
Abstract
We report the case of a false aneurysm at the origin of the anterior tibial artery complicating upper tibial osteotomy. The proximally located lesion compressed the posterior tibial nerve, and despite successful decompression, the patient suffers from probably irreversible neurologic after-effects. Even though it is rare, this complication must be considered when faced with leg pain consecutive to upper tibial osteotomy without deep venous thrombosis.
Arterial vascular complications during orthopedic surgery of the lower limbs are rare and feared because in certain dramatic cases, they may cause limb amputation. We report the case of a voluminous false aneurysm of the anterior tibial artery with a widest diameter of 75 mm and the additional complication of paralysis of the posterior tibial nerve, which was diagnosed several months after opening wedge osteotomy. This false aneurysm was opened, and vascular continuity was achieved with a venous bypass. Apart from the fact that this complication seldom occurs after upper tibial osteotomy, the present case is notable for the location of the false aneurysm and the neurologic compression it caused.
Clinical Case
A 63-year-old man presented with the following clinical history: stable coronary disease after two myocardial infarctions, high blood pressure, and tobacco use. He suffered from medial unicompartmental arthritis in the right knee with slight cartilage destruction, for which various arthroscopies with local infiltration of corticosteroid had been performed, with incomplete pain resolution. He had medial opening wedge osteotomy of the right knee. The immediate postoperative course was uneventful, and the anatomic result was satisfactory. The patient was discharged after a routine postoperative duplex sonogram showed no venous thrombosis.
During the following weeks, the patient experienced intensifying pain resistant to pain medications in the right leg. A clinical examination did not detect signs of deep venous thrombosis, but right-sided distal pulses were found. Hypoesthesia in the external popliteal sciatic nerve area was also found, which led us to prescribe clonazepam.
After a few weeks of persistent pain, the patient complained of swelling of the lower limb. Venous duplex ultrasonography revealed right-sided minimal sural venous thrombosis without deep venous thrombosis associated with a muscle hematoma. As the patient was faced with persistent pain, computed tomography (CT) was performed, which showed a narrowed lumbar canal; laminectomy was also performed but was unsuccessful. After a diagnosis of algodystrophy was made, another arterial and venous duplex scan of the lower limbs showed patency of the deep venous network and a large false aneurysm of the lower popliteal artery. A CT scan revealed a false aneurysm in the posterior compartment of the leg communicating with the arterial lumen at the level of the horizontal part of the anterior tibial artery (Figure 1). The maximum diameter of this lesion was 75 mm. CT angiogram with three-dimensional reconstruction clearly demonstrates the mass effect on tibial vessels (Figure 2); the volume of the lesion was evaluated at 200 cc with Osirix software (OsiriX Foundation, Switzerland) (Figure 3). Conventional surgery was performed through a medial approach; the popliteal artery was controlled. The false aneurysm did not allow for control of the anterior tibial artery; thus, the distal popliteal artery was clamped, the false aneurysm was opened, and thrombus was removed. This maneuver enabled identification of two perforations at the origin of the tibial artery feeding the false aneurysm. The anterior tibial artery could not be repaired directly, and a short bypass with a reversed saphenous vein was performed between the distal popliteal artery and the healthy anterior tibial artery distal to the perforations. To gain adequate access, a cruciate incision in the interosseus membrane was made, and the end-to-end distal anastomosis of the anterior tibial artery was performed first.
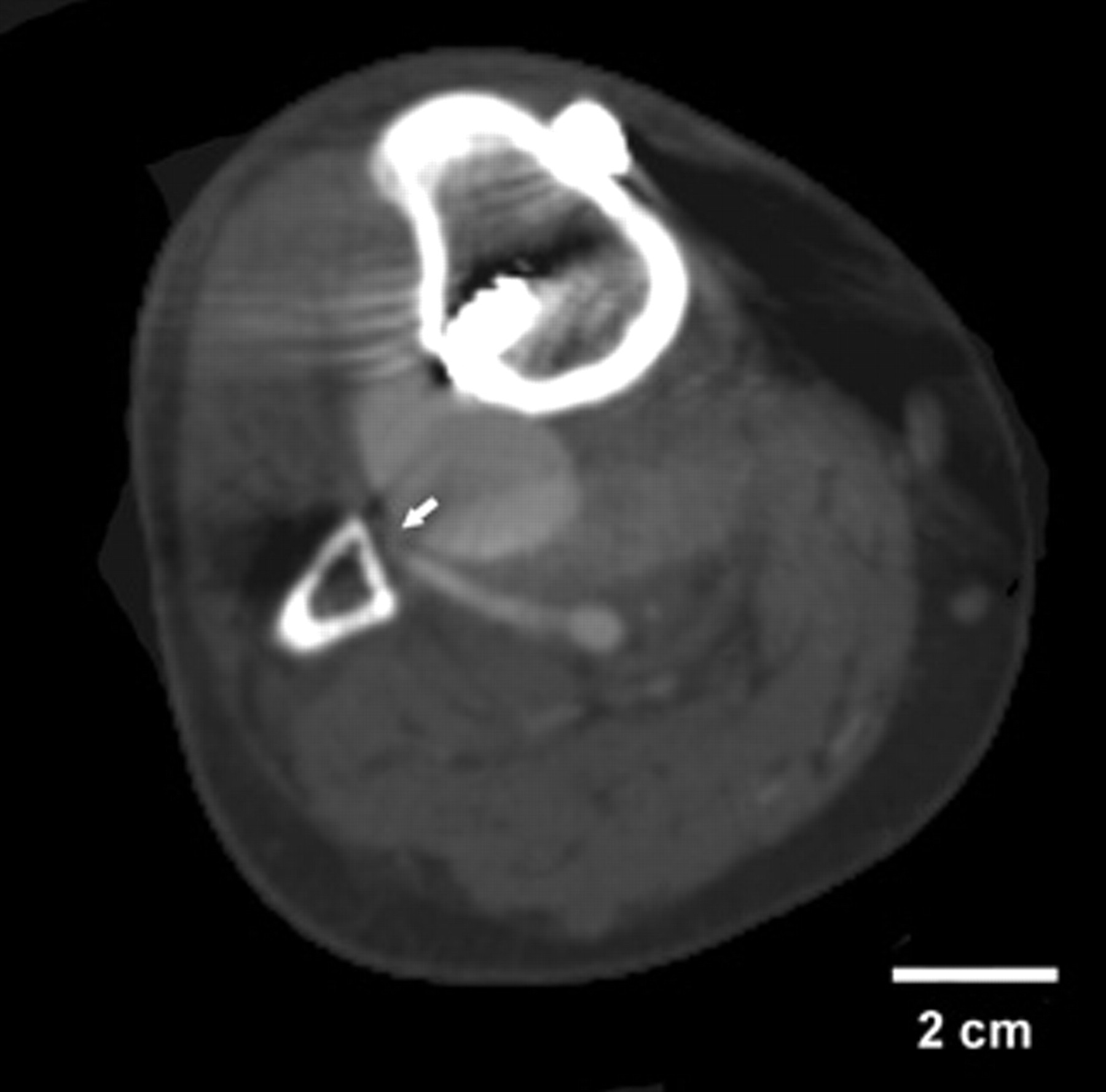
Computed tomographic scan showing the false aneurysm arising from the horizontal part of the anterior tibial artery. The white arrow shows the origin of the false aneurysm.

Three-dimensional reconstruction of the diagnostic computed tomographic scan. The development of the false aneurysm is essentially posterior, with important shifting of the vascular pattern (Osirix software).

Three-dimensional reconstruction of the diagnostic computed tomographic scan. The entire volume evaluation of the false aneurysm is shown in red (Osirix software).
The false aneurysm was opened, and vascular continuity was achieved with a venous graft. The intervention considerably improved pain symptomatology in the right lower limb, but the patient reported significant walking difficulty associated with plantar arch paresthesia of the right foot. An electromyogram at 6 months showed total unexcitability of the motor and sensitive branches of the posterior tibial nerve.
Discussion
Arterial complications during orthopedic surgery of the knee are exceptional. The frequency reported in connection with prosthetic replacements of the knee is 0.03 to 0.2%. 1 It is less than 1% in knee arthroscopy 2 and 0.4% in upper osteotomy of the tibia. 3 Generally, in the case of arterial lesions consecutive to high tibial osteotomy, the lower popliteal artery suffers the most. The 90-degree flexion of the knee during osteotomy is considered to decrease the risk of damage of the popliteal artery. The danger seems to be far less the distancing of the artery from the posterior aspect of the tibia than the absence of tension of the popliteal artery during flexion. 4 Generally, the popliteal artery is flexible and spared from atherosclerosis for a long time. With regard to the lesions of the anterior tibial artery in the course of upper tibial osteotomy, they mostly occur during a lateral approach by direct damage during exposure of the bone surface or during resection of the inferomedial part of the head of the fibula. 5
It is surprising that a proximal arterial perforation should cause a false aneurysm of the anterior tibial artery to compress the posterior tibial nerve. The origin of the false aneurysm was situated above the interosseous membrane; the aneurysm developed medial to the interosseus membrane into the posterior muscles of the leg between the interosseous membrane in the front and the soleus muscle in the back. In this space, the peroneal artery and the posterior tibial vascular-nervous bundle are located. Increasing in volume in that osteoarticular nonextensible space, the false aneurysm mainly compressed the tibial nerve, causing probably irreversible damage. False aneurysm development led to an important anterolateral displacement of the interosseous membrane.
As a protocol, systematic postoperative duplex ultrasonography is performed in the orthopedic surgery unit even if there is no suspicion of deep venous thrombosis. As the patient was facing persistent pain, duplex ultrasonography was performed again before the lumbosacral spine CT. In France, these examinations are not recorded on tape, and we were able to review only the report of the examinations. The first examination reported the absence of any abnormality. On the second duplex scan, retrospectively, the presence of such an important hematoma might have been considered abnormal, especially taking into account the delay after surgery, and should have led to more aggressive diagnostic investigations on the leg instead of the spine. Unfortunately, this duplex examination did not explore the arteries.
We hypothesize that the arterial traumatism occurred with the distal screw placed in the tibia. The neck of the false aneurysm is located in the axis of that screw. It is therefore possible that the drilling of the tibia perforated the horizontal part of the anterior tibial artery. This hypothesis is undermined by the rupture of the internal periosteum of the fibula in the axis of the fourth screw, as seen in the CT scan (Figure 4). Considering that the rotating worm could only have severed the anterior tibial artery, it might be assumed that it was damaged secondarily by “hooking” during the measuring process. The distal screw was inserted into the tibia at 45° vertically in a posterolateral direction, which was defined as dangerous for the anterior tibial artery by Rubash and colleagues in their anatomic study on the drilling of the tibial element of the total knee prosthesis. 6 A strictly anteroposterior drilling angle represents a danger for the lower popliteal artery and the tibioperoneal trunk. It is therefore suggested to keep in mind that a posterolateral angle at the corresponding height is likely to cross the horizontal segment of the anterior tibial artery. Moreover, to avoid arterial trauma, it is also recommended when performing the osteotomy stabilization to reach the opposite osseus cortical only if it is necessary to obtain a firm reconstruction.
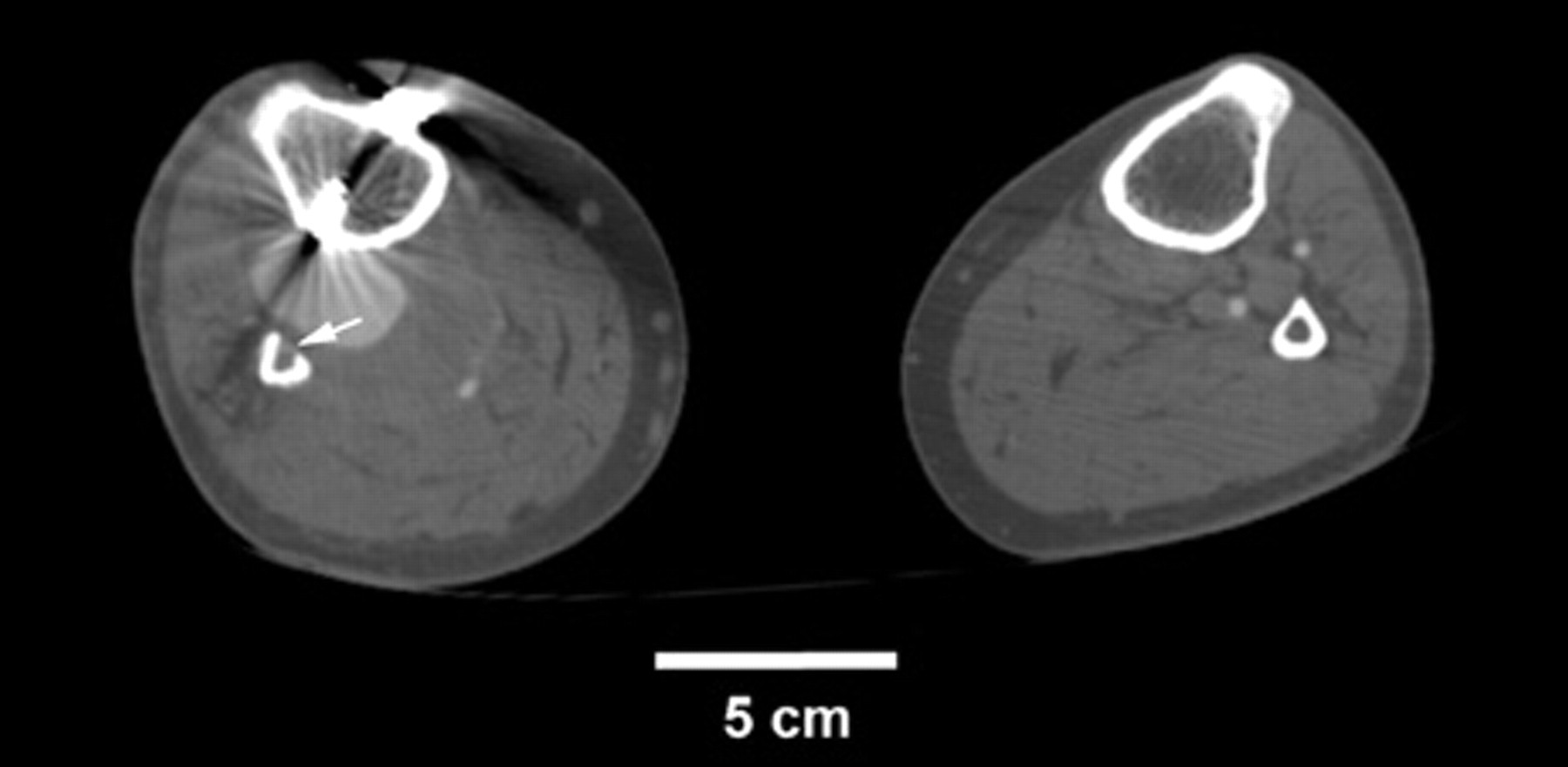
Computed tomographic scan showing the axis of the fourth screw of the osteosynthesis. The white arrow shows the gap of the internal fibula periosteum.
False aneurysms may remain unnoticed, developing spontaneously into thromboses and complete regression. 7 They can also progressively increase in volume and compress adjacent structures, notably nerves and veins, causing swelling, pain, and paresthesia. These clinical signs generally are delayed. 8,9 In this case, the difficulties of diagnosis explain the delay leading to sequelae. Routine arterial and venous duplex ultrasonography in the case of unexplained pain after this kind of procedure should be recommended.
The feasibility of many endovascular techniques, which are less invasive than open surgery, has been demonstrated. 10 In most of these cases, the endovascular technique requires thrombosis of the artery with the false aneurysm, which may compromise the viability of the limb in a patient with atherosclerosis. For our patient, conventional surgery was chosen and provided a good result because it allowed for quick and very efficient decompression of the posterior tibial nerve and preserved the diseased artery. The large volume of the lesion was also a reason for choosing conventional surgery. These endovascular techniques lose many of their advantages if they are associated with a surgical evacuation of the hematoma, and we might consider them preferentially for small false aneurysms. Nevertheless, in the literature, secondary pain to a relatively small false aneurysm generally disappears 48 hours after false aneurysm thrombosis.
Conclusions
We report the case of a rare vascular complication following medially performed upper opening wedge osteotomy. After several months of diagnostic uncertainty, duplex ultrasound exploration revealed a large false aneurysm that had developed in the horizontal part of the anterior tibial artery and was compressing the tibial nerve. When performing medial high tibial osteotomy, one should keep in mind the position of the horizontal segment of the anterior tibial artery. In the postoperative course, an unusual hematoma detected during ultrasonography might hide a vascular complication. Therefore, when confronted with these symptoms, CT should be recommended.
Footnotes
Acknowledgment
Financial disclosure of authors and reviewers: None reported.