
Abstract
Isolated dissection of the origin of both celiac and superior mesenteric arteries is a rare vascular pathology with limited management guidelines. The presentation is generally nonspecific, most often manifesting with epigastric pain radiating to the back. A high diagnostic index of suspicion and stepwise management are essential for a successful outcome. This case report details the clinical course of a 57-year-male who presented with a 2-week history of epigastric discomfort with back pain and was found to have focal celiac artery dissection with aneurysmal dilation of 1.2 cm. His vital signs were stable, and the physical examination was unremarkable. At this time, he was placed on antiplatelet medication and was scheduled for endovascular repair of his celiac aneurysm with a covered stent graft. Two weeks later, recurrent abdominal pain prompted a repeat computed tomographic scan that revealed sequential superior mesenteric artery (SMA) dissection. The patient was admitted and anticoagulated. A complete workup ruled out underlying collagen vascular and autoimmune pathology. He remained stable, with significant symptomatic improvement. After 6 months, anticoagulation was discontinued and antiplatelet therapy was instituted for long-term management. Subsequent operative or endovascular intervention was not required. The patient was continuing to do well on his 18-month clinical follow-up. There are 71 cases of SMA and 12 cases of celiac artery dissection in the literature. This report outlines this rare presentation of isolated, proximal sequential celiac artery and SMA dissection. This case illustrates that conservative management may be warranted in uncomplicated, isolated visceral arterial dissection.
Arterial dissection is defined as an arterial wall cleavage and subsequent hematoma creation of a false lumen. 1 Isolated arterial dissection without aortic pathology has been reported most commonly in carotid and renal arteries but rarely in mesenteric vessels. 2,3
Seventy-one cases of superior mesenteric artery (SMA) and 12 cases of celiac artery (CA) isolated dissection have been reported in the literature dating back to 1959. This scarcity of literature limits data available to the clinician, resulting in clinical management challenges in an area warranting further research.
Case Report
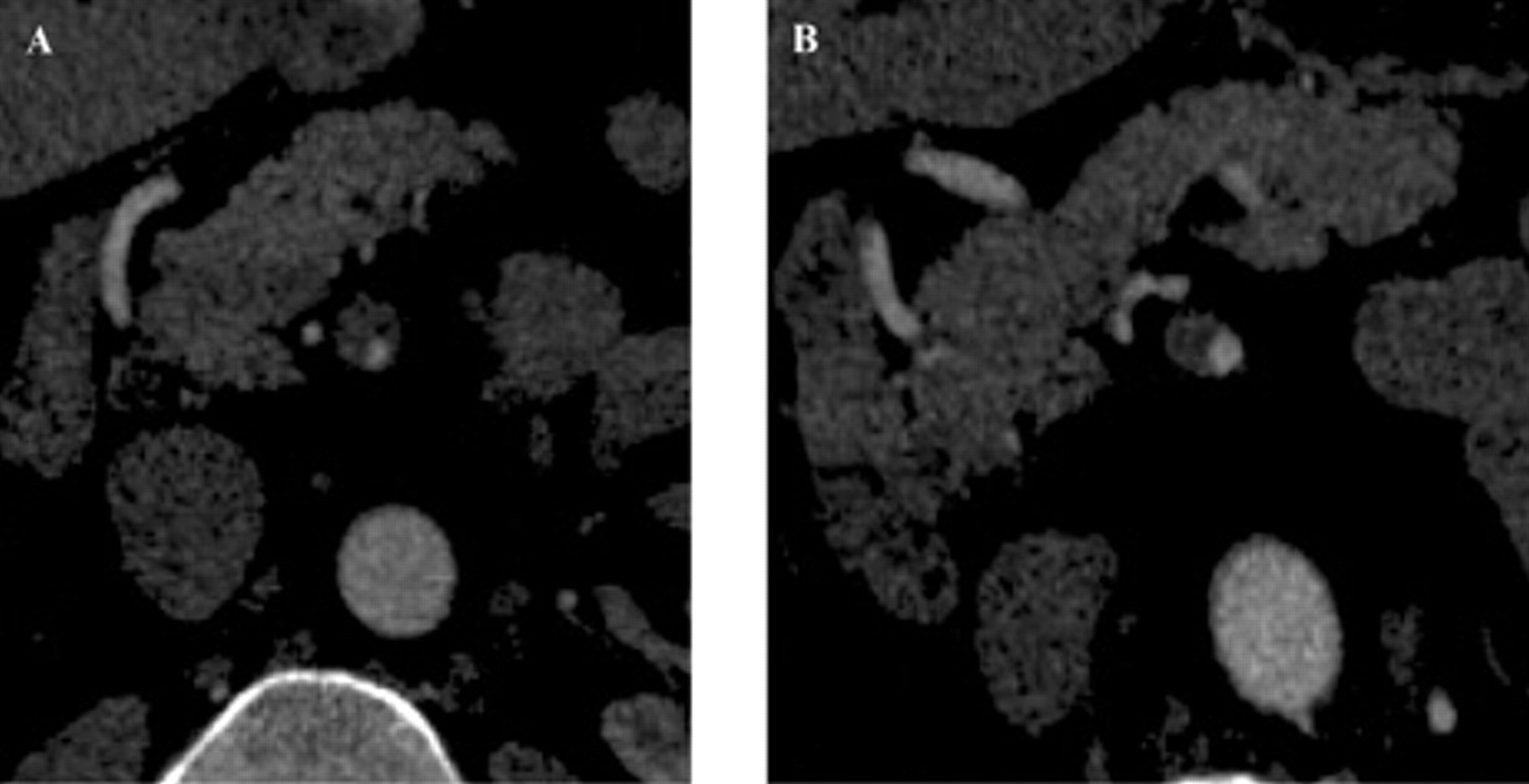
A 57-year-old male presented with a 2-week history of abdominal pain, bloating, nausea, and back pain of 8 on a scale of 10 radiating to his upper back. On presentation, he was asymptomatic and denied any constitutional symptoms. His past medical history was remarkable for mild hypertension with no history of abdominal trauma, connective tissue disease, vasculitis, or infectious disease. Laboratory data were within normal limits, including complete blood count with differential, erythrocyte sedimentation rate, and blood cultures. A computed tomographic (CT) scan revealed focal CA dissection with aneurysmal dilation of 1.2 cm (Figure 1). A whole-body indium white blood cell scan was negative. There was no evidence of vasculitis or ankylosing spondylitis. Because the patient was completely asymptomatic, full anticoagulation was not indicated. He was started on oral antiplatelet therapy (clopidogrel [Plavix]) prophylactically. He was scheduled for elective exclusion of the CA aneurysm with a stent graft; however, we waited for the inflammation to subside and for completion of ongoing workup regarding the differential diagnosis.

(A & B) Axial contrast-enhanced computed tomographic scan through the upper abdomen shows an intimal flap (arrow) in the celiac trunk. This finding is consistent with celiac artery dissection.
Two weeks later, the patient presented with severe abdominal pain (self-rated 7 on a scale of 1 to 10) and bloating. His physical examination was remarkable for epigastric tenderness without peritoneal signs. Repeat CT was performed with M2S reconstruction. In addition to the previous CA dissection, an SMA dissection with thrombus extending approximately 4 cm from the SMA origin was noted (Figure 2). Abdominal aortic ultrasonography (US) demonstrated elevated velocities in the SMA of 593 cm/s with a dissection flap; the velocity in the celiac trunk was 403 cm/s (Figure 3).
Axial contrast-enhanced CT scan shows a narrowed true lumen of the superior mesenteric artery before (A) and after (B) treatment.

Sonogram showing a dissection flap in the superior mesenteric artery.
The patient remained hemodynamically stable with vague abdominal pain but without peritoneal signs and was admitted for anticoagulation. Sodium heparin infusion was initiated. Within 8 hours, the patient's abdominal pain improved dramatically. In-hospital therapy consisted of bowel rest, sodium heparin intravenous anticoagulation, and pain management. The patient was completely pain free by hospital day 3, and a repeat abdominal computed tomographic angiogram (CTA) revealed a markedly small thread-like true lumen of the SMA that filled the distal small bowel branches. Rheumatology consultation, based on the absence of constitutional symptoms with normal acute-phase reactants, discounted a diagnosis of isolated vasculitis, and glucocorticoid therapy was not recommended. Carotid duplex imaging showed minimal carotid disease with no evidence of dissection, and no aortic dissection was evident on chest CTA. The patient tolerated diet advancement. Coumadin (warfarin sodium) was initiated. A therapeutic international normalized ratio (INR) of 2.5 was achieved on hospital day 4, and he was discharged to home. At the 6-month follow-up, the patient denied abdominal discomfort, bloating, and weight loss. Repeat CTA showed improved CA and SMA dissection with decreased inflammation (Figure 4). The patient continued to do well at the 18-month clinical follow-up.
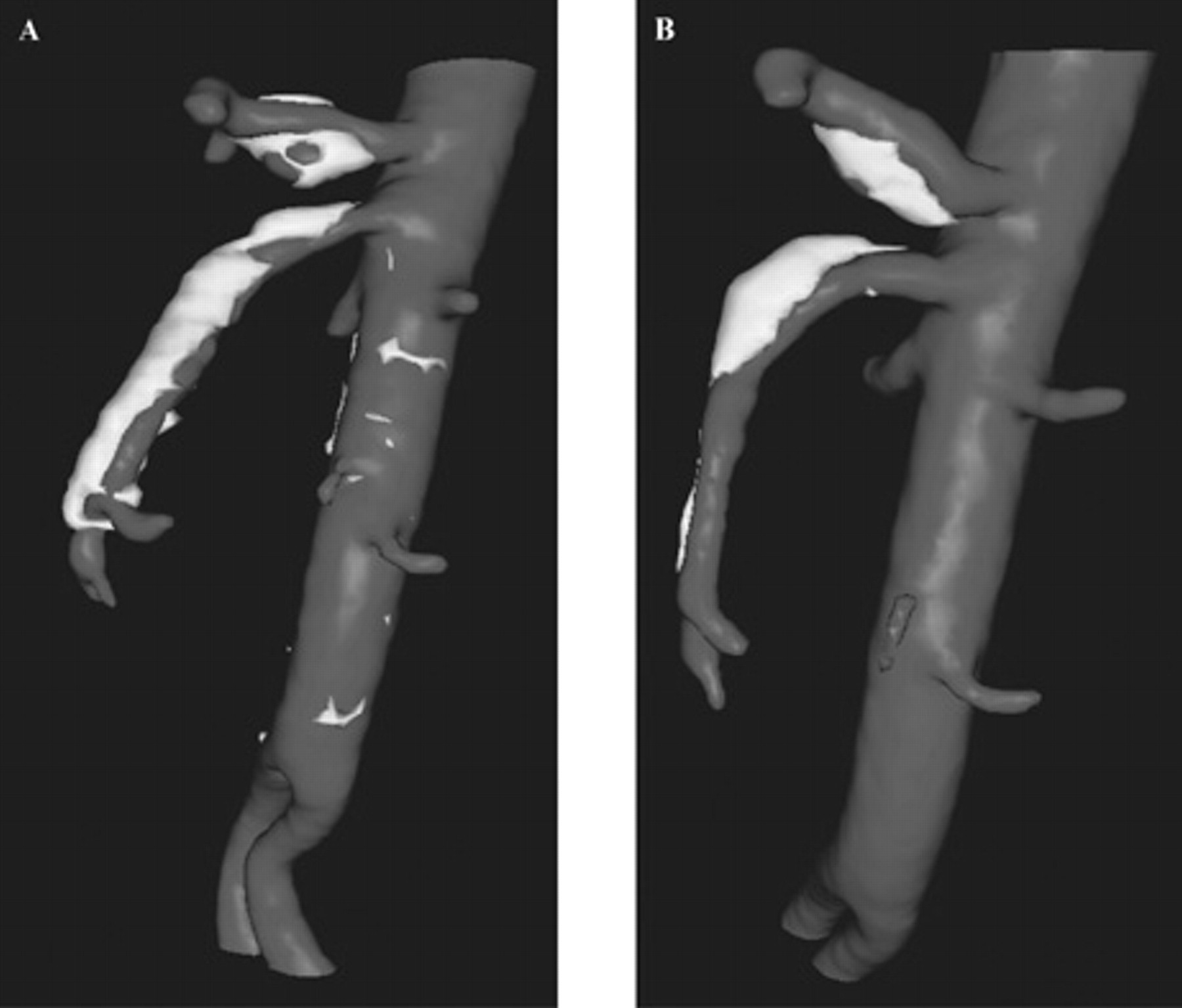
Sagital reformatted computed tomographic scan showing both celiac and superior mesenteric arteries before (A) and after (B) conservative management for 6 months.
Discussion
Spontaneous visceral artery origin dissection of both celiac and superior mesenteric arteries is an exceptionally rare event. Since the first case reported in 1947, only 71 cases of SMA and 12 cases of CA dissection have appeared in the literature (see Table 1 for a synopsis of the recent literature). 3,4 This case report documents the very rare presentation of simultaneous dissection of CA and SMA and subsequent management of this difficult vascular disorder.
Synopsis of CA/SMA Dissection Literature Review: 1985–2008
CA = celiac artery; CT = computed tomography; NA = not available; PTFE = polytetrafluoroethylene; SMA = superior mesenteric artery.
A literature review indicated that the majority of patients presenting with visceral dissections are male, with an average age of 55 years. 1,3,5 Given the overall older age and lack of associated mechanical injury, it is unlikely that the etiology of this disorder is traumatic in nature, as in cervical dissections-nor does it appear related to malignant hypertensive disorders frequently associated with aortic dissections. The presentation can include abdominal pain, nausea, vomiting, bloating, or weight loss. Patients with SMA lesions are more often symptomatic than those with CA lesions. 5,6 Overall, however, patients with spontaneous dissection of the splanchnic arteries are most often asymptomatic, and development of significant end-organ ischemia is relatively rare. 7 Owing to the nonspecific presentation of mesenteric artery dissections, it must be included in the differential diagnosis of abdominal pain, with the caveat that it is an exceedingly unusual finding.
Recommended workup includes cytoplasmic anti-neutrophil cytoplasmic antibodies (c-ANCA)/perinuclear-staining anti-neutrophil cytoplasmic antibodies (p-ANCA) autoantibodies and whole-body indium white cell scan to rule out collagen vascular or infectious etiologies. Risk factors include arteriosclerosis, hypertension, fibromuscular dysplasia, cystic medial necrosis, and elastic tissue disorders (Marfan disease, Elhers-Danlos disease). Trauma and pregnancy have been cited as potential precipitants. 1,5,8 Often, however, as in our case, no etiology can be found despite extensive investigation. 7,9,10
Abdominal ultrasound (US) 10 may be helpful if aneurysmal dilatation or the intimal flap is observed. However, US is an insensitive tool for the initial diagnosis owing to inconsistent flap visualization, air swallowing associated with abdominal pain, and the specialization required for mesenteric duplex examination. US is useful postdiagnosis to assess the physiologic impact and to track the pathologic process. In our patient, the abdominal duplex scan revealed elevated velocities in the celiac axis and SMA with dissection in both vessels.
CTA is a much more sensitive diagnostic modality because it allows visualization of the false lumen together with the intimal flap during the arterial phase. 5,11,12 Other findings that may be encountered during the CTA are segmental fat infiltration, dissection extension, and an additional aneurysm, such as in the hepatic artery. 5,11,12 It may also reveal signs of acute ischemic bowel (lack of bowel wall enhancement, mesenteric edema) and provide an estimation of the extent and severity of the lesion. The portal phase gives an indication of the severity of mesenteric ischemia by showing mesenteric or portal venous gas that is often associated with bowel necrosis.
Mesentric angiography (MA) is a valid diagnostic tool, and it can give specific details regarding complications of dissection such as lumen thrombus, embolization, and measurement of gradient across the SMA lesion. However, MA has its own limitations: it is invasive, it may cause embolization or dissection, and it may be questionable, especially if an inflammatory aneurysm is not ruled out. On the other hand, CTA documents better details than MA, which offers not only luminal but also cross-sectional axial examination of all relevant anatomy.
Unlike other dissections, visceral mesenteric dissection is unique in its morphology, with alternative areas of narrowing and dilation resulting in a characteristic beaded shape. Our patient presented with dissection 1 cm from the SMA origin. Reportedly, SMA dissection typically begins 1.5 to 3 cm distal to the origin of the SMA, with differing clinical presentations according to the extent of dissection. 7
Management of visceral artery dissection includes medical and surgical options. Despite clinical diagnostic and management experience gleaned from individual case reports and case series, there is no established standard for treating visceral artery dissection. Suggested medical treatment includes antihypertensives, antiinflammatory drugs, and steroids (in case of vasculitis) and anticoagulation to prevent thromboembolic complications. 7,13 Anticoagulation therapy continued for 3 to 6 months with a target INR of 2.0 to 3.0 and with strict blood pressure control is recommended. 14
Our patient presented initially with focal CA dissection. He was asymptomatic; therefore, full anticoagulation was not indicated, and we treated him prophylactically with an antiplatelet agent. When he developed severe abdominal pain and was found to have simultaneous dissection of both the CA and the SMA, we placed him on full anticoagulation.
The extent of subsegmental branch involvement, bleeding, or end-organ injury determines the prognosis. 15 Based on standard surgical guidelines, operative or endovascular options should be reserved for patients with persistent signs of ischemia despite adequate anticoagulation or those with uncontrolled hypertension or progression of the dissection. 1,5,14,16 Surgical intervention was considered for our patient, particularly in light of dissection extension from the CA to include the SMA. However, our patient's clinical course rapidly improved with conservative treatment; the risks due to the complexity involved with repair outweighed the potential benefits given this rapid improvement.
Open repair includes thrombectomy, aneurysmorrhaphy, intimectomy with patch angioplasty, ligation, resection, venous graft bypass, or arterial bypass graft. Surgery has been advocated as a standard of care if the vessel is operatively accessible and the clinical symptoms warrant this. The first operation for an SMA dissection was reported by Krupski and colleagues in 1985, who performed an SMA thrombectomy, “intimectomy,” and vein patch angioplasty on a 51-year-old female with spontaneous SMA dissection. 17 They recommended that symptomatic patients with SMA dissections undergo operative repair because the SMA is a “surgically accessible vessel.” In 1992, Cormier and colleagues reported the successful surgical management of four SMA dissections with bypasses, intimal flap excisions, and tacking procedures. 18 Following review of 10 previously reported cases of SMA dissection, they concluded that a more successful outcome justified an operative approach to such lesions.
Endovascular treatment is an attractive option in patients with high surgical risks, involving stent placement or thrombolytics. 19 Bare stents may be helpful in a dissection to cover the entry points; however, in case of focal aneurysmal disease, covered stents minimize pressurization of the aneurysm sac. However, the data for a comparison with surgery are not available.
Conclusion
In conclusion, spontaneous mesenteric artery aneurysm and dissection is rare. It may have been underreported in the past as these dissections are more frequently documented as a result of the progress of imaging modalities, such as US, CT, and angiography. Treatment remains controversial. Surgery and endovascular procedures are indicated in acute symptomatic forms with suspicion of mesenteric ischemia, but in uncomplicated cases, conservative management with anticoagulation may be sufficient. Retrospectively, our patient improved with medical management; however, stenting may be an option with his initial presentation. His clinical improvement on full anticoagulation highlights the applicability of medical management.
Footnotes
Acknowledgment
Financial disclosure of authors and reviewers: None reported.