago, IL Northwestern Memorial Hospital, Chicago, IL
Vincente Riambau
Thorax Institute, University of Barcelona, Barcelona, Spain
The therapeutic objective of type B dissection should be to prevent or fix malperfusion, aortic expansion, and/or rupture. Major critical issues have been described regarding thoracic endografting technology in aortic dissection. Stent conformability in the inner curvature of the arch, accurate stent radial force and smooth/atraumatic design, controlled deployment, and fixation are the most relevant limitations of current thoracic endografts. Therefore, to develop dedicated endografts for type B dissections seems to be mandatory before determining if thoracic endografting techniques are useful or not, especially in acute phases.
The Relay NBS Registry is designed to capture multicenter results for the treatment of nonchronic type B pathologies. These data will include institutional procedure variation, acute technical results, clinician input on device performance, and acute and moderate clinical input. The study will include the support of five to seven institutions throughout Europe. The goal will be to capture five procedures at each institution. Thus, the study will capture a total of 25 to 35 patients. Regular follow-up will be conducted at 1-, 6-, 12-, and 24-month intervals. Preliminary clinical experience will be presented at the time of the International Congress XXI.
W. Anthony Lee
University of Florida, Gainesville, Florida
Tara Mastracci, Roy K. Greenberg
Department of Cardiovascular Medicine, Cleveland Clinic Foundation, Cleveland, Ohio
08:36 DISCUSSION
SESSION II: The Unknown Knowns in AAA Repair
Venue: Main Hall
Moderators: Sherif Sultan, Frank Veith
Mark Morasch
Northwestern Memorial Hospital, Chicago, IL
Greg Modrall
Dallas Veterans Affairs, Dallas, Texas
Frank Veith
The Cleveland Clinic, Cleveland, Ohio, and New York, New York
Despite all therapeutic improvements, open surgical treatment of ruptured abdominal aortoiliac aneurysms (RAAAs) has a high mortality.
Our experience and that of several other centers throughout the world have shown that endovascular techniques, including the use of aortic endografts, have reduced the 30-day mortality of treatment for RAAAs to 10 to 18%. However, some groups have been unable to achieve these good results, and comparative controlled studies have failed to demonstrate the benefit of EVAR in the ruptured AAA setting.
It is our belief that these poorer results for EVAR are due to the failure to use certain strategies, adjuncts, and techniques that can contribute and have contributed to reduced mortality and improved outcomes. These include the following: (1) hypotensive hemostasis or restriction of fluid resuscitation, allowing the systolic blood pressure (BP) to fall to levels as low as 50 mm Hg without giving fluids; (2) placement, preferably via a femoral approach under local anesthesia, of a guidewire and catheter in the supraceliac aorta; (3) using this catheter, arteriography is performed to define infrarenal aortic neck and iliac anatomy and to determine suitability for endovascular graft repair of the aneurysms using either an aortounilateral graft or a bifurcated modular graft; (4) in the event that circulatory arrest or collapse (BP < 40 mm Hg) occurs, a large (14–16F) hemostatic sheath is placed via one femoral artery into the supraceliac aorta; (5) a large compliant balloon is inserted through this sheath and inflated with dilute contrast under fluoroscopic control to occlude the supraceliac aorta; the balloon position is supported by leaving the hemostatic sheath in place; (6) the position of the renal arteries is determined, and an aortic endograft is then deployed via the opposite femoral artery while the inflated supraceliac balloon is left in place; (7) if an aortounilateral graft is used, the balloon is then deflated and removed through its insertion sheath; (8) if a modular bifurcated graft is used, the main body is fully deployed, and a second compliant balloon is placed within the body of the graft and inflated; (9) the supraceliac balloon is deflated and removed through the large sheath, which is then removed; (10) the remainder of the operation is completed; this includes common iliac occlusion and a femorofemoral bypass if an aortounilateral graft is used; (11) if abdominal compartment syndrome is suspected because of the need for increased ventilatory pressures or elevated bladder pressure, a minilaparotomy is performed with evacuation of the retroperitoneal hematoma; (12) the abdomen may have to be left open and sealed with a VAC dressing.
Use of these methods and techniques will contribute to improved survival with endograft treatment of RAAAs and eliminate all controversy that endovascular methods and grafts should be used to treat them whenever possible. Proof that a randomized trial is not necessary is the large number of RAAA patients who survive EVAR despite being totally unsuitable for open repair.
Craig Kent
University of Wisconsin Hospital, Madison, Wisconsin
We recently embarked on a study to evaluate trends in hospitalizations, treatment, and mortality of ruptured abdominal aortic aneurysms (rAAAs) in the US Medicare population. The Medicare inpatient database (1995 through 2006) was reviewed for patients with rAAA and AAA by using International Classification of Disease (9th Clinical Modification) codes for rAAA and AAA. Proportions and trends were analyzed by chi-square analysis, continuous variables by t-test, and trends by the Cochran-Armitage test. During the study period, hospitalizations with the diagnoses of rAAA declined from 23.2 to 12.8 per 100,000 Medicare beneficiaries (p < .0001), as did repairs of rAAA (15.6 to 8.4 per 100,000; p < .0001). No change was observed in AAA elective repairs. The 30-day mortality rate after open repair of rAAA decreased by 4.9% (from 39.6% to 34.7%; p = .0007 for trend) for the age group 65 to 74 and by 2.4% (from 52.9% to 50.5%, p = .0008) for the age group ≥ 75. Perioperative mortality after endovascular repair diminished by 13.6% (from 43.5% in 2001 to 29.9% in 2006; p = .0020). Mortality among women was higher than among men (51.1% vs 40.0% in 2006). The demographics of patients treated for rAAA changed to include a greater proportion of women and patients aged ≥ 75 years. A significant decrease has occurred in the number of patients who have a diagnosis of rAAA and undergo treatment, but there has been no change in repairs of AAA. The perioperative mortality rate has improved due to the introduction of endovascular repair and a small but progressive improvement in survival after open repair for patients aged 65 to 74 years.
Jan Hoist, Tim Resch, Bengt Lindblad, Krassi Ivancev, Sven Mathies-sen, Katarina Björses, Björn Sonesson, Nuno Dias, Martin Malina Malmö University Hospital, Malmö, Sweden
The 30-day and 1-year mortality was 27% and 37%, respectively. One-year aneurysm-related mortality was 33%. Twenty-eight percent of patients required reinterventions during the follow-up. The use of an aortic occlusion balloon and the presence of cerebrovascular disease or obstructive lung disorder correlated significantly with 30-day mortality in the multivariate analysis.
Sherif Sultan, Niamh Hynes
Western Vascular Institute, Galway, Ireland
Frank Lederle
VA Medical Center, Minneapolis, Minnesota
We conducted a systematic review of randomized trials to determine the comparative effectiveness of treatment options of nonruptured abdominal aortic aneurysm (AAA), including active surveillance, open repair, and endovascular repair. We also conducted a separate review of studies on cost-effectiveness. Two trials compared open repair with surveillance for small AAA. Open repair did not significantly improve all-cause or AAA-related mortality. Four trials have reported comparisons of open with endovascular repair. Endovascular repair reduced 30-day mortality but not midterm (up to 4 years) mortality. In the only trial to compare endovascular repair with observation in patients unfit for open repair, endovascular repair did not reduce all-cause or AAA-related mortality, but high crossover and procedural mortality rates complicate interpretation. For small AAA, immediate open surgery costs more than surveillance. All studies found that endovascular repair costs more than open surgery. Among patients with large AAA considered unfit for open surgery, endovascular repair costs more than no intervention. Long—term trial data comparing endovascular with open repair are needed, as is another trial comparing endovascular repair with observation in high-risk patients.
William Boden
University at Buffalo Schools of Medicine and Public Health, Buffalo General Hospital, Bufalo, New York
Vincente Riambau
Thorax Institute, University of Barcelona, Barcelona, Spain
EVAR has demonstrated its early benefits when compared with open surgery. However, the reintervention rate darkens the potential for EVAR expansion. Complications such as migration or endoleaks should be detected during the follow-up. A surveillance program must be applied after EVAR to avoid fatal adverse events.
The most accepted schedule, as for other vascular procedures, is 1,3, 6, 12, and 18 months and lifelong yearly assessment. Minor variations of this schedule have been applied to the major registries and clinical studies.
Clinical status and physical examination, ankle-brachial index, contrast-enhanced computed tomography, and plain x-ray with four projections are the regular components for a minimum surveillance visit.
Some concern is related to the adverse events derived from the repetitive exposition to radiation and iodine contrast. To avoid these inconveniences, other test modalities have been suggested: duplex scan, magnetic resonance, and pressure sensors.
“Close” EVAR surveillance can be recommended when any aneurysm increases or type II endoleak without an aneurysm increases proximal or distal migrations > 5 mm where detected. A reduction of elapsed periods, every 3 months, can be applied to prevent and treat any major complication.
In contrast, a “relaxing” EVAR surveillance can be used when some findings are observed. For example, a complete shrinkage with complete device integrity can be followed yearly by ultrasound and plain x-rays with a systematic protocol. Or a tendency to shrinkage with device integrity can be followed yearly with ultrasound and CT/MRI alternatively and always with plain x-rays.
We still need new improvements from the industry to provide new devices with better fixation and durability. New endografts must be as durable as the life expectancy of our patients, to reduce cost derived from the surveillance and reinterventions and even to expand indications to low-risk patients. In the meantime, a basic surveillance program should be lifelong applied to all EVAR patients with minimal deviations according to the findings.
Carlos Timaran
Dallas Veterans Affairs, Dallas, Texas
Mark Morasch
Northwestern Memorial Hospital, Chicago, Illinois
Stewart Walsh
Cambridge Vascular Unit, Cambridge, United Kingdom
10:16 DISCUSSION
10:30 COFFEE BREAK
Venue: Exhibition Hall
SESSION III: Is the Complex Aortic Neck a True Reality or a Virtual Dilemma?
Venue: Main Hall
Moderators: Ali Aburahma, Ralf Kolvenbach
Ralf Kolvenbach, Edward Shifrin, Wesley Moore
Augusta Hospital Duesseldorf, Duesseldorf, Germany
Open and laparoscopic stapling has largely replaced a hand-sewn anastomosis in colorectal surgery. In aortic surgery, the hand-sewn anastomosis is still the gold standard. Any stapling device must perform equally to or better than sutures. A minimally invasive approach with laparoscopic exposure requires a device that facilitates performance of the aortic anastomosis with the help of a mini-incision. A wider use of laparoscopic aortic techniques requires an expeditious way to perform the aortic anastomosis since laparoscopic suturing is still considered to be a major obstacle.
The sterile single-use stapler consisted of two main parts: the head and the handle. The head of the stapler contains a round cassette that is preloaded with 10 clips. The special feature of the clips is their geometric configuration that opens to both sides, so every clip fixes the graft to the aortic wall in two points. The stapler was provided in three diameters (16, 18, or 20 mm).
The main advantage of the mechanical L-OAS device in laparoscopic aortic repair over the conventional suturing is the significant decrease in clamping time that, together with the other advantages of the mechanical stapling over the suturing process, may only contribute to decreasing the rate of postoperative complications.
Michael Horrocks
Bath Clinic, Bath, United Kingdom
Dieter Raithel, Lefneg Qu
Medical Centre of Nuremberg, Nuremberg, Germany
Venkatesh Ramaiah
Arizona Heart Institute, Phoenix, Arizona
Ralf Kolvenbach
Augusta Hospital Duesseldorf, Duesseldorf, Germany
Graft migration and other device-related problems are more frequent in AAA patients with a complicated neck. We wanted to evaluate the performance of a balloon-expandable stent graft in these cases. Complicated aortic neck morphology was defined as a combination of short (< 15 mm) and angulated (> 45°) necks with or without circumferential thrombus. Severe neck angulation was defined as more than 60°.
The VI-Datascope graft consists of an aortounifemoral polytetrafluoroethylene (PTFE) graft sutured to a proximal balloon-expandable stent. The length of the graft is 40 cm; thus, the distal end of the graft always protrudes through the ipsilateral arteriotomy and can be cut to an appropriate length for each patient. The graft-covered of the graft was deployed just below the level of the lowest renal artery. The proximal bare metal stent was deployed in the suprarenal area. An endoluminal hand-sewn anastomosis was performed between the aortounifemoral limb and the distal external iliac or the common femoral arteries. An occluder device was placed in the contralateral common iliac artery to prevent retrograde perfusion of the aneurysm. A femorofemoral 8 mm Dacron bypass was then performed to establish flow.
Alt Aburahma
Charleston Area Medical Center, Charleston, West Virginia
Prakash Madhavan
St James Hospital, Dublin, Ireland
Sherif Sultan, Niamh Hynes
Western Vascular Institute, Galway, Ireland
Although EVAR has been reputable as affording more favorable perioperative and long-term survival than open surgical repair (OSR), it is estimated that 50% of AAAs are anatomically unsuitable for EVAR using commercially available devices.
We aim to gauge the feasibility of extending the use of current commercially available devices for pararenal aneurysm with respect to clinical, economical, and quality of life outcomes, compared with the current standard OSR. Primary end points were aneurysm-related survival and cost per quality-adjusted life-years (QALYs).
Between 2002 and 2009, 1,769 patients with AAA were seen at our unit. Ninety-two patients had intervention for pararenal AAAs, which were reported by the radiology department as unsuitable for EVAR. Fifty-four of these had OSR and 38 had EVAR. AAAs were deemed unsuitable for EVAR if they had no normal aortic neck between the lowest renal artery and the start of the aneurysm, if there was significant thrombus at the implantation site, and if the angle between the neck and start of the aneurysm was greater than 90° and thrombus load more than 4 mm around the aortic neck.
The majority of patients were male (EVAR 87% vs OSR 76%, p = .198). The EVAR group was significantly older (74.5 vs 71.1 years, p = .034) with significantly higher mean SVS comorbidity severity scores (p < .0001) and Kertai customized probability indices (p < .001).
All procedures were done within 14 days of diagnosis. Mean aneurysm diameter was not significantly different between treatment groups (EVAR 6.0 cm vs OR 6.6 cm, p > .05). In the EVAR group, 83% of the endografts were 36 mm diameter and the mean proximal diameter of the deployed endografts was 32 mm. All open repairs were done with a diagonally placed proximal clamp, preserving flow to the highest renal artery. The renal arteries were reimplanted in four cases and the inferior mesenteric artery in one case. All OSRs were done with 16 or 18 mm silver-impregnated Dacron grafts.
Five-year aneurysm-related survival rates were higher with EVAR (100%) compared with OSR (94.4%, p > .05), although this did not reach statistical significance. Five-year freedom from secondary intervention was not significantly different between EVAR (94.1%, 95% CI 80.1 to 98.8) and OSR (100%, p > .05).
Five-year all-cause survival was significantly reduced in the EVAR group (50.4%, 95% CI 34 to 66) when compared with OSR (80.4%, 95% CI 66.9 to 89.5]) (p = .0279, h = 0.34, 95% CI 0.12 to 0.94). Five-year intervention-free survival was significantly reduced with EVAR (48.9%, 95% CI 32.7 to 65.3) compared with OSR (80.4%, 95% CI 66.9 to 89.5). However, none of the deaths in the EVAR group were aneurysm related.
Thirty-day morbidity (p < .0001), length of hospital stay (p < .0001), 5-year quality time spent without symptoms or toxicity of treatment (Q-TWiST) (p < .01), and cost per QALY (p < .01) were all significantly reduced with EVAR compared with OSR. Sensitivity analysis revealed that Q-TWiST was significantly improved with EVAR compared with OSR (p < .0032).
Endografts can be effectively used to treat difficult pararenal AAAs with enhanced long-term aneurysm-related survival, cost-effectiveness, and quality of life and significantly reduced perioperative morbidity and mortality and waiting time from diagnosis to treatment.
12:04 DISCUSSION
SESSION IV: Modular Devices: The Reality of Endoleak
Venue: Main Hall
Moderators: Mohan Adiseshiah, Dieter Raithel
Peter Naughton, J.S. Matsumura, Mark Morasch, H.E. Rodriguez, S.A. Resnick, W.H. Pearce, D.J. Amaranto, Mark Eskandari Division of Vascular Surgery, Northwestern University, Chicago, Illinois
Northwestern Memorial Hospital, Chicago, Illinois
Mohan Adiseshiah
University College Hospital, London, United Kingdom
Vincente Riambau, R. Hobo, F. Urgnani, M. Da Rocha, P. Lerut, D. Adriani
Thorax Institute, University of Barcelona, Barcelona, Spain
EUROSTAR Data Registry Center, Catharina Hospital, Eindhoven, the Netherlands
Colin Bicknell, M. Jenkins, M. W. Clark, J. Burrill, C V. Riga, R.G.J. Gibbs, M. Hamady, P. Bourke, M. Mireskandari, Nick Cheshire, J.H.N. Wolfe
Sheffield Vascular Institute, Sheffield, United Kingdom
Niamh Hynes, Sherif Sultan
Western Vascular Institute, Galway, Ireland
Our endeavor was to contrast clinical and technical outcomes of BIF versus AUI in high-risk EVAR patients.
From 2002 to 2007, 82 high-risk patients underwent elective EVAR (BIF, n = 52 [63.4%]; AUI, n = 30 [36.6%]). Mean age 74 years (BIF vs AUI, p = .835), male percentage (BIF vs AUI, 86.5% vs 76.7%, p = .260), and mean aneurysm diameter (BIF vs AUI: 5.4 cm vs 5.3 cm, P = .514).
The predicted probability of receiving AUI was tabulated for all patients by using multiple logistic regressions to control for SVS comorbidity and anatomic severity scores. We used propensity scoring to adjust for baseline characteristics and selection bias by matching covariables, creating a pseudorandomized control design. Primary end points were 30-day mortality, 4-year survival, and 4-year intervention-free survival.
Mean proximal endograft diameter was significantly lower with BIF (29.3 vs 30.9, p = .031). Mean number of devices used was similar (3.0 vs 3.4, p = .165).
BIF and AUI had similar 30-day mortality (1.9% vs 0%, p = .453), 4-year all-cause survival (72.1% vs 74.0%, p = .882, h = 0.92, 95% CI = 0.30–2.78), and 4-year aneurysm-related survival (98.1% vs 100%, p = .448). There was no graft migration or structural failure. There was no intervention required for type II (23.1% vs 36.7%, p = .191). Four-year limb thrombosis rate (7.6% vs 10%, p = .723) and 4-year intervention-free survival (BIF 89.8% vs AUI 85.9%, p = .612, h = 0.71, 95% CI = 0.18–2.76) were similar. Four-year femorofemoral crossover patency rate is 92.6% (95% CI = 75.6–98.6).
There were no significant differences in procedure time, mean blood units, and change in estimated glomerular filtration rate between groups (p > .05). Length of stay/HDU (4.2 vs 7.4, p = .021/.87 vs 1.2 days, p = .656) were similarly low, with the majority of patients discharged directly home (BIF vs AUI: 92% vs 80%, p = .103).
By using propensity scoring for the primary end points, the proportions of AUI patients were equal to those of BIF for all levels of probability and were unchanged as the probability of AUI increased.
We established at 4 years that clinical and technical outcomes were not compromised with AUI compared with BIF in this high-risk cohort.
12:55 DISCUSSION
13:00 LUNCH
Venue: Restaurant
SESSION V: The Great Aortic Debates
Venue: Main Hall
Moderators: Venkatesh Ramaiah, Frank Veith
Piergiorgio Cao, Fabio Verzini, Giuseppe Panuccio, Gianbattista Parlani, Lydia Romano, Paola De Rango
University of Perugia, Ospedale S. Maria della Misericordia, Perugia, Italy
Frank Veith, Manish Mehta, Frank Criado, Dieter Raithel
The Cleveland Clinic, Cleveland, Ohio, and New York, New York
Albany Medical College, Albany Medical Center Hospital, Albany, New York
Union Memorial Hospital-MedStar, Baltimore, Maryland
Medical Centre of Nuremberg, Nuremberg, Germany
Rodney White
Harbor-UCLA Medical Center, Los Angeles, California
Aortic dissection is a frequently occurring pathology with the natural history, including a significant number of severe complications, including stroke, aortic valve insufficiency, cardiac tamponade, and aortic rupture. Although surgical intervention remains the primary treatment for ascending (Stanford type A) aortic dissections, the treatment of both acute and chronic descending aortic dissections (Stanford type B) is still controversial despite advances in surgical and medical therapy.
In the acute phase, most institutions treat descending aortic dissections (DTD) with medical therapy and reserve surgical intervention for life-threatening complications such as uncontrolled hypertension, ongoing chest pain despite medical therapy, progression of dissection, aneurysmal enlargement, rupture, and/or extremity ischemia. This selected approach has resulted in mortality rates of 25% for medical therapy and approximately 35% for open surgical procedures but can exceed 50% when organ ischemia is present prior to surgery.
When acute descending aortic dissections are successfully treated with medical therapy, the dissections are considered chronic after 14 days. Nearly one-third of chronic dissections are at risk of further dissection or aortic rupture or require surgery for aneurysmal enlargement of the false lumen within 5 years. The survival rate has improved with operative intervention; however, thoracic aortic aneurysm repair is associated with high morbidity and mortality. Significant risk of postoperative paraplegia and other complications, including renal failure and long recovery periods related to comorbid medical conditions, are frequently encountered.
Endovascular treatment of acute and chronic descending aortic dissections has historically been limited to fenestration of the aortic septum, separating the true and false lumen to increase flow to ischemic visceral arteries and lower extremities. In the early 1990s, Dake et al reported the application of endograft techniques for treatment of DTD by covering the proximal entry site in Stanford B dissections with endografts diverting flow from the false lumen to the true lumen. The initial application of this technology has been very promising from several perspectives, with the benefit in acute dissections being alleviation of pain, relief of visceral and peripheral ischemia related to malperfusion, and decompression of the false lumen to control of bleeding. Exclusion of the entry site promotes a significant rate of false lumen thrombosis and dissection regression in the first 6 to 12 months following exclusion. A major benefit of the endovascular treatment of acute and chronic dissection has been reduction in the mortality rate and incidence of paraplegia compared with surgical repairs. Complications including renal failure and long-term recovery have been diminished, with the incidence of stroke remaining a low but significant complication. Exclusion of infrarenal aneurysmal components of the dissection has been more challenging, with delineation of the optimal treatment awaiting further advances.
Significant ongoing investigation is required to determine optimal indications for endovascular treatment of descending thoracic aortic dissections as the endovascular alternative has proven to be possible, with low mortality and paraplegia rates compared with the medical or surgical alternative. Although the indication for treatment of acute DTD is reserved for complications following failure of medical management, some studies suggest a benefit for endovascular exclusion of most acute lesions even with symptoms if late complications of chronic dissections can be avoided by regression of the dissection. Concurrent cohort and/or randomized clinical studies are indicated to compare endograft treatment of descending thoracic aortic dissections with contemporary medical and surgical treatment, with initial observations being that this alternative new method offers significant advantages.
Venkatesh Ramaiah
Arizona Heart Institute, Phoenix, Arizona
Hazim J. Safi
University of Texas Medical School, Memorial Hermann Hospital, Houston, Texas
Timothy Chuter, Linda Reilly
UCSP Medical Center, San Francisco, CA
14:48 DISCUSSION
SESSION VI: Viseral Arteries: An Inconvenience in the Endovascular Era?
Venue: Main Hall
Moderators: Jerry Goldstone, James Stanley
Greg Modrall, Eric B. Rosero, Carlos Timaran
Dallas Veterans Affairs, Dallas, Texas
Peter Schneider
Hawaii Permanente Medical Group, Honolulu, Hawaii
Renal artery stenting is going through an intensive reevaluation. The problem is not that renal artery stenting does not work, it is that we do not know how to select the patients who will be helped the most. We do not have adequate trial data, and ASTRAL and CORAL may not provide it. In available studies, there are some cures and many with improved hypertension and subsets of patients identified that appear to benefit; recurrent flash pulmonary edema, renal occlusion or preocclusive stenosis, severe bilateral renal artery stenosis, global renal ischemia, deteriorating renal function with no other cause. Among the procedures we do, it is the biggest mismatch between the angiographic result and predicted clinical result. The best test we have, arteriography, is an anatomic test, not a physiologic one, and it can harm the organ we are trying to evaluate. We do not know exactly what kind of vascular pathophysiology we are trying to tackle; whether it is embolic or a perfusion deficit or both. When you pass on the revascularization option, it has major long-term implications. Kidneys have less collateral flow and fewer potential collateral pathways than any other organ, except for possibly an isolated cerebral hemisphere. When someone gets to the point of severely diminished GFR, they are much less tolerant of everything, including any type of challenge and even some medications. Re-generative capacity of the kidney once function is lost is poor. We are trying to apply end points that are not sensitive enough, the major cardiovascular events. The issue goes back to basics: better to have open arteries than closed arteries and better to have two kidneys than one or one kidney than none.
Greg Modrall
Dallas Veterans Affairs, Dallas, Texas
Mark Davies
Methodist DeBakey Heart and Vascular Center, Houston, Texas
Endovascular interventions for atherosclerotic and nonathero-sclerotic renal artery stenosis are commonplace. The efficacy of these interventions is currently under review. The goals of therapy are dependent on the indication for therapy. Renal angioplasty for FMD is appropriate and has a high cure and improvement rate. In atherosclerotic renal disease, indications are hypertension, ischemic nephropathy, and congestive heart failure. In hypertension, cure or improvement with > 2 medication drops are required. The recent ASTRAL study has shown no significant clinical benefit of renal angioplasty over best medical therapy. In chronic renal insufficiency, cure or improved renal function is the goal. Patients whose eGFR is dropping appear to benefit most, with a greater number showing improvements in renal function and parenchymal preservation. Those with established disease do not appear to have a cost-effective result. In patients with congestive heart failure, left ventricular remodeling and a decrease in the number of hospital admissions for decompensaion are the goal. Small single-center studies suggest that both goals can be achieved after renal angioplasty, but no consensus has been achieved in the literature. Renal angioplasty and stenting is only justified in select patients and where cost-effectiveness has been demonstrated. Current randomized trials are demonstrating that renal intervention is not superior to best medical management.
James Stanley
University of Michigan, Ann Arbor, Michigan
Jeffrey Indes, Richard Gusberg, Bauer Sumpio, Alan Dardik, Bart Muhs
Columbia College of Physicians and Surgeons, Columbia University Yale-New Haven Hospital, Connecticut
Yale University School of Medicine
15:56 DISCUSSION
SESSION VII: Optimal Medical Management
Venue: Main Hall
Moderators: Anthony Comerota, Dimitri Mikhailidis
Anthony Comerota
Jobst Vascular Center, Toledo, Ohio
Vascular surgeons have pushed the technical limits of revascularization procedures. However, the important question remains: Following a technically successful bypass, can anything more be done to preserve patency? Although this remains an area of some controversy, there is increasing consensus regarding appropriate pharmacotherapy before, during, and following infrainguinal revascularization. Preoperative platelet inhibition is important because it reduces platelet deposition on prosthetic bypasses and areas of arterial wall injury, resulting in improved patency of prosthetic bypass grafts. Intraoperative dextran is beneficial, especially in difficult infrainguinal bypasses. Combined platelet inhibition with aspirin and clopidogrel is being used with increased frequency by vascular surgeons due to the observed benefits following coronary intervention, although specific data regarding improved patency following lower extremity bypass are lacking. Anticoagulation with warfarin combined with aspirin improves the patency of both prosthetic and vein bypasses. Improved patency of saphenous grafts with the platelet ADP receptor blocker ticlopidine was found in one prospective study, suggesting that there may be a difference in outcome between platelet inhibitors, depending on their mechanism of action. Low-molecular-weight heparin also improves patients; however, its cost, risk of osteoporosis, and need for injection make this an unrealistic form of long-term therapy.
Michael Norton
Sunderland Teaching Primary Care Trust, United Kingdom
It is widely recognized that peripheral vascular disease frequently coexists with significant coronary artery disease and cerebrovascular disease. Symptomatic peripheral vascular disease carries a significant risk of death from myocardial infarction and stroke. Abdominal aortic aneurysms are also associated with increased MI and stroke risk. This session will review current evidence and guidelines for cardiovascular risk factor reduction and will also consider practical ways in which clinicians can work across traditional boundaries to further improve the management of the patient with vascular disease.
Anthony Comerota
Jobst Vascular Center, Toledo, Ohio
The use of the term “resistance” as it applies to aspirin and clopidogrel is often confusing and misleading. Primarily, a drug response should be defined in terms of biomarkers rather than clinical events since clinical events can result from numerous concomitant comorbidities. A number of in vitro tests are available to evaluate response to platelet inhibitor drugs; however, the responses reported on one test do not necessarily correlate with responses by others. Therefore, categorizing a particular patient as either responsive or resistant may be dependent upon the test used. These points need to be considered when discussing clopidogrel resistance. Numerous reports have indicated an impaired response to clopidogrel in a variety of ischemic outcomes. Most of these studies are observational and retrospective. However, several important studies performed in patients undergoing percutaneous coronary intervention indicate that clopidogrel unresponsiveness (or “resistance”) is associated with an increased chance of developing ischemic events. These observations indicate the need for prospective trials and suggest perhaps a gradual discontinuation of clopidogrel if, indeed, it is to be terminated. These observations also have risk implications when patients have clopidogrel stopped to undergo an operative procedure.
Herbert Schuster
Humboldt University
Cardiovascular disease is a major health burden and a leading cause of global mortality. Cardiovascular disease includes coronary heart disease (CHD) and cerebrovascular and peripheral artery disease and is most frequently caused by atherosclerosis, a progressive condition that may remain asymptomatic for many years, with sudden death often being the first clinical manifestation. Elevated LDL cholesterol (LDL-C) is an important contributory factor to the development of atherosclerosis and as such is recognized as a major risk factor for CHD. Consequently, LDL-C is a key therapeutic target for the prevention of CHD, with statins recommended as first-line drug treatment.
However, as many as 50% of cardiovascular events occur in apparently healthy people with normal LDL-C levels. Studies have shown that C-reactive protein (CRP), a marker of systemic inflammation, is a strong predictor of vascular risk among apparently healthy individuals and in most cases is independent of other risk factors, such as elevated cholesterol levels, age, smoking, blood pressure, and diabetes. Prospective population-based studies have shown a strong relationship between the level of CRP and risk of coronary events. Moreover, in studies involving over 8,000 patients, it has been shown that statin therapy lowers CRP in a lipid-independent fashion and that the magnitude of benefit of statin therapy is greater in the presence of high CRP levels. Retrospective analysis of an earlier study has suggested that statin therapy may prevent coronary events in people with raised CRP even when they have low to normal LDL-C levels.
In the JUPITER trial, apparently healthy individuals with low to normal levels of LDL-C but with increased CHD risk identified by elevated CRP levels were treated with rosuvastatin 20 mg for 1.9 years. LDL-C was reduced to a median level of 55 mg/dL, down from a median of 108 mg/dL. The corresponding reduction in the rate of MI, stroke, arterial revascularization, or cardiovascular death was 44% (p < .00001). The JUPITER findings raise two important questions: whether indications for statin use should be expanded and how measurement of high-sensitivity CRP should be used in clinical practice.
16:48 DISCUSSION
17:00 COFFEE BREAK
Venue: Exhibition Hall
SESSION VIII: Venous Disease Forum
Venue: Main Hall
Moderators: Anthony Comerota, Mark Meissner
Mark Meissner
University of Washington School of Medicine, Seattle, Washington
Percutaneous endothermal ablation of the saphenous veins, using either radiofrequency (RF) or laser energy, has become a widely accepted alternative to stripping. Initial success rates of up to 95% have been associated with less postoperative pain, a more rapid return to work and usual activities, and an objectively improved quality of life early after the procedure. Although safe and effective, these procedures are associated with rare complications. Some, such as skin burns, are avoidable with proper technique, whereas the clinical importance of others, such as bruising, is debatable. Other complications, such as phlebitis, nerve injuries, and deep venous thrombosis (DVT), are clinically important and do affect patient outcomes.
Some degree of inflammation accompanies all endovenous procedures. However, pain, erythema, warmth, and induration along the course of the saphenous vein occur in up to 15% of patients. Thrombotic venous occlusion has been suggested as a possible mechanism of phlebitis, and ensuring a bloodless field with leg elevation, adequate tumescence, and use of appropriate power may be important considerations in this regard. Animal models also suggest that laser ablation is associated with vein perforation and extravasation of steam and blood, perhaps leading to perivenous inflammation—an observation supported by a few comparative studies suggesting less phlebitis with RF in comparison with laser ablation.
Paresthesias secondary to saphenous nerve injury may be the most common persistent complication of endovenous ablation. Among 286 patients reported by Merchant, the incidence of paresthesias following RF ablation decreased from 15% at 1 week to 3.9% at 1 year. Although nerve injury can occur after any saphenous procedure, most improve with time and are rarely associated with long-term disability. Saphenous injuries can be minimized, even with ablation to the ankle, with meticulous attention to tu-mescent anesthesia. Clinically important nerve injuries, such as to the common peroneal nerve, may be more common after short saphenous procedures. Most of these can be avoided with careful attention to anatomy and technique.
DVT is a well-recognized complication of endovenous ablation. However, it is important to distinguish cases of saphenofemoral thrombus extension from cases of true DVT. The former are substantially more common, likely are not associated with systemically activated coagulation, appear to resolve rapidly, and have a relatively benign natural history. Although overall DVT rates have varied widely among series, a review of 4,955 patients reported in the literature suggests a weight average of 1.1%. The appropriate management of these lesions remains ill defined, and the value of routine postablation screening for asymptomatic saphenofemoral thrombus extension must be questioned. From a theoretical standpoint, the number of bleeding complications potentially generated by this practice may approach the number of pulmonary emboli prevented.
Sherif Sultan, Niamh Hynes
Western Vascular Institute, Galway, Ireland
There is a paucity of data on EVLT incidence of postoperative pain, phlegmon, and recanalization. Our aim is to compare saphenous closure rates, complications, and cost-effectiveness of high-energy endovenous laser ablation (HE-EVLA) and stab avulsion with level II saphenofemoral junction ligation and stab avulsion with upward perforate invaginate stripping (EUPIS) or conventional downward invaginate stripping (DIS)
From 2003 to 2007, of 756 consecutive VVS procedures, we matched controlled 257 patients with primary VVs, CEAP 2, 3, 4 Sixty-four had HE-EVLA under local anesthesia (88% female; mean age [± SD] = 50 ± 11 years), 130 had EUPIS under spinal anesthesia (75% female; mean age [± SD] = 52 ± 13 years), and 63 had DIS (60% female; mean age [± SD] = 50 ±15 years). HE-EVLA was performed with 14 W at 100 J/s. Major adverse events (MAEs), quality time spent without symptoms or toxicity (Q-TWiST), and cost-effectiveness were analyzed. Venous clinical severity, segmental disease, and disability scores were compared, but all were statistically similar (p > .05).
Mean follow-up was 29 ± 8.7 months, and LSV closure rate with HE-EVLA was 96.2% (95% CI 87.2–99.2) at 36 months. At 3 years, there was no incidence of recurrence with EUPIS or DIS. Mean length of stay was lower with HE-EVLA (5 hours vsl5 hours [ES] vs 18 hours [CS], p < .0001).
There was one incidence of wound infection with DIS (1.6%, p = .217). There were eight cases of severe postoperative pain in the HE-EVLT group (12.5%), two in the DIS group (3.2%), and none in the EUPIS group (p = .000154). There were two cases of phlegmonous phlebitis with HE-EVLA (3%, p = .047). All cases resolved with oral antibiotics and analgesia. Using Cox proportional hazard ratios, the only factors found to influence the rate of MAEs was use of laser (p = .005), antiplatelets (p = .012), and length of LSV (p = .025). The use of endovenous conduits reduced the risk of MAEs (HE-EVLA and EUPIS vs DIS, p <. 001).
Three-year Q-TWiST was longest with DIS (35 months) compared with HE-EVLA (23 months, p < .1) or DIS (26 months, p < .01). But there was a 30% reduction in mean cost per QALY with HE-EVLA compared with EUPIS or DIS.
The use of endovenous stripping reduces the incidence of hematoma and pain along the track of the LSV. HE-EVLT is a safe, prudent, effectual procedure; however, postoperative thermal injury pain is the foremost constraining dynamic factor with contemporary laser probes.
Anthony Comerota
Jobst Vascular Center, Toledo, Ohio
Venous leg ulcers are a significant health problem that afflicts 1% of the population at some point during their lifetime. Intermittent pneumatic compression (IPC) is widely used to prevent deep venous thrombosis. However, IPC appears to have application to a broader base of circulatory diseases. The intermittent nature of pulsatile external compression produces beneficial physiologic changes, including hematologic (fibrinolytic and intravascular coagulation) and hemodynamic (venous velocity increase) changes, and alteration of endothelial function. Data suggest that the use of IPC as an adjunct to sustained compression may be the optimal choice for treating patients with venous ulcers. However, a number of questions remain with regard to its optimal use. For example, it is not clear whether there are advantages to the particular type of compression. However, it appears clear that rapid inflation is superior to slow inflation and that IPC, which cycles at 2 to 3 times per minute (time to venous refill), is superior to long cycle times (1 cycle per 2 to 3 minutes). Findings such as these led the American College of Chest Physicians (ACCP) evidence-based guidelines (8th edition) to suggest that patients with venous ulcers resistant to healing with wound care and compression undergo IPC as adjunctive therapy (grade 2B).
Wael Tawfick, Sherif Sultan
Western Vascular Institute, Galway, Ireland
The primary end point is the proportion of ulcers healed at 12 weeks. Secondary end points are time to full healing, percentage of reduction in ulcer size, pain reduction, recurrence rates, and quality-adjusted time spent without symptoms of disease and toxicity of treatment (Q-TWiST).
Anthony Comerota
Jobst Vascular Center, Toledo, Ohio
Although anticoagulation alone is appropriate for many patients with acute pulmonary emboli (PE), those with large PE causing hemodynamic instability or pulmonary hypertension associated with right heart abnormalities benefit considerably by restoring normal outflow from the right ventricle. Ideally the goal of therapy in patients with large PE is to restore cardiopulmonary hemodynamics and avoid chronic thromboembolic pulmonary hypertension, with its associated morbidity and mortality. Chronic thromboembolic pulmonary hypertension is associated with recurrent PE < younger age at onset, large perfusion defects, and patients suffering idiopathic PE >. PE large enough to cause right ventricular dysfunction are associated with a sixfold increase in hospital mortality and a 2.4-fold 1-year mortality. Systemic thrombolytic therapy has been shown to decrease mortality, improve right ventricular function, improve pulmonary function, decrease chronic thromboembolic pulmonary hypertension, and decrease recurrent venous thromboembolism. Patients with PE that raise pulmonary artery pressures to the point of affecting right ventricular function have a high risk of chronic thromboembolic pulmonary hypertension and increased mortality. As a result, all patients with PE should be valuated with cardiac echocardiography, assessing pulmonary artery pressure and right ventricular function. Patients demonstrating abnormalities of the right heart, such as right ventricular dilation, deviation of the septum, tricuspid insufficiency, and documented pulmonary hypertension, should be considered for systemic thrombolytic therapy or catheter-based fragmentation with thrombolysis.
Mark Meissner
University of Washington School of Medicine, Seattle, Washington
Under the auspices of the American Venous Forum, the 5th Pacific Vascular Symposium was charged with reviewing the current state of knowledge with respect to acute and chronic venous disease and developing a roadmap for advancing the field over the next decade. Accordingly, an international multidisciplinary group of experts in venous disease was assembled and identified 14 priorities for future venous research (Table 1).
Significant progress has been made in some areas. Most remarkably, The ATTRACT trial, comparing pharmacomechanical thrombolysis of acute DVT with best medical management, will begin enrolling patients in early 2009. The need for dedicated venous stents has been recognized by industry and designs, are currently in development, with trials anticipated in early 2010. The ideal venous stent would be available in large diameters and long lengths, have a high radial force and low thrombogenicity, and be flexible enough to cross the inguinal ligament if necessary. A potential role for prophylactic inferior vena cava filters in high-risk bariatric and trauma patients has been recognized. Although no randomized trials have yet been funded, the American Venous Registry plans launch of an IVC filter registry in 2009 with the goal of collecting preliminary data regarding these indications. Finally, evidence-based practice guidelines for chronic venous disease are actively being developed. Meta-analyses of the data supporting thrombus removal strategies for acute DVT and the treatment of great saphenous incompetence have been completed, and guidelines are anticipated in mid-2009.
Anthony Comerota
Jobst Vascular Center, Toledo, Ohio
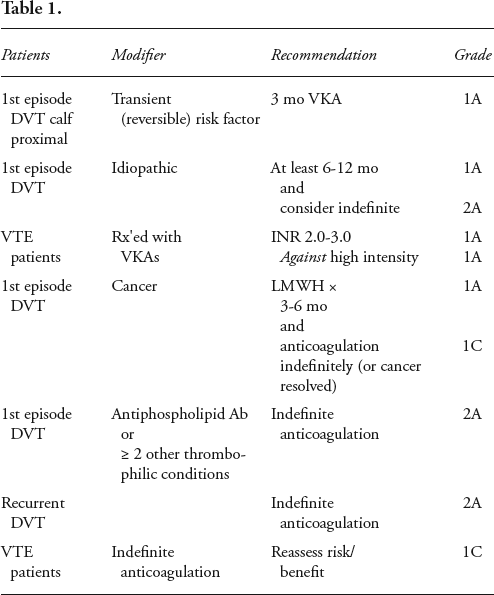
The purpose of early anticoagulation after acute deep venous thrombosis (DVT) is to stop thrombus propagation, reduce the risk of pulmonary embolism, and reduce recurrent venous thromboembolic events if anticoagulation is continuously therapeutic. Over the long term (< 1 week), the purpose of anticoagulation is to reduce recurrences. Studies evaluating the duration of anticoagulation for DVT demonstrate the longer the better! Current recommendations by the American College of Chest Physicians (ACCP) for anticoagulant therapy for DVT are listed in Table 2.

Gerry O'Sullivan
Department of Interventional Radiology, University College Hospital, Galway, Ireland
18:04 DISCUSSION
SESSION IX: Miscellaneous Topics: From Vascular Access to Wound Closure
Venue: Main Hall
Moderators: Theodore Saad, Peter Schneider
Peter Schneider
Hawaii Permanente Medical Group, Honolulu, Hawaii
Arterial access using the upper extremity is an essential maneuver in the scope of an active endovascular practice. The indications for upper extremity access are hostile femoral puncture site, diseased or tortuous approach artery (between femoral puncture and target site), favorable configuration of the pathway to the target artery (eg, visceral, renal), and as an alternative approach when unable to cross the lesion from a femoral approach (eg, subclavian or iliac occlusion). Upper extremity arterial access has traditionally been considered to have a higher complication rate than routine femoral access. In addition, the complication of brachial neuropathy related to a brachial sheath hematoma is one that may cause significant disability when it occurs. Several advances have occurred that have made percutaneous upper extremity access safer. Portable ultrasound may be used to safely guide the puncture. Micropuncture technique permits entry with a 21-gauge needle and a 4F tapered dilator. Better sheaths (low profile, tapered) help minimize the risk of injury. Pretreatment definition of anatomy using CTA, MRA, or duplex also helpschoose the best approach prior to arteriography. Advantages are as follows: it provides an alternative to femoral access, it may be the only access site that permits a successful intervention, the entire extremity can be covered with pressure dressing after hemostasis, and the patient is released with no deleterious effect on mobility. Disadvantages include the lack of closure device availability, sheath size limitations, and issues related to nerve compression. Approximately 15% of cases are performed via the upper extremity in our practice. Upper extremity access has become safer, offers an option that may serve an adjunctive role, and should be included in the standard care of vascular patients
Simon Cross, Z. Khan, A. Ryan, H. Prins, A. Quinn, I. Kelly, F. Walker, S. Leavey
Waterford Regional Hospital, Waterford, Ireland
Results: To be presented.
Theodore Saad
Nephrology Associates PA., Newark, Delaware
Cephalic arch stenosis occurs frequently in upper arm brachiocephalic fistulae. This may occur due to the unique anatomy at this site and/or local hemodynamic factors. Angioplasty is commonly employed as “first-line” therapy for cephalic arch stenosis. High-pressure balloon inflation is often required. Balloon oversizing is important, utilizing successively larger balloon diameters over time. Angioplasty results vary, with significant risk for vein rupture, recoil, and early restenosis. Clinical features of cephalic arch stenosis have been described by Rajan (JVIR 2003).
Stents may be used for treatment of cephalic arch stenosis. The anatomy is challenging due to the sharply curved arch and near-right angle junction with the axillary vein. A stent of appropriate type, diameter, and length must be deployed without adversely impacting on normal axillary or cephalic vein. Recurrent stenosis within bare metal stents is common. Stent grafts may reduce instent restenosis and prolong treatment-area patency. A controlled trial by Shemesh (JVS 2008) demonstrated more rapid restenosis in bare metal stents compared with stent grafts placed in the cephalic arch.
Surgical revision is an alternative to angioplasty or stenting. Local patch repair is technically difficult, and outcomes have not been reported. Often a new outflow pathway can be constructed from the cephalic to the axillary vein, eliminating the cephalic arch. This may be accomplished by cephalic vein “turndown” with vein-to-vein anastomosis or by using a nonautogenous interposition graft. Stenosis of the revised outflow commonly occurs. Although no advantage of surgery has been demonstrated in controlled trials, in some cases, surgical revision may provide superior outcomes to angioplasty or stenting.
Mark Davies
Methodist DeBakey Heart and Vascular Center, Houston, Texas
Endovascular interventions for atherosclerotic and nonathero-sclerotic renal artery stenosis are commonplace. The efficacy of these interventions is currently under review. The goals of therapy are dependent on the indication for therapy. Renal angioplasty for FMD is appropriate and has a high cure and improvement rate. In atherosclerotic renal disease, indications are hypertension, ischemic nephropathy, and congestive heart failure. In hypertension, cure or improvement with > 2-medication drop is required. The recent ASTRAL study has shown no significant clinical benefit of renal angioplasty over best medical therapy. In chronic renal insufficiency, cure or improved renal function is the goal. Patients whose eGFR is dropping appear to benefit most, with a greater number showing improvements in renal function and parenchymal preservation. Those with established disease do not appear to have a cost-effective result. In patients with congestive heart failure, left ventricular remodeling and a decrease in the number of hospital admissions for decompensaion are the goal. Small single-center studies suggest that both goals can be achieved after renal angioplasty, but no consensus has been achieved in the literature. Renal angioplasty and stenting is only justified in select patients and where cost-effectiveness has been demonstrated. Current randomized trials are demonstrating that renal intervention is not superior to best medical management.
Dasa Kovacic, Wael Tawfick, Sherif Sultan
Western Vascular Institute, Galway, Ireland
The most common wounds were groin wounds (n = 11, p = .019), abdominal wounds (n = 4), and thigh wounds (n = 2). Ten reintervention procedures for VSSI were performed and seven VSSIs settled on antibiotics alone. Five organisms responsible for the infection were isolated; MRSA was the most common (n = 2). Q-TWiST for patients with VSSI was significantly reduced compared with those who did not develop VSSI (6.34 vs 15.89, p < .001).
18:58 DISCUSSION
SESSION X: The SFA: Have We Found the Optimal Therapy?
Venue: Main Hall
Moderators: Ali Amin, Bauer Sumpio
John E. Connolly
University of California, Irvine, Orange, California
Carrel in 1905 first perfected vascular anastomosis by a triangulation technique. In other experiments, he anastomosed veins to arteries, showing that the vein wall thickened to safely compensate for the higher arterial pressure without any subsequent aneurysmal development. Likewise, he used vein patch grafts to enlarge the inside diameter of veins. However, surprisingly, these techniques were not clinically applied in patients until 40 years later, when Kunlin in France in 1948 reported the use of a reversed saphenous vein in a patient to bypass an occluded superficial femoral artery (SFA). Kunlin was a pupil of Leriche who had been very skeptical of its chances for success. Kunlin wrote, “After the patron's refusal, I elaborated the technique of grafting, choosing a lateral anastomosis for reasons of security and ease. No one knew the chances of success of a long graft. It was necessary to eliminate the difficulties and risks of anastomosing vessels of a size and quality that were often very different. Six months after proposing it to the patrons, I performed (in his absence) my first femoral-popliteal graft on a patient suffering increasingly from a necrotic ulcer of the foot in spite of sympathectomy and arteriectomy. The result surprised M. Leriche very much, as did the spectacular improvements from subsequent grafts.” Although open thromboendarterectomy of the common femoral artery was first performed by Dos Santos in 1946, it was not widely practiced until Wylie reported successful aortoiliac endarterectomy in 1951. He, along with Cannon and Barker, and subsequently Vollmar, next described semiclosed atherectomy of the SFA employing ring strippers. A transverse incision was made in the popliteal artery just distal to the occluding disease. The plane between the intimal disease and the media was developed, and a cutting ring stripper of the appropriate diameter was passed proximately until it passed beyond the occluding intimal disease. At this point, another transverse incision in the SFA was made and the core of obstructing disease was removed. Any residual flap in the popliteal incision was tacked down with interrupted sutures. Although these early ring debulking procedures results were promising, the technique was eventually abandoned because of the high incidence of subsequent artery occlusion due to residual disease and neointimal hyperplasia. In 1960, Edwards modified the operation by using a longitudinal incision the full length of the diseased artery followed by open endarterectomy. To avoid narrowing of the artery, he employed a long saphenous vein onlay patch. However, this was a tedious, long procedure subject also to occlusion and thus not widely adopted. In 1962, Linton and Darling reported their application of Kunlin's femoropopliteal bypass, and by 1971, DeWeese and Rob published excellent patency of the procedure at 5-year follow-up, establishing it as the gold standard for treatment of superficial femoral occlusive disease.
Mohan Adiseshiah
University College Hospital, London, United Kingdom
Wael Tawfick, Sherif Sultan
Western Vascular Institute, Galway, Ireland
John E. Connolly
University of California, Irvine, Orange, California
The fact that the profunda femoris artery may maintain the leg by collateral circulation in the presence of an occluded superficial femoral artery was described as long ago as 1811 by Sir Astley Cooper, a student of John Hunter and an eminent surgeon at Guys Hospital in London. Three decades ago Morris in London and Leeds and Gilfilian in San Francisco suggested that profundaplasty could be a simple alternative to femoral-popliteal bypass. Now, in the age of endovascular surgery, current trainees know little of open surgery and open profundaplasty. Besides cardiologists and endovascular radiologists concentrate their procedures on the superficial femoral artery. What little experience with angioplasty and/or stenting of the profunda femoris artery has been reported is lacking in follow-up.
The author's experience with open endarterectomy of the diseased profunda femoris artery and patch grafting using eversion endarterectomized tissue from the occlusived superficial femoral artery, has spanned 50 years. The major indications for the procedure has been: 1) to provide an adequate runoff vessel for a proximal bypass in the presence of an occluded superficial femoral artery; 2) as an alternative to a femoral-popliteal bypass. Oblique or lateral arteriographic views of the profunda femoris artery are necessary to select the patients who are judged to be candidates for the procedure. Disease is usually located at the origin or in the proximal portion of the artery, though may extend several inches downward. A major advantage of the procedure is that it only requires a small groin incision and can be performed under local anesthesia, making it applicable in poor-risk patients. If it fails to reduce claudication or rest pain, it can still be followed by a femoral-popliteal bypass.
Sam Ahn
University Vascular Associates and DFW Vascular Group, Los Angeles, California and Dallas, Texas
Peter Schneider
Hawaii Permanente Medical Group, Honolulu, Hawaii
SFA reconstruction is being undertaken more aggressively with endovascular means. Numerous options are available to the clinician to accomplish this, and it is often not clear which is best. Balloon angioplasty, stenting, scoring, cutting, cryoplasty, laser atherectomy, directional or rotational atherectomy, and stent grafts have been employed. Balloon angioplasty alone works well for focal stenotic lesions. Cutting balloon also works well here and may have a lower incidence of dissection. There is now level 1 evidence to suggest that primary stenting has better patency than selective stenting. However, many clinicians resist primary stenting because the treatments for instent restenosis are poor. Debulking devices provide an opportunity as a potential advance, but they have the risk of creating too much injury at the lesion site and releasing embolic material. Stent grafts seem to provide an improvement in patency rates, but they also cover collaterals and sometimes present with worse ischemia when they fail. A direct comparison of the rates of patency and complication is not possible based on existing data. The combination of available data and clinical experience is used to select treatments on a case-by-case basis.
Frank Criado
Union Memorial Hospital-MedStar, Baltimore, Maryland
Balloon angioplasty and stenting are well-established and widely available endovascular techniques. Their application to SFA intervention has resulted in expanded capabilities for lower extremity revascularization, but results continue to disappoint in some cases because of long-term failure related to hyperplastic restenosis and other issues. A host of alternative and additional endovascular technologies have emerged over the past years and continue to proliferate as an effort to improve on such results or replace the time-honored PTA/stenting techniques.
Currently available nitinol stents are easy to use, widely available, and highly predictable in their performance. Most interventionists have grown to depend on them, and that is the reason why they continue to predominate in the SFA field (and elsewhere). This is not likely to change any time soon—a thought reinforced by the lack of evidence so far that anything else is any better.
Sherif Sultan, Niamh Hynes
Western Vascular Institute, Galway, Ireland
Patients with CLI face a gloomy future, with 30% mortality in the first year and long-term survival significantly reduced compared with a matched population. Infrapopliteal bypass surgery (BS) is a demanding procedure with poor long-term survival. A minimally invasive therapy with equivalent consequences possibly be the unorthodox. Subintimal angioplasty (SIA) is easy to execute, requires short hospital admission, and has lower costs.
Our primary aim is to equate the effectiveness of SIA with BS in sustaining clinical improvement and amputation-free survival (AFS). Secondary end points are binary restenosis rate, freedom from target lesion revascularization (TLR), risk of major adverse clinical events (MACEs), quality time without symptoms of disease or toxicity of treatment (Q-TWiST), and cost-effectiveness.
From 2002 to 2007, 1,076 patients were referred with PVD. We prospectively compared 334 primary procedures (SIA = 206, BS = 128) in 309 patients (NSIA = 190, NBS = 119) with TASC C and D lesions. Mean age (SIA 73 ± 13 years vs BS 70 ± 14 years, p = .127) and comorbidity severity scores (p > .05) were similar between groups. Fifty-five percent were females in the SIA group versus 35% in BS, p = .0005.
Sustained clinical improvement at 5 years was 82.8% for SIA and 68.2% for BS (68.2%, p = 0.106, h = 0.65, 95% CI = 0.38–1.11).
Five-year freedom from binary restenosis was SIA 72.8% versus BS 65.3%, p = .7001, wheraes 5-year freedom from TLR was SIA 85.9% versus BS 72.1%, p = .2624.
Five-year all-cause survival was similar for SIA (78.6%) and BS (80.1%), p = .7343. Five-year AFS was comparable (SIA 72.9% vs BS 71.2%, p = .9765). Hyperfibrinogenemia and elevated CRP had a negative effect on AFS (p = .009, RR 2.4, 95% CI = 1.2–4.6 and p = .019, RR 1.02, 95% CI = 1.01–1.04, respectively).
Hyperhomocysteine had a significant adverse effect on the risk of binary restenosis for SIA (p = .009), BS (p = .019), and AFS for SIA (p = .009) and BS (p = .019).
Bypass results were not impinged on by stent use (35%, p = .780) or mean number of stents used (1.3, p = .330).
Risk of MAE (p > .002) and length of hospital stay (LOS-SIA 14 ± 16 days vs LOSBS 24 ± 23 days, p > .0001) were significantly reduced with SIA. Q-TWiST significantly improved (p > .001), and cost per QALY (SIA €5,663 vs BS €9,172, p > .05) reduced with SIA. Five-year risk of reintervention (p < .05) and mean number of procedures (SIA 1.19 vs BS 1.10, p = .078) were similar.
BS is an independent risk factor for MAE. Five-year freedom from MACE in SIA is enhanced by 20%. SIA enhances patient-specific Q-TWiST with substantial cost reduction. SIA expands AFS and symptom-free survival, is minimally invasive, and allows for a high patient turnover without compromising limb salvage. SIA seems to be virtuous and factual and a paradigm shift in the management of CLI.
Venkatesh Ramaiah
Arizona Heart Institute, Phoenix, Arizona
Alt Amin
Reading Hospital and Medical Center, Reading, Pennsylvania
Percutaneous intentional extraluminal recanalization (PIER) was first described by Bolia in 1989. Subintimal recanalization can be used to treat lesions that are typically difficult to treat with intraluminal percutaneous transluminal angioplasty, including long chronic occlusions, diffuse tandem occlusions, and calcified occlusions. Major contraindications are fresh thrombus, recent occlusions, and thrombosed aneurysm. If wire passes easily into the occlusion or there is evidence of acute/subacute occlusion, then use of the thrombolytics will help unmask the underlying stenosis or lesion. Utilizing the PIER technique to treat limb ischemia may be comparable to those treated with surgical arterial bypass especially if stents are used to improve patency.
Preprocedure Evaluation
It is essential to perform a complete evaluation of inflow and outflow arteries of the affected extremity. This should include aortoiliac anatomy to help with a possible contralateral approach. This evaluation can be performed utilizing arteriogram, CTA, or MRA. The approximate “start” and “end” points, length of occlusion, and diameter of the artery are taken into consideration. All patients are started on 81 mg of aspirin and 75 mg of Plavix a few days before the procedure. There is no contraindication in patients with renal insufficiency who need endovascular intervention since gadolinium or diluted contrast agent (quarter-strength Visipaque) can be used during intervention.
Contralateral Approach for Crossing Total Occlusion Superficial Femoral Artery
Place a 6F 55 cm contralateral sheath. Place the tip at the CFA. Perform a selective arteriogram to study the entire symptomatic lower extremity (baseline). Identity your “start” and “end” points of the occlusion. Place the image intensifier to cover the “start” and “end” points. If the occlusion is too long, then place the “start” point at the top of the image intensifier. Perform a roadmap through the sheath to visualize your “start” point and your “end” point (if possible). Advance a 100 or 120 cm angle 4F Tempo-Aqua (Cordis Endovascular) over an Exchange length angle glidewire 0.035 (280 cm). Place the tip of the Tempo-Aqua at the “start” point (where SFA patency ends and occlusion starts). Push (force) the angle glidewire into the occlusion. The wire may stay semistraight or form a loop. For long segment occlusions, form a loop by passing the wire back and forth until a loop is formed. Once a loop is formed, pass the Tempo-Aqua into the occlusion. Advance the wire more followed by the Tempo-Aqua until the “end” point is reached. For short segment occlusion (2–5 cm), slowly pass the wire without forming a loop and then advance the Tempo-Aqua. Continue to do this maneuver of advancing the Tempo-Aqua over the glidewire until the “end” point is reached. At this point, the “end” point and the patent distal SFA should be visualized on your roadmap. If not, then move the image intensifier down to cover this area and perform a new roadmap through the 6F sheath. Then pass the loop approximately 1 to 2 cm into the patent distal SFA. At this point, the tip of the loop usually enters the true lumen. Gently pass the Tempo-Aqua through the “end” point into the native SFA. Remove the wire. Backbleeding from the Tempo-Aqua is a good sign that you are in the true lumen of the patent SFA. Gently hand-inject half-strength dye to confirm this. Once this has been accomplished, the wire is exchanged for a stiffer 0.035 wire and a predilatation is done with a 4 mm diameter Opta balloon (Cordis Endovascular) with (appropriate length), followed by 7 or 8 mm diameter SMART stent (Cordis Endovascular) to cover the entire lesion. Post-stent angioplasty is usually done with a 5 or 6 mm diameter balloon. If the true lumen is not entered, then during hand injection, a channel might be seen leading to the native patent SFA (true lumen). In this case, roadmapping through the Tempo-Aqua is done and the glidewire is gently manipulated into the true lumen. Otherwise, the angle Tempo-Aqua is slightly pulled back and rotated to push the wire into the true lumen in a different direction. This should be done under roadmapping (done through the sheath) with image intensifier magnified. Rotating the tip of the angle Tempo-Aqua allows entering the true lumen through an alternative subinitimal channel. All efforts should be done to advance the wire into the true lumen at the “end” point using this technique. Advancing the loop wire further causes extension of the dissection plane into the native SFA, jeopardizing major collateral or future shorter bypass.
Bauer Sumpio, J.E. Aruny, P. Blume
Yale-New Haven Hospital, Connecticut
Alt Amin
Reading Hospital and Medical Center, Reading, Pennsylvania
Acute limb ischemia is defined as sudden reduction of the perfusion of an extremity that produces symptoms ranging from a worsening of preexisting symptoms to a dramatic threat to limb viability. The age of the affected individuals is usually older than 70 years, and patients usually have multiple comorbid medical conditions. Beyond the risk of limb loss, acute arterial occlusion is associated with high mortality (up to 20%) in patients even with revascularization. Etiologies of acute limb ischemia include thrombosis or embolism. Thrombosis may include either the native artery or a bypass graft. Thrombosis of a native artery most commonly occurs when there is preexisting arterial occlusive disease. Thrombosis of an arterial bypass graft is usually secondary to progressive atherosclerosis in the proximal or distal native artery or possible pathology in the graft itself. Prosthetic bypass grafts may develop intimal hyperplasia in either distal or proximal anastomosis. Autogenous bypass grafts may develop intimal hyperplasia or stenosis at the site of venous valves, which may lead to flow-limiting lesion.
The goal of treatment of acute limb ischemia is to achieve a viable, functional, pain-free in a patient. Urgency of treatment depends on the degree of ischemia. With the exception of an embolus where an embolectomy can quickly restore normal arterial flow, thrombosis of a native artery is associated with a complex occlusion, which includes underlying atherosclerosis.
Pharmacologic thrombolysis alone to restore arterial flow in an extremity may require a long period of administration with increased risk of bleeding. Mechanical thrombectomy allows removal of an acutely occluded artery, with a high thrombus burden, in a percutaneous fashion.
Combination of a mechanical thrombectomy catheter and a thrombolytic agent is even more powerful in restoring arterial circulation in an acutely ischemic leg. This method has several advantages when compared with either technique alone. They include faster result with restoring perfusion, limiting the dose of thrombolytic, minimizing risk of bleeding, and restoring perfusion to the occluded collateral vessels. This technique, while maximizing limb salvage, minimizes risk of wound infection and cardiac complications associated with open procedures.
Tubassam Muhammad, Sherif Sultan
Western Vascular Institute, Galway, Ireland
Chris Beirne, Sherif Sultan
Western Vascular Institute, Galway, Ireland
EvR allows for high patient turnover with procedural and clinical outcome success without compromising hemodynamic outcome.
09:00 DISCUSSION
SESSION XI: Tibial Artery Disease: How Far Can You Go?
Venue: Main Hall
Moderators: Herbert Dardik, Cliff Shearman
Herbert Dardik
Englewood Hospital & Medical Center, Englewood, New Jersey
We have previously described the basis for using the distal arteriovenous fistula (dAVF) as an adjunct to crural revascularization. Even in the era of endovascular surgery, we believe that tibial/peroneal bypass combined with dAVF will continue in the surgical armamentarium required for limb salvage, when a prosthetic is required. Our data, similar to those of other institutions, show a significant decline in open lower limb bypass, although the total number of peripheral vascular procedures has increased.
The theoretical basis for using the dAVF as an adjunct to crural reconstructions is based on the need to reduce the vascular overload presented to the distal circuit and, at the same time, keep graft flow above the critical thrombotic threshold level. This results in increased flow in the graft and with distal perfusion, reversal of the ischemic state. Maldistribution can occur if inflow is restricted, as is possible with poor compliance of the inflow conduit graft material causing a relative stenosis effect. However, the concept of “steal” does not exist in these cases of advanced ischemia since antegrade flow distal to the distal anastomosis has been confirmed by electromagnetic flow, duplex studies, and, most important, by clinical reversal of the ischemic state.
Over a 30-year period, cumulative patency rates were documented for 488 reconstructions and compared in subgroups as a retroprospective historical analysis and not as a prospective randomized study. The subgroups were based on improved patient selection and surgical technique over time. The majority of the operations were performed with glutaraldehyde-processed umbilical vein grafts. Primary and secondary cumulative patency rates for the most recent subgroup at 3 years were 50% and 55% and at 5 years 36% and 40%. Corresponding limb salvage and patient survival rates were 65% and 58% at 3 years and 44% and 42% at 5 years. Conversely, our experience with dAVF in the inframalleolar position has been unimpressive. Only one of six cases continues patent after 2 years.
Despite the negativism expressed by some authors with regard to the need for adjunctive procedures to enhance crural graft patency, we continue to be impressed by reasonably durable patency and limb salvage rates. We believe that the creation of a dAVF as an adjunct to prosthetic bypass at the crural level has validity and the potential for significantly improving crural limb salvage rates and return the patients to a functional and pain-free existence.
Peter Schneider
Hawaii Permanente Medical Group, Honolulu, Hawaii
Endovascular reconstruction of the tibial arteries is assuming a larger role in limb salvage. Devices and techniques have improved significantly, and this has led to increased aggressiveness in the endovascular treatment of these arteries. Disease in the tibial arteries tends to be diffuse and is usually a combination of long segment stenoses or occlusions. The small caliber of the arteries, the remote location, the slow flow of the distal bed, and concerns about preserving runoff capacity have combined to make this a vascular bed that presents challenges to endovascular treatment. The results of tibial angioplasty and stenting are closely tied to the degree of foot damage with which the patient presents. When foot damage is in an early stage, a small improvement in perfusion may be enough to heal the lesion, even if patency is only short term. The best results are achieved when presenting ischemic foot damage is minimal; risks of intervention are low, the likelihood of damaging the runoff is low, and a leg bypass is often avoided. When there is objective evidence of ischemia and an open ischemic lesion that has caused minimal damage, endovascular is the treatment of choice, rather than waiting to see if the patient needs a distal bypass. Unfortunately, many patients present with severe foot damage, often with ongoing or partially treated infection. When foot damage is extensive, recanalizing one tibial artery is often not adequate for limb salvage. Open as many tibial arteries as possible to provide robust revascularization to a severely damaged foot. If the only thing open distally is an isolated segment that does not provide in-line flow to the foot, do not waste your time with endovascular. Tibial angioplasty and stenting is assuming a larger role as devices and techniques have improved.
Alt Amin
Reading Hospital and Medical Center, Reading, Pennsylvania
Sherif Sultan, Wael Tawfick, Niamh Hynes
Western Vascular Institute, Galway, Ireland
Prospective clinical prelude showed ostial lesions with poor distal runoff to have reduced the prospect of distal embolization and ameliorated PTA if CELA is used primarily in instances where the wire can cross but not the balloon. Initially, compromised endeavors at crural PTA can be treated successfully with redo PTA without spoiling subsequent attempts at bypass grafting.
Peter Schneider
Hawaii Permanente Medical Group, Honolulu, Hawaii
Complex lower extremity lesions are being managed with increasing frequency using endovascular techniques. As this trend has developed, the potential for limb-threatening distal embolization to occur during these procedures is increased. Distal protection devices may have utility in complex lower extremity revascularizations. Although it is not yet clear which cases may be best for this technique, there are some clues. Distal protection devices have been used with success while treating the following conditions, including embolizing infrainguinal lesions, during debulking of femoropopliteal lesions with atherectomy devices (laser or mechanical), complex lesions containing thrombus, friable or mobile lesions, severe femoropopliteal occlusive disease with single-vessel runoff, treating recent emboli (eg, during mechanical thrombectomy). Use of distal protection devices in routine lower extremity endovascular cases is not warranted. This technique is contraindicated when there is no safe landing zone for the filter, when the filter cannot be placed, when the arteries are too large for available filters, and when the filter guidewire length is inadequate for performing the case. Distal protection devices are currently being used in approximately 20% of lower extremity revascularizations in our institution. Aspiration is used liberally. Debris was recovered in 80% of cases. Cessation of flow during the procedure occurs in about 20%. It is beneficial to have a clear understanding of the runoff before placing the filter. This is especially true if the case has already been identified as one in which the runoff is at risk. Among patients with lesions at high risk for embolization or with compromised runoff, the use of a distal protection device should be considered during infrainguinal endovascular repair.
Frank Veith
The Cleveland Clinic, Cleveland, Ohio, and New York, New York
The RESILIENT Trial was a prospective randomized trial comparing two strategies of revascularization for superficial femoral artery stenosis and occlusions. The trial compared percutaneous transluminal angioplasty (PTA) versus angioplasty and stenting from both an acute and 12-month outcome point of view. Initial evaluation demonstrated statistically significant benefit for use of self-expanding nitinol LifeStent compared with angioplasty alone, and this benefit seemed to continue through to the 1-year time period. At 1 year, primary patency in the stented group was 80% versus 38% in the PTA group (p < .0001), and freedom from target lesion revascularization was 87% in the stented group and 48% in the PTA group. At 2 years, freedom from target lesion revascularization was 80% in the stented group and 43% in the PTA group (p < .0001).
Thus, level 1 data continue to support the use of stenting in most superficial femoral artery lesions, whereas angioplasty may be effective in certain lesions, particularly those that are shorter in length.
The presence of extensive calcification and longer lesion lengths provide strong predictive value for benefit in use of the LifeStent.
Cliff Shearman
Univerity of Southampton, Southampton General Hospital, Southamptom, United Kingdom
By 2010, there will be 221 million people with diabetes worldwide, and in the United Kingdom, the latest QoF data have shown a prevalence of 3.55%. A large number of complications are associated with the disease process, in particular the risk of developing a foot ulcer. An estimated 5% of patients with diabetes develop a foot ulcer every year, and a lifetime risk of an ulcer is 15%. The ultimate consequence of foot disease without adequate management is amputation. The relative risk of amputation associated with diabetes is 13 times greater compared with that of a nondiabetic patient.
In the current REACH Registry, a current view of the outcomes for patients with peripheral arterial disease (PAD), 43% of patients have diabetes, and the prevalence is increasing. Therefore, the majority of patients with PAD will either have diabetes or present with foot complications as a direct consequence of the disease.
Insulin resistance is strongly linked to the development and progression of PAD, and patients with type 2 diabetes have 3 to 5 times greater chance of developing PAD compared with nondiabetics. Intensive blood glucose control does not appear to reduce the risk of developing cardiovascular death or prevent amputation. However, development of the complications of diabetes is strongly associated with previous episodes of hyperglycemia, as reflected by HbA1C levels. A reduction of 1% in HbA1C is associated with a 21% reduction in complications. Risk factors for PAD such as hypertension, smoking and hypercholesterolemia are extremely common in type 2 diabetics. Not only does their presence increase the risk of an individual developing PAD, but in the patient with diabetes, the individual risk is amplified by the diabetes. Conversely, however, the benefits of risk factor modification, blood pressure control, lipid lowering with statins, and smoking cessation are greater for the patient with diabetes compared with the nondiabetic patient. Many patients with complications of diabetes and PAD have poor diabetic control, which is often overlooked by the podiatrist or vascular surgeon treating the specific foot complication. This emphasizes the need for a well-coordinated multidisciplinary team.
At a microscopic level, there are differences between diabetic and nondiabetic vascular disease. Histologic examination of atherosclerosis from diabetics reveals more calcification and increased presence of inflammatory cells, which are generally held to be bad prognostic signs. At a macrovascular level, it is commonly recognized that the disease more commonly affects the more distal parts of the circulation, particularly the calf, with relative sparing of the pedal blood vessels. The microcirculation itself is often abnormal, with changes in vasomotor control, thickening of the vascular endothelium, and abnormalities of the platelets, which may partly explain the sudden deterioration seen in wounds that initially appear to be healing well. The effect of this microcirculatory dysfunction tends to amplify the effects of large vessel disease.
The biologic behavior of vascular disease in diabetics also seems different. Patients with coronary artery disease and diabetes have a worse prognosis than nondiabetic patients despite equivalent treatment. In the coronary circulation, collateral development is less marked in diabetic patients, which may influence their ability to adapt to vascular disease. Patients with diabetes are at considerably greater risk of lower limb amputation than nondiabetic patients, and the detection of PAD is a strong predictor of the subsequent amputation.
There is increasing evidence that diabetic vascular disease behaves differently from nondiabetic vascular disease. The disease affects more peripheral vessels, and the lesions tend to be more calcified. There is increased inflammatory activity, and the lesions progress more rapidly, with plaque rupture more likely. Also, patients with diabetes seem less likely to form collaterals after acute events. Clinically, although some present with signs of chromic ischemia, many will develop foot complications, which unmask the PAD and need urgent treatment.
On balance, then, it seems that diabetic vascular disease is a different condition from nondiabetic disease and should be managed as such.
Chris Beirne, Sherif Sultan
Western Vascular Institute, Galway, Ireland
09:57 DISCUSSION
10:00 COFFEE BREAK
Venue: Exhibition Hall
SESSION XII: Carotid Artery Disease: Is CAS Safe for Routine Practice?
Venue: Main Hall
Moderators: Frank Criado, Ross Naylor
Frank Criado
Union Memorial Hospital-MedStar, Baltimore, Maryland
Gaining endovascular access for the introduction and delivery of stent graft devices remains the most important technical issue during TEVAR. Not infrequently, patients present with small or diseased access arteries that make them unsuitable for the standard (and desirable) transfemoral approach.
Although a retroperitoneal common iliac artery conduit is the most common alternative technique, it cannot always be used. Other retrograde (transiliac and transaortic) technical options exist, as well as antegrade alternatives such as use of the common carotid artery. These and other techniques will be discussed and examined during the presentation.
Ross Naylor
Leicester Royal Infirmary, Leicester, United Kingdom
Positive cultures were obtained in 54 of 73 (74%), with staphylococci/streptococci accounting for 90% of infections. Only 7 MRSA patch infections have been reported.
A variety of management strategies were described: (1) conservative (n = 5, 2 late reinfections), (2) endovascular (n = 3, 0% early morbidity, no reinfections at 12 months), (3) carotid ligation (n = 7, 17% 30-day death/stroke, no reinfections), (4) patch excision plus autologous reconstruction (n = 43; 9.3% 30-day death/stroke, 8% reinfection), and (5) patch excision plus prosthetic reconstruction (n = 9, 11% 30-day death/stroke, all survivors reinfected).
Peter Naughton, Mark Eskandari, Mark Morasch, J.S. Matsumura, H.R. Rodriguez, W.H. Pearce
Division of Vascular Surgery, Northwestern University, Chicago, Illinois
Northwestern Memorial Hospital, Chicago, Illinois
Droc lonely Goleanu Viorel, Pinte Fiorina
Army's Center for Cardio-Vascular Diseases, Bucharest, Romania
Few data are available on surgical or endovascular treatment of failed carotid stenting. The aim of this study is to document the incidence, location, risk factors, and clinical consequences of restenosis after carotid artery stenting (CAS).
The rate restenosis has been reported in different series between 2 and 8%.
Restenosis is defined as a stenosis more than 80% in duplex scan. It can be located proximal to the body of the stent, central to the body of the stent, and distal. It is symptomatic in only 7% of cases. Instent restenosis (ISR) may be managed by endovascular techniques; however, the results obtained may be suboptimal, particularly in the long term. The surgical approach is also difficult because of the fibrosis of the surrounding tissues, the requirement for distal internal carotid artery dissection, and clamping and removal of the stent.
The endovascular procedures that can be used are balloon angioplasty alone, angioplasty and stent, and angioplasty with cutting balloon. Some teams reported very good results without per procedural complications and absence of significant restenosis at 1 year.
More aggressive approaches are currently at the investigational level and include intravascular brachytherapy, antiproliferative therapy with drug-coated stents, and biodegradable stents.
The factors identified with the developing of ISR are female gender, elevated creatinine level, and elevated cholesterol level. The surgical treatment is carotid endarterectomy (CEA) with plaque and stent removal. An alternative to CEA is the arterial bypass using saphenous vein graft or PTFE grafts.
In our experience, ISR appears in 5% of cases. In the primary procedure, we have used autoexpandable stents and cerebral protection devices systematically.
We performed CEA with en bloc removal of the plaque and stent, using a Brenner shunt for cerebral protection and Dacron patch of enlargement. Intimal hyperplasia was the predominant mechanism leading to ISR. No major complications occurred. The postoperative follow-up (by duplex scan) was 12 months. The patients remained asymptomatic and without recurrent restenosis.
In conclusion, the optimal treatment of instent restenosis has yet to be defined, but standard CEA with stent removal appears to be feasible and safe for the patient.
Ross Naylor
Leicester Royal Infirmary, Leicester, United Kingdom
It is essential that the phrase being “high risk for carotid endarterectomy (CEA)” does not become synonymous with being “high risk for stroke.” They are not the same. Recognized features for making CEA more risky include multiple medical comorbidities, increasing age, and anatomic/surgical features such as contralateral occlusion, restenosis, radiation arteritis, and recurrent laryngeal nerve injury. However, unless these are also associated with an increase in stroke risk, accepted guidelines of practice must be maintained (ie, procedural risk must still be < 6% in symptomatic patients and < 3% in asymptomatic patients).
In recently symptomatic patients, several of the features that make surgery more difficult were associated with the greatest benefit from surgical intervention in ECST and NASCET (eg, increasing comorbidity, very recent symptoms (< 2 weeks), age > 75 years, contralateral occlusion, increasing stenosis, irregular plaques). It may, therefore, be reasonable to accept a slight relaxation of accepted risk thresholds in these patients.
By contrast, asymptomatic patients are completely different, and none of the high risk for stroke criteria found in symptomatic patients held true in ACAS and ACST (eg, patients aged > 75 gained no benefit at all from intervention even if the procedural risk was excluded). Neither trial showed that women (overall) gained any benefit from intervention. I also defy anyone to prove that an asymptomatic restenosis confers a higher risk of late stroke than an atherosclerotic lesion.
In essence, being “high risk” should refer to the risk of stroke, and it means (first and foremost) being symptomatic, especially if the index event occurred within the preceding 7 days. By contrast, we have virtually no consensus criteria for what constitutes a “high risk for stroke” asymptomatic patient. This definition should not, however, include women, restenoses, or patients aged > 75 years!
Piergiorgio Cao, Paola De Rango, Deborah Brambilla, Giuseppe Giordano, Gianbattista Parlani, Fabio Verzini
University of Perugia, Ospedale S. Maria della Misericordia, Perugia, Italy
Sherif Sultan, Niamh Hynes
Western Vascular Institute, Galway, Ireland
CEA is the gold standard in stroke preclusion. Although CAS showed initial promise in high-risk patients, recent trials have cast doubt on safety and efficacy. Our aim is to conciliate CAS with CEA and BMT in high-risk patients regarding clinical success, efficacy in plummeting morbidity and mortality, and recuperating cost-effectiveness. Primary end points were stroke, myocardial infarction, or death. Secondary end points were patency rate, cost-effectiveness, length of hospital stay, and reintervention rate.
From 2002 to 2007, 712 patients with carotid artery disease were managed; 300 were high risk and symptomatic with low GSM on preoperative duplex ultrasound. Patients were assigned to CEA (n = 228), CAS (n = 34), or BMT (n = 38). Nineteen (6.3%) had bilateral interventions. Propensity scores were used to adjust for confounding factors.
Mean age was similar between CEA, 68.6 years, and CAS, 70.6, p > .05, but BMT patients were significantly older (75 years) than CEA (p < .01) or CAST (p < .05) groups. Male-to-female ratios were 2:1 for CEA and CAS and 1:1 for BMT. Comorbidity severity scores were similar between groups (p > .05). Mean length of hospital stay was similar between CEA (9.4 ± 0.5 days) and CAS (7.2 ± 1.1 days), p = .130. However, mean time in HDU was reduced with CEA (1.9 ± 0.3 days vs 0.2 ± 0.1 days, p = .025).
Following carotid intervention, the overall 30-day stroke-free survival rate was 99.1% (95% CI 99.6–99.9), and at 5 years, the stroke-free rate was 99.1% (95% CI 99.6–99.9), stroke-free survival was 90.6% (95% CI 85.9–93.9), and primary patency was 94.6% (95% CI 90.5–97.0). At 5 years, stroke-free survival was significantly improved with CEA (90.6%) when compared with BMT (44.3%, p < .0001, h = 0.22, 95% CI 0.08–0.61) but was not significantly improved with CEA (90.6%) when compared with CAS (84.3%, p = .581, h = 0.73, 95% CI 0.22–2.44). Four patients in the CAS group required on-table tPA. Three of these recovered fully by the end of the procedure, and the fourth, an 84-year-old lady, had a postoperative hyperperfusion reaction and required overnight care in the HDU.
Cox proportional hazards ratio showed that age > 80 years (p < .001), female gender (p < .04), and echolucent plaque material (p < .01) were associated with reduced stroke-free survival. Quality of life, Q-TWiST, and cost per QALY were similar between CEA and CAS (p > .05) but were significantly improved with CEA compared with BMT (p < .0001 and p < .001).
OMT does not prevent future stroke in patients with severe carotid artery disease. Indications for CAST are limited and strict selection criteria should apply. Contemporary Trends in Carotid Intervention had verified that Carotid Artery Stenting prerequisite a lot of development with device maturity sooner than it is befall routine clinical practice. CEA is the gold standard in management of carotid artery disease with superior stroke free survival rates at five years when compared to CAST or OMT.
Anthony Comerota
Jobst Vascular Center, Toledo, Ohio
The SAPPHIRE trial was designed as a randomized trial to compare carotid artery stenting (CAS) with carotid endarterectomy (CEA) in patients at high risk for CEA. However, the majority of the patients reported in SAPPHIRE were part of the “SAPPHIRE Registry” and, hence, not randomized. The patients who were deemed unacceptable for CEA were assigned to CAS. Unfortunately, this was “opinion-based” entry criteria, not objectively driven criteria, and therefore was not testable. The study was originally designed to randomize up to 2,900 patients but was terminated after randomizing only 334 patients (less than one-eighth of the projected upper limit), the majority of the patients being asymptomatic and a large cohort having recurrent carotid stenosis. The SAPPHIRE trial was flawed from inception because it was based on an improperly designed “feasibility study.” The treatment outcomes of patients in SAPPHIRE were compared with those of NASCET and ACAS. However, arteriographic criteria were used for patient entry into ACAS and NASCET, but this was not the case with SAPPHIRE. Patients were entered on the basis of noninvasive testing, which substantially overestimated the disease. However, arteriogram information was available and reported to the FDA (but not in their manuscript). Less than 2% of SAPPHIRE patients had ≥ 90% ICA stenosis, and < 20% of SAPPHIRE patients had ≥ 80% diameter reduction of stenosis. Although the SAPPHIRE patients were at high risk for procedures, the majority of the patients did not have high-risk carotid disease. The results of the CREST trial will undoubtedly clarify many of the remaining issues surrounding CAS versus CEA.
Jean Pierre Becquemin
University of Paris XII, Henri Mondor Hospital, Creteil, France
Carotid stenting (CAS) has been proposed as an alternative to surgery with the advantage of avoiding the complications of neck incision and of general anesthesia.
Unfortunately, for recently symptomatic carotid stenosis, accumulating data comparing CAS and CEA led to the perception that CAS is less efficient than CEA.
EVA 3 S was a multicenter randomized noninferiority trial comparing CAS with CEA in patients with a symptomatic carotid stenosis. Five hundred twenty-seven patients were enrolled; 263 were submitted to CAS and 264 to CEA. The majority of patients had a previous stroke or a hemispheric TIA, and 13% had ocular TIA. Seventy percent had a tight stenosis (> 80%) and 30% a less severe stenosis (between 60 and 79%). At 1 month, the RSD was 9.6% after CAS and 3.9% following CEA, with a relative risk of 2.5 of RSD with CAS. When considering disabling strokes and deaths, the rates were 3.4% with CAS and 1.5% with CEA (RR 2.2). There were more pulmonary complications and cranial nerve injuries following CEA and more local complications following CAS.
Recent analysis of the 4-year follow-up of EVA 3S was less pessimistic. Both groups had a similar long-term adverse event rate when the first month events were not taken into account. 1
The SPACE trial had a design similar to that of EVA 3 S. After 1,183 patients enrolled, the trial was stopped for futility reasons and lack of founding. It was calculated that with the current event rates, a sample size of more than 2,500 would be needed to achieve 80% power. The RSD was 6.84 with CAS and 6.34 with CEA. Disabling ipsilateral stroke was 4.01% with CAS and 2.91% with CEA.
The 2-year results have recently been published.2 The rate of recurrent ipsilateral ischemic strokes was similar for both treatment groups. The incidence of recurrent carotid stenosis at 2 years, as defined by ultrasound, was significantly higher after carotid artery stenting.
They are other clues against CAS in symptomatic patients.
McPhee and colleagues reviewed 259,080 carotid interventions performed in the United States between 2003 and 2004.3 They showed that the rates of stroke and death in symptomatic patients were, respectively, 4.2% and 7.5% with CAS and 1.1% and 1% with CEA (p < .0001).
Finally, in a systematic review and meta-analysis of 10 RCTs, Murad and colleagues concluded that CAS and CEA seem equivalent in terms of death and nonfatal myocardial infarction.4 Although the impact on stroke remains unestablished, results are consistent with a clinically important increase in stroke risk with stenting, an intervention that aims at reducing the risk of stroke.
These data represent a serious drawback for CAS in symptomatic patients. It remains, however, uncertain that they are the final nails in the coffin of CAS.
Similar long-term outcomes between the two treatment modalities are reassuring. Thus, a reduction of early complications with CAS may shift the current trend against CAS. Is it achievable? Good training and high caseload, 5–8 stent and protection device selection according to the patient's anatomy, 9–13 and, finally, rejection of adverse anatomy 14 may reduce the overall complication rate after CAS.
On the other hand, previous symptoms are constantly identified as a major predictor of adverse outcome after CAS. 15,16 Delayed treatment with CAS after stabilizing the plaque by statins and double-antiplatelet regimen is not an advisable option: it has been shown that urgent intervention is a major factor of stroke prevention.
In summary, according to the current data, we do think that for symptomatic carotid stenosis, CAS is a bridge too far. Remarkable results achieve by modern surgery cannot be beaten.
Alt Aburahma
Charleston Area Medical Center, Charleston, West Virginia
Mark Eskandari
Northwestern Memorial Hospital, Chicago, Illinois
Carlos Timaran
Dallas Veterans Affairs, Dallas, Texas
Craig Kent
University of Wisconsin Hospital, Madison, Wisconsin
Although the outcomes of carotid stenting and endarterectomy have been compared in various trials, the relative indications for these two interventions remain controversial. Despite uncertainty about carotid stenting, over the past several years in the United States, a large number of CAS procedures have been performed. The development of an ICD-9 procedural code for CAS in the United States has provided us with the opportunity to examine the outcomes of CAS and CEA performed by all practitioners in two large states. The data to be presented represent the largest direct comparison of these two techniques to date. Our findings are notable in that we will demonstrate that symptomatic patients do not benefit from CAS; conversely, asymptomatic patients may. One could hypothesize that the differences in outcomes found in symptomatic and asymptomatic patients are explainable based on anatomy. In symptomatic patients, internal manipulation of an unstable plaque may predispose to embolization and stroke, whereas internal manipulation of stable plaque in an asymptomatic patient may not.
In this analysis of 49,107 hospitalizations from New York and California for either CAS or CEA, we found CAS patients to have a significantly greater number of comorbidities, making direct comparison of these two cohorts impossible. Thus, the technique of propensity scoring was used to create cohorts matched by comorbid conditions and demographics. The choice of these two states for this analysis was based on the availability of a present on admission flag, allowing the distinction between pre- and postoperative neurologic symptoms. Although patients who underwent CAS had significantly more comorbidities, there were no statistical differences in comorbidities or demographics between the groups after propensity matching.
In the matched symptomatic cohort, the mortality rate was three times as high in patients treated with CAS when compared with those treated with CEA. Moreover, there was a 2% higher rate of stroke in patients treated with CAS, although this finding did not reach statistical significance. The combined stroke/mortality rates revealed an absolute difference of approximately 3.5% favoring CEA. Ironically, the only reimbursed indication for carotid stenting currently is for high-risk symptomatic patients. Yet a major European study and now our analysis of two large data sets from the United States reveal that symptomatic carotid stenosis may not be an appropriate indication for CAS. Our finding of a dramatic and significant increased risk of stroke and death in symptomatic patients undergoing CAS warrants reevaluation of the patient population that may indeed benefit from this intervention.
Conversely, in matched asymptomatic patients, there was no statistical advantage of either procedure, and the absolute difference for all primary outcomes was less than 0.5%. Furthermore, the mortality rates were essentially equivalent in the asymptomatic patients receiving stent or endarterectomy. When a minimally invasive intervention is compared with conventional surgery, if there is equivalence in outcomes, more often than not, the patient's choice is the less invasive procedure. Clearly, there are other relevant factors that impact the choice of a procedure, including the cost, the steepness of the learning curve for new technology, as well as the availability of skilled interventionalists capable of providing optimal outcomes. In this series, the asymptomatic population constituted approximately 91% of the treated patients. Thus, these findings are relevant to a large number of patients with carotid artery disease. In most reported series of patients treated for carotid disease, at least two-thirds of patients are asymptomatic. These findings raise the possibility that ongoing randomized controlled trials comparing CAS and CEA may well demonstrate benefit and safety of CAS in asymptomatic patients. Practitioners should feel confident in encouraging active enrolment of asymptomatic patients in current and future trials comparing these two interventions.
This analysis brings to question the current role of carotid stenting for the treatment of both asymptomatic and symptomatic carotid atherosclerosis. A rate of perioperative stroke and mortality of 8.06% for CAS versus 4.66% for CEA in symptomatic patients suggests that the current coverage criteria for CAS may be inappropriate. For asymptomatic patients, the near-equivalent rate of stroke and death of 2.60% for CAS versus 2.32% for CEA suggests that CAS may indeed be advantageous in this cohort of patients. Although we recommend that definitive decisions regarding the treatment of carotid stenosis await the results of randomized trials such as CREST, in the interim, consideration should be given to limiting the widespread policy of treating symptomatic patients with CAS. Moreover, randomization of asymptomatic patients in ongoing clinical trials should be encouraged.
Frank Criado
Union Memorial Hospital-MedStar, Baltimore, Maryland
FDA approval of carotid stenting (in the United States) appeared to signal the beginning of the end for CEA, but such fate has not materialized. Why?
Clearly, this is a complex area where many different reasons and developments have combined to explain the current status of CAS. In any case, it is a most interesting “case study” that we should all scrutinize and try to understand. Carotid revascularization is a most important area for vascular surgeons and all vascular specialists, and this is a dynamic field that will continue to evolve.
Despite its present woes, CAS is likely to have a bright future and to play a significant role in carotid revascularization. In the meantime, CEA continues to predominate and be the standard of the care for most patients; this is not likely to change any time soon.
Rodney White
Harbor-UCLA Medical Center, Los Angeles, California
Carotid endarterectomy for extracranial carotid artery occlusive disease has demonstrated efficacy. Multiple studies have shown that significant stroke risk can be minimized by appropriately choosing patients for intervention.
New modalities to treat carotid lesions, that is, carotid stents and medical therapy, are evolving, and clinical efficacy of these methods is complex as the new therapies continue to change and the indications for intervention, including asymptomatic patients, require long-term comparative studies that have not been completed.
Randomized studies comparing the efficacy of CEA, stents, and medical therapy may be initiated, but the likelihood of determining benefit across a broad spectrum of patients with evolving endovascular technologies and drug therapies is unlikely by randomized methods.
A promising way to determine efficacy in the evolving environment is to compare modalities in similar patients using clinical registries that have been carefully constructed to enable ongoing analysis of established methods in patients with clearly defined clinical syndromes and add additional treatment modalities as the intervention matures to the clinical trial phase.
The good news is that treatment is advancing. The responsibility of the interventional community is to introduce treatment based on comparative studies to established methods with patient care being protected from adaptation of unproven methods.
Peter Schneider
Hawaii Permanente Medical Group, Honolulu, Hawaii
Carotid stenting (CAS) will remain a treatment option. There is a group of patients who are at high risk for open surgery who will continue to use CAS as the only reasonable available treatment option, regardless of the outcome of ongoing trials. This includes patients with anatomic high risk, such as open tracheostomy, previous radical neck dissection, cranial nerve palsy, and certain recurrent carotid lesions. How widely CAS is used beyond surgical high-risk cases will depend on the results of ongoing studies and further developments. The long-term patency and stroke-free survival of carotid stenting appear to be similar to those of endarterectomy. The difference in success between the two treatments will likely come down to 30-day rates of adverse events. As experience has been gained with stenting, subsets of patients who are at higher risk for stenting have been identified. Patient selection and advances in equipment, technique, and clinical management are likely to lead to continued improvement in carotid stenting.
Carlos Timaran
Dallas Veterans Affairs, Dallas, Texas
Alt Aburahma
Charleston Area Medical Center, Charleston, West Virginia
Dieter Raithel, Lefeng Qu, Ritter Wolfgang
Medical Centre of Nuremberg, Nuremberg, Germany
Military Medical University, Shanghai, China
Nuremberg Southern Hospital, Nuremberg, Germany
Herein we present the first reported case of fracture of a cerebral protection device wire in carotid artery stenting for management of a restenosis lesion after carotid endarterectomy. ACCULINK carotid stent and RX ACCUNET embolie-protections system (Guidant, CA) were used. All procedures were carried out routinely and normally according to the guidelines. But the protection wire was broken while retrieving the protection system, and the tip of the protection system (basket part) was found inside the patient. Immediate angiogram showed migration of the carotid stent to the common carotid. This patient was converted to open surgery 19 days later, and the tip of the protection device was found biting together with the carotid stent; both were explanted, and a Dacron patchplasty was undertaken for the residual stenosis. No symptoms were detected during all the procedures.
Frank Criado
Union Memorial Hospital-MedStar, Baltimore, Maryland
Endovascular repair of nonbranched segments of the aorta is relatively straightforward and will be embraced as the new standard of care in the near future. Unfortunately, a predominance of aortic thoracic pathologies occurs adjacent to or in branched segments—most notably, the aortic arch and the visceral segment. Branch management has thus emerged as a frequent and most important issue in the entire TEVAR field.
In essence, branches can be sacrificed (overstented), revascularized, or relocated in the context of endograft intervention when branch vessel origin must be covered by the device during endovascular repair. Technical options abound for management of arch branches because these vessels are relatively easily accessible, either through the neck or via a median sternotomy. The situation is altogether different in the visceral segment, where debranching requires the performance of major intracavitary operations.
The various options and current state of the knowledge and thinking will be examined in some detail in the course of the presentation.
13:10 DISCUSSION
13:15 LUNCH
Venue: Restaurant
SESSION XIII: Vascular Innovation: From Stem Cells to Robots
Venue: Main Hall
Moderators: Alan Dardik, Alun Lumsden
Alan Dardik
Yale University School of Medicine
Well-publicized clinical trials that used growth factors for therapeutic angiogenesis led to disappointing results, with negative trials for FGF and VEGF injections in patients with claudication or in need of limb salvage but without other options. However, the exciting potential of stem cells to provide a more balanced, and perhaps optimal, cocktail of growth factors capable of both angiogenesis—small vessel growth—and arteriogenesis—large vessel growth—has reopened the field with additional possibilities for treatment and trials. Initial exciting reports and small series have been reported using both bone marrow—derived stem cells as well as peripherally circulating stem cells as sources of stem cells. Current clinical trials have yet to define the optimal cell sources, type, and purpose for in vitro culture, as well as the method of delivery of the cells to the patient. As additional advances will be made in the field, it is likely that stem cell treatments will become a useful option for the vascular surgeon to treat patients.
Dusan Pavcnik
Oregan Health & Science University of Portland, Portalnd, Oregon
Alan Dardik
Yale University School of Medicine
Dusan Pavcnik
Oregan Health & Science University of Portland, Portalnd, Oregon
Materials and Methods: This filter (Angiodynamics) was designed as jugular and femoral delivery via a single delivery system, 6F deployment catheter system, filtering efficiency, self-centering design, nonmigrating with stable fixation, and minimal wall damage on retrieval. In addition to anchoring and filtering struts, this filter has four centering struts that have the ability to disengage from the filtering core portion, thereby allowing the legs to slide out of endothelial growth. Six filters were placed in three sheep, two filters in each sheep. Filters were assessed for ease of delivery, filter tilt, filter migration, patency, success of retrieval, and filter fractures. Post—filter retrieval histopathology of the IVC was performed to asses for possible wall injury and foreign body response.
Triona Lolly
Dublin City University, Dublin, Ireland
Restenosis is the major long-term limitation of intravascular stenting procedures. Excessive proliferation of vascular smooth muscle cells (SMCs) is the predominant mechanism of neointima formation and Instent restenosis. Mechanical stimuli have been shown to affect cell behavior, namely cell proliferation and apoptosis. Using a preclinical testing device, designed in-house, SMC behavior was investigated in response to alterations in the mechanical environment within a mock artery following a stenting procedure. The device should provide insights into restenosis development and hence provide better stent design indicators and enable early-stage evaluations of new stent designs.
The novel in-house bioreactor consists of a perfused stented Sylgard mock coronary artery into which physiologic and pathologic levels of wall strain can be generated along with fluid shear stress conditions. Tests to date using the bioreactor have identified that the level of cyclic strain has a temporal antiproliferative and proapoptotic effect on SMC in vitro. In fact, the proliferative and apoptotic capacity of SMC was found to be highly dependent on the amplitude of the cyclic strain rather than the mean strain and independent of shear stress. These data provide evidence for the use of more compliant stent designs to maintain the antiproliferative effect of cyclic strain on SMC and therefore reduce restenosis.
Future work is focused on the use of this novel bioreactor to evaluate the influence of drug-eluting stents and novel stent designs on SMC growth.
Alun Lumsden
Methodist DeBakey Heart and Vascular Center, Houston, Texas
Endovascular interventions are currently performed manually under fluoroscopic guidance. This requires radiation exposure and is dependent on the skill and dexterity of the proceduralist to achieve the correct and safe access and perform the appropriate intervention. Robotics have been introduced into vascular education, vascular laparoscopy, and intravascular interventions. Robotic systems are a valuable tool to teach basic endovascular skills and to perfect intervention-specific skill sets. The use of these systems can result in a reduction learning period and detection and correction of erroneous behavior patterns and allow evaluation of the capabilities obtained. Final goals are a drastic reduction in learning curves, better technique, and a significant reduction in surgical errors and technical complications. This improves patient safety and quality of care. Total laparoscopic aneurysm resection operating times and the aortic cross-clamping period are significantly reduced by the addition of a robot to facilitate the surgical procedure. Robotic-directed catheter systems enable precise manipulation, stable positioning, and minimum instrumentation of the aorta and its branches while minimizing radiation exposure. Vascular robotic linked to a three-dimensional imaging environment offers the next incremental advance in the practice of vascular surgery.
Colin Bicknell, C V. Riga, M. Hamady, Nick Cheshire
Sheffield Vascular Institute, Sheffield, United Kingdom
Three-dimensional navigation techniques have been investigated in an in vitro model. An electromagnetic system has been used to accurately navigate through vessels by integrating detailed preprocedural CT imaging with real-time information from an electromagnetic system.
Alun Lumsden
Methodist DeBakey Heart and Vascular Center, Houston, Texas
Accurate imaging is the key to success in vascular surgery. Progression in magnetic resonance (MR) technology has allowed the development of dedicated whole-body MR systems with specially designed surface coils, the movement to higher field strength, and the implementation of parallel acquisition techniques, which have improved spatial resolution, shortened acquisition time, and allowed computerized flow dynamics to be incorporated into the diagnostic information. This has allowed MRA to move from a static cross-sectional picture with incomplete resolution to an anatomic and functional image, which can demonstrate real-time images and hemodynamics within a three-dimensional environment. Dynamic MR allows flow rates, pressure, shear stress, and wall motion of a vessel to be accurately modeled and can be used for diagnostic classification and clinical decision making. Dynamic MRA data sets can be used in computational modeling to preduct the progression of disease and the response to intervention. The presentation of real-time anatomic and flow provides the surgeon with an added and valuable tool in the evaluation of cardiovascular disease.
15:04 DISCUSSION
SESSION XIV: The Business of Vascular Surgery: How to Manage Our Future
Venue: Main Hall
Moderators: Jerry Goldstone, Cliff Shearman
Jerry Goldstone
Case Medical Center, Cleveland, Ohio
In the United States, vascular surgery training is controlled by two independent, voluntary, nongovernmental organizations. The Accreditation Council for Graduate Medical Education (ACGME) approves training programs, whereas the American Board of Surgery (ABS) and its Vascular Surgery Board set standards for certifying individual surgeons. New training schemes have been approved by these organizations. The two most common types of programs and number of trainees are as shown in Table 3.
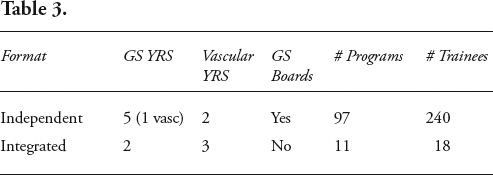
The major initiatives of the ACGME over the past 5 years have been the Outcomes Project, which is an effort to change from a process-driven to an outcomes-driven accreditation. This involves an emphasis on six defined physician competencies that programs are required to teach: patient care, medical knowledge, interpersonal communication, practice-based learning and improvement, systems-based practice, and professionalism. For surgical specialties, there is also operative/technical. The latter is of particular concern as the number and percentage of endovascular procedures continue to increase, leaving many residents inadequately experienced with open surgical procedures, of which there is an increasing complexity. The other major focus had been duty hours, beginning with the adoption in 2003 of a set of standards that included a maximum of 80 working hours per week. This highly controversial activity has recently become more so by the changes recommended by the Institute of Medicine. Obviously, the even more limited resident work hours adopted in the European community have figured prominently in the discussions.
The ABS has recently acknowledged that GS training no longer confers adequate training for vascular surgery. This is spelled out in a document outlining the curriculum for GS training based on the ACGME competencies. The other major initiative of the ABS is a greatly expanded recertification program called maintenance of certification, which is far more than a written examination every 10 years. The effort for vascular surgery to become an independent specialty that started in 1986 is currently dormant. Training enough vascular surgeons with the requisite knowledge and technical skills in the face of increasing public scrutiny, increasing educational requirements, and reduced training time to meet the needs of an aging population are challenges faced by surgical educators in the United States and elsewhere.
Cliff Shearman
Univerity of Southampton, Southampton General Hospital, Southamptom, United Kingdom
In the United Kingdom, a number of factors are driving centralization of vascular services toward large centers where all facilities are available 24 hours/day. Most pressing is the European Working Time Directive (EWTD), and by August 2009, hospitals will have to demonstrate that medical staff are compliant with a 48-hour working week, making it impossible for smaller units with low staff numbers to achieve. Other factors are driving centralization of vascular services. Outcomes are demonstrably better in high-volume units, and economic pressures mean that it is not sustainable to maintain small units.
Vascular surgery and training are likely to benefit. A concentration of large numbers of cases in one unit will allow the trainee to gain experience more quickly. Trainer time and experience will be more available to gain the most out of each training opportunity. The shortened working time will mean that trainees’ time has to be focused more on training rather than service, but, again, this can only be achieved in large units.
On balance, the centralization of vascular services can only benefit training, but there will have to be a concerted effort on the part of trainers to capitalize on this opportunity in the face of the challenge of EWTD. Provision of service work will remain a challenge, but as that is ultimately what trainees are training for, it does not seem impossible to achieve both high-quality training and excellent service.
Martin Feeley
Adelaide/Meath Hospital, Dublin, Ireland
Vascular surgery in Ireland, as in the rest of the Western world, is evolving at quite a pace. We are fortunate in that in April 2000, the Department of Health published a document along IAVS guidelines putting in place a structure whereby every citizen has access to both emergency and elective specialist vascular surgery care.
It has been quite evident for some time that vascular surgery specialization would inevitably lead to the point whereby vascular surgeons would not be trained or be capable of delivering a general surgery on-call service. This has been accepted by Irish vascular surgeons for a number of years. However, the implementation of a program where vascular surgeons do not provide any general surgery services, elective or emergency, is not easily achieved for many reasons, not least of which is the fact that if all vascular surgeons come off call, the duty becomes onerous for our general surgery colleagues. With the implementation of the national cancer strategy, the general surgery on-call dilemma is destined to become a crisis. Nevertheless, at the moment, in two of the nine vascular centers, the vascular surgeons provide no general surgical on-call duty, and two vascular surgeons in other centers do not provide a general surgery on-call service.
With the decision taken at the last Vascular Surgery Society AGM to move toward vascular surgery as a monospecialty, it is anticipated that within the foreseeable future, vascular surgeons will not provide any general surgery call.
For the past number of years, there has been an acute awareness of the importance of endovascular techniques in the armamentarium of the vascular surgeons. Therefore, there has been tremendous emphasis on trainees learning these techniques in the Irish centers and in obtaining fellowship posts in endovascular centers abroad for our trainees. As a result, all recent appointees are accomplished endovascular practitioners. The IAVS is working with the Royal College of Surgeons in Ireland to develop a training program that will dramatically change the emphasis for vascular surgery trainees, with little time spent in general surgery and its subspecialties but with the emphasis on conventional and endovascular training.
The IAVS feels that we are advanced in our preparations for the provision for vascular surgery services for the future, but there is still considerable work to be done in developing the comprehensive training program. The twin objectives are, first, to keep abreast of developments and pass on a robust healthy state-of-the-art service and, second, to ensure that our young surgeons are trained and capable of taking up the vascular surgery baton.
James Stanley, Kim Eagle, Linda Larin, David Pinsky, Richard Prager
University of Michigan, Ann Arbor, Michigan
Sam Ahn
University of Vascular Associates and DFW Vascular Group, Los Angeles, California and Dallas, Texas
Larry Hollier
LSU Health Sciences Center, New Orleans, Louisiana
Aneurysm Outreach Inc. (AOI) is a nonprofit organization that is dedicated to mobilizing people and resources to diagnose abdominal aortic aneurysms. The primary goals are to promote public awareness about the threat of aneurysms, especially the fact that certain families have a predisposition toward their occurrence, to stimulate and fund genetic research through advocacy and donations, and to coordinate a support network for those affected or at risk and their families.
AOI has enlisted the support of vascular surgeons, ultrasound technicians, and imaging companies to donate their time and resources to conduct free aneurysm screenings. The screenings include a general vascular history and physical examination, a family history, and ultrasound examination of the abdomen.
Between 2001 and 2009, 44 screenings have taken place in 14 cities in two states. In the screenings conducted, 6,737 patients were evaluated for abdominal aortic aneurysm (aortic size 4 cm or greater), which were identified in 222 of the patients (3.3%). Those found to have an aneurysm were given an opportunity to have a consultation with a vascular surgeon regarding options for treatment.
15:48 DISCUSSION
16:00 COFFEE BREAK
Venue: Exhibition Hall
16:20 SESSION XV: Bioconvergence: A Model to Deliver Excellence in Healthcare
Venue: Main Hall
Moderators: Finbar Dolan, Sharon Higgins, Frank Veith
17:20 SESSION XVI: Bioconvergence: A Catalyst for Innovation
Venue: Main Hall
Moderators: Mike Devane, Sherif Sultan