
Abstract
Vascular injuries are manifested by life-threatening hemorrhage or limb loss and their diagnosis and treatment are challenging. Angiography is beyond the capability of available teams during wartime. Thus, computed tomographic angiography (CTA) may become a major triage tool. This study reports on the presentation, diagnosis, management and outcome of combat vascular injuries with emphasis on the utility of CTA. Presenting signs and symptoms, means of diagnosis, treatments and results of all combat sustained vascular cases were collected and compiled with follow-up.
Of 511 patients, 39 patients (7.6%) with vascular injuries were admitted. Injuries were penetrating and accompanied by soft tissue and bone insult. Diagnosis was made by CTA in 62% and by surgical exploration in 38%. Extremity arteries were injured in 72% of cases. Treatment included surgical and endovascular techniques. Complications: one late amputation, 5% thrombosis, 24% wound infections with no mortalities or early amputations.
Although similarities exist between this experience and recent wartime reports, differences are apparent including the effectiveness of CTA. High index of suspicion and liberal use of CTA allows for an early and accurate diagnosis of a vascular injury resulting in high rates of limb salvage and low mortality. CTA should be the first line modality for diagnosis of vascular injuries, reserving angiography for endovascular treatment.
Keywords
Although several recent wartime reports on vascular injury management are larger than the experience presented herein, none are able to describe such a unique and concise experience of all the casualties being treated at one established urban trauma center.
Vascular injuries are manifested by life-threatening hemorrhage or by limb loss. Such injuries, with a single entry and/or exit wound, lead to surgery immediately after the primary assessment in the emergency room (ER). With multiple injuries, imaging is necessary for diagnosis and the choice of treatment. Angiography is considered the gold standard diagnostic modality for a vascular injury but is invasive and time consuming. During wartime, the number of simultaneously admitted patients in need of vascular assessment is above and beyond the handling capability of invasive radiology teams and available angiography suites. Computed tomographic angiography (CTA) is routinely performed as part of the trauma patient workup. Intravenous administration of contrast medium, according to study protocol, at the same time provides enhancement of the arterial tree. Thus, CTA, by virtue of its availability, quick data acquisition, and reconstruction, becomes a major triage tool. This was tested in a 33-day surge of casualties stemming from sustained urban combat.
Patients and Methods
Study Location and Dates
Rambam Health Care Campus (RHCC), established in 1938, is located in Haifa on the Mediterranean Sea. RHCC is the largest medical center in northern Israel and serves over 2 million citizens. With over 1,000 beds, RHCC delivers the full spectrum of health care services and is the only established level I trauma center in northern Israel.
The 33-day conflict in Lebanon in the summer of 2006 necessitated that RHCC, located merely 60 km from the Lebanese border, act under fire. Altogether, 511 wounded patients (soldiers and civilians) were admitted to our ER, excluding nonphysical casualties.
Diagnosis and Management Strategies
Patients were evacuated by air (mostly soldiers) or by ambulances (mostly civilians). The ER contained four basic assessment and primary treatment points for critically, severely, moderately, and mildly wounded patients. A fifth anxiety station was positioned outside the ER. Casualties were referred to the specific station by the admitting triage officer in charge. On arrival, our level I trauma center ER patients underwent primary assessment, leading to treatment and obligatory scans (cervical spine and chest radiography, focused assessment with sonography for trauma [FAST], ultrasonography). Damage control resuscitation with permissive hypotension, minimal crystalloid infusion, and early fast warmed blood transfusion were employed.
Next, based on the patients' condition, the station triage officer and the ER team sent patients either directly to the operation room or to radiology suites for additional studies, such as CTA, angiography, or extremity radiography.
Hard signs for a vascular injury were active arterial bleeding, expanding or pulsating hematoma, limb ischemia, and a thrill. Soft signs were a history of a moderate hemorrhage, hypovolemic shock, peripheral neurologic damage, decreased peripheral pulses, and injury in proximity to a named (large) artery.
If necessary during vascular assessment, handheld Doppler ultrasonography was used to measure the ankle-brachial index (ABI).
A multidisciplinary approach was used to minimize ischemic time, set treatment priorities, and determine the need for a temporary shunt and allowed for quick and meticulous vascular repair. Tourniquets were removed in the operation room. Antibiotic treatment was started prior to surgery (penicillin 5 million units and gentamicin 80 mg) and carried out for 3 days. After proximal control was achieved, and prior to arterial cross-clamping, intraoperative systemic heparin (5,000 units) was routinely administered, except in cases of excessive bleeding owing to other, nonvascular injuries. Vascular repairs were not left exposed but were covered by a live and intact muscle flap or were routed extra-anatomically outside a massive destructed soft tissue region. Following surgery, patients received a daily subcutaneous dose (40–80 mg) of low-molecular-weight heparin (Clexane) to prevent a thromboembolic event in a nonmobile trauma patient. This was discontinued as the patients became ambulant. If contraindicated, because of bleeding, a temporary inferior vena cava filter was introduced.
Postoperatively, patients were treated in the intensive care unit to allow for repeated operations and débridements of devitalized tissues. Wounds and distal pulses were checked on a daily basis. ABIs were measured for nonpalpable or diminished extremity pulses by handheld Doppler ultrasonography. A 0.2 decrease in ABI led to further vascular imaging by either CTA (Brilliance CT Philips, Cleveland, OH; 64 slices) or angiography (Axiom Artis dBA, Siemens, Munchen, Germany). CTA scans were performed after bolus timing at 1 mm slices. Demonstration of the reconstructed arterial tree was done by various methods, such as volume rendering, maximal intensity projection (MIP), or vessel extraction and master cut.
Follow-up visits after hospital discharge were scheduled every 3 months for the first year after surgery and every 6 months thereafter up to 24 months. These visits included a physical examination and ABI measurements in our outpatient vascular laboratory. A follow-up was conducted by telephone for patients missing their appointments.
Results
During the 33-day war, 511 casualties (only physical injuries) were admitted, of which 39 (7.6%) had sustained a major vascular injury. There were 36 males (92%) and only 3 females (8%), with a mean age of 29 years (range 20–53 years). There were 306 injured soldiers (60% of all injured) and 205 civilians. The incidence of a vascular injury in soldiers was 10.8% (33 of 306). All injuries were penetrating secondary to small arms used in direct combat, high-velocity missiles, and multiple fragments or pellets stored in long-range missiles (Figure 1). All injuries were accompanied by additional insult to soft tissue, bones, and viscera. Each patient suffering a vascular trauma had an average of 2.3 additional injuries. The mean injury severity score was 16 (range 9–35) according to the modified 1997 injury severity score.

Fragments and pellets stored in long-range missiles.
The average time from injury to hospital was 7 hours. Twenty-four percent of the patients were evacuated after more than 10 hours, and 4% were evacuated more than 20 hours after their injury. Complicated urban conflicts interfered with radio control, patient primary treatment, and rescue-hence the extended evacuation times. Each military unit has at least one paramedic and a physician with basic medical equipment. Larger units have specific medical unit assistance that manages the injured patients until transportation. Hemorrhagic shock was the presenting sign in 43% of the patients (17 patients) when first admitted to the ER. Hemorrhagic shock was diagnosed when the systolic blood pressure was lower than 90 mm Hg and the heart rate was greater than 100 beats per minute. The average hemoglobin level was 8.7 g/dL (range 6.7–12.3 g/dL), and hematocrit averaged 25.3% (range 19.5–34%). Thirteen patients (10 soldiers, 3 civilians) with bleeding extremity injuries were admitted to the ER with a tourniquet.
Following resuscitation and primary assessment, 15 patients (38%) were rushed to the operation room, where diagnosis and treatment were done during surgery without using any further imaging modality.
Altogether, CTA was performed in 166 patients (Figure 2) and was positive for a major vascular injury in 24 patients (14.5%). In one additional case, CTA was nonconclusive, and the patient underwent angiography, which demonstrated an intact arterial tree. Vascular injury was diagnosed by CTA by the following findings: extravasation, pseudoaneurysm, segmental loss of opacification, arteriovenous fistula, or abrupt narrowing of the arterial lumen. Patients with a deemed vascular injury were taken to surgery. All 141 patients with negative CTA findings were followed up by the vascular team (normal pulse, normal ABI).
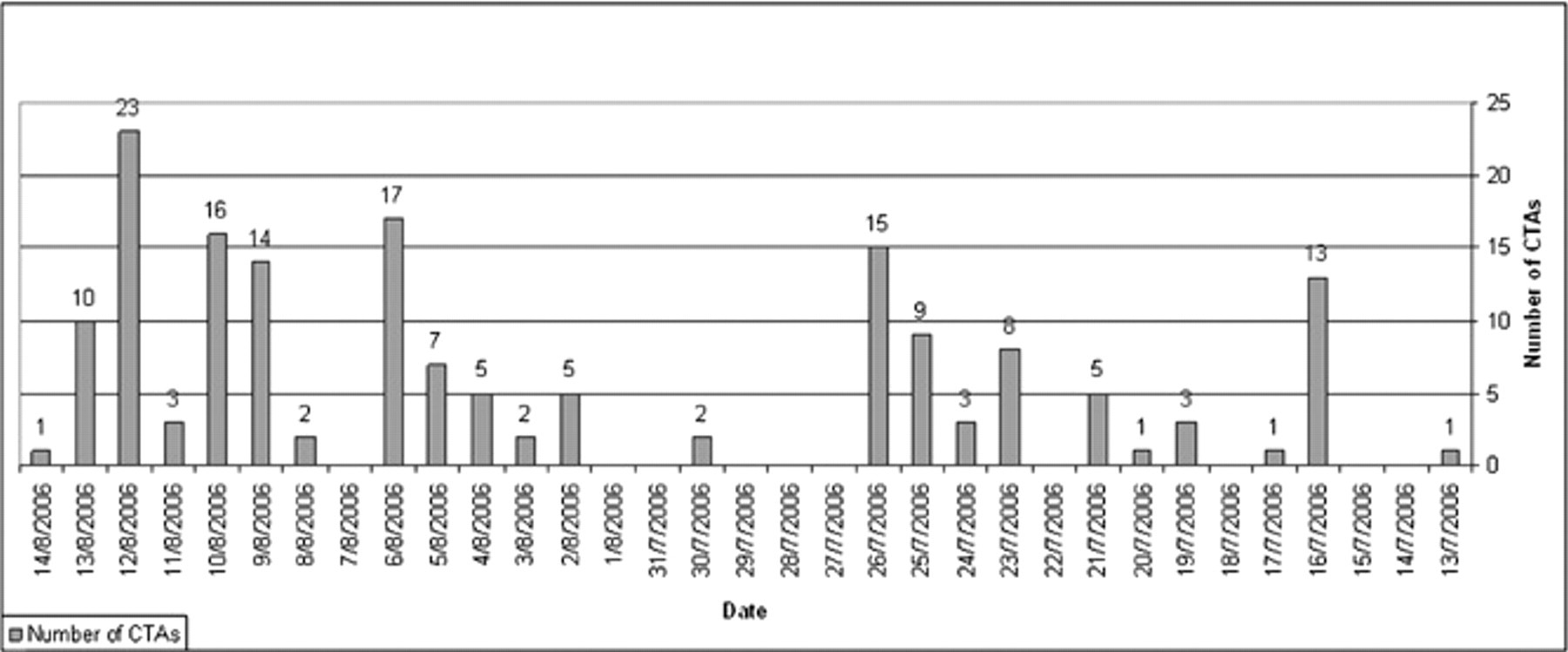
Actual number of computed tomographic angiograms (CTAs) performed during the conflict.
Civilians' vascular injuries were equally divided between the torso and the extremities. In soldiers wearing body armor, the vast majority of vascular injuries were in the extremities (83%), with 17% (5 of 30) torso injuries. The various injured vessels are presented by their anatomic location in Table 1. The arteries of the extremities (upper and lower) were, by far, the most frequently encountered injuries in 28 of 39 patients (72%); lower extremity arteries were injured in 46% of the cases. Almost 80% of the patients with extremity vascular injury had skeletal fractures (22 of 28 patients). Limb ischemia was present in 21 of 28 extremity arterial injuries (75%) and massive bleeding in 7 (25%). Tourniquets were removed only in the operating room, during which time 11 tourniquets (39% of all extremity vascular injuries) were found beneficial. On the other hand, retrospectively, two additional applied tourniquets were unnecessary. Tourniquets are the basic equipment of every medical team, but every soldier also has them. Thus, without the presence of a medical team, soldiers can use tourniquets on their wounded comrades when necessary.
Arterial Injuries by Anatomic Location
Temporary shunts were inserted in 17% of extremity vascular injuries using a Javid shunt or a Silastic tube (for tibial arteries). An additional shunt (Javid) was used during carotid artery repair. Thus, a temporary shunt was used in 15% of the entire cohort. Temporary vascular shunts were used by the vascular team when the definitive treatment had to be delayed and the limb was ischemic.
Injured arteries were repaired by the methods summarized in Table 2. A lateral repair or a patch was done in 6 cases (15%), end-to-end anastomosis was employed in 9 cases (23%), and a venous interposition graft was performed in the majority of cases (15 cases; 38%). Ligation was done in three injuries of a single arm artery (radial or ulnar). Prior to ligation of one arm artery (radial or ulnar), the other artery was checked to be intact by a palpated pulse, Allen test, and normal flow by Doppler ultrasonography. The specific repair used for each injured artery is presented in Table 3. Endovascular technique (Table 4) was employed for the treatment of five cases (13%) and included traumatic arteriovenous fistula of the internal iliac vessels, insertion of a stent graft to the subclavian artery, insertion of a stent, and two embolizations (maxillary artery and superior gluteal artery). No synthetic grafts or patches were used. In addition, 16 large extremity veins were injured, all of which were repaired. Similar to injured arteries, the majority of injured veins were in the extremities (n = 10), followed by 4 in the abdomen and pelvis and 2 in the neck.
Methods of Repair
Method of Specific Repair of Arteries
Endovascular Treatment
Open fasciotomy was liberally done for all cases of combined arterial and venous injury or for ischemia longer than 6 hours. Lower limb fasciotomy was performed in 14 of 18 patients (78%) and was followed later by a skin graft closure.
There were no mortalities and no early amputations in these patients. Their immediate postoperative course was relatively uneventful. Approximately two-thirds of the patients had a second or even up to four operations for débridement of devitalized tissues. There were two cases of thrombosis (5%), one of a patch repair and the other one of an interposition graft. Both were operated on, and a new venous interposition graft was fashioned.
At last follow-up, 30 months postoperatively, one above-knee amputation was performed in a patient with a well-functioning interposition graft for popliteal artery and vein injury. The patient had paresis of his left leg owing to severe sciatic nerve injury. He underwent arthrodesis of the knee joint, but a pus-secreting wound and osteomyelitis necessitated amputation of the limb 23 months after the injury. All end-to-end anastomoses and patch vascular repairs were patent and had a normal flow pattern as assessed by duplex scanning (Diagnostic Ultrasound, Philips, Bothell WA). A mild stenosis was encountered in two venous interposition grafts at the level of the tibial artery and tibioperoneal trunk (distal anastomosis).
Discussion
The incidence of battlefield vascular injuries in older conflicts of the previous century was 0.2 to 4%. 1–4 Recent reports from Iraq have reported 4.8 to 7%, 5,6 and the present study reports 7.6%. The increase in combat-sustained vascular injuries may represent the aggressiveness of modern wars using more devastating weapons or improvement in resuscitation and evacuation.
All injuries reported herein were penetrating secondary to small arms used in direct combat, blast, high-velocity missiles, and multiple fragments or pellets stored in long-range missiles.
Severe vascular injury is manifested by hemorrhage or ischemia and may harbor mortality or limb loss. Bleeding may be external or internal and lead to a hypovolemic shock, which, indeed, was the presenting symptom in 43% of the cases in the present series. Therefore, the surgeon's primary objective, in this setup, is to prevent exsanguination and death; the next objective is to reestablish the vascular supply (revascularization) to prevent amputation.
Better understanding of physiologic derangement in combat-sustained trauma resulted in further advancements in resuscitation, such as permissive hypotension, minimal crystalloid infusion, and early and rapid administration of warmed blood and its products to prevent physiologic deterioration (hypothermia and coagulopathy). Recent modern technologic improvements such as damage control, liberal use of tourniquets, fasciotomies, and temporary shunts enabled better life and limb salvage rates. 7–12
Vascular injuries with a single entry and/or exit wound lead to surgery immediately after the primary assessment and resuscitation in the ER. With multiple injuries, or the presence of only soft signs for a possible vascular injury, imaging is necessary before surgery for both diagnosis and the choice of the preferred treatment.
Computed tomography is routinely performed as part of the trauma patient workup. Intravenous administration of contrast medium, according to study protocol at the same time, provides enhancement of the arterial tree.
Thus, CTA, by virtue of its availability, quick data acquisition, and reconstruction, becomes a major triage tool, and angiography is used for endovascular treatment. CTA was demonstrated to be an accurate and reliable imaging modality in trauma of the carotid arteries in our hands 13 and others'. 6 CTA has a good resolution compared with angiography even for vascular injuries of the extremities, with sensitivity and specificity of 90 to 100%. 14,15 Conceivably CTA may not be diagnostic in the presence of multiple fragmentation casualties of the extremities owing to metal artifacts. We were able to avoid these problems and demonstrate the reconstructed arterial tree by various methods, such as volume rendering and MIP or vessel extraction and master cut. Figure 3 demonstrates such a case in which accurate diagnosis of a vascular injury was made despite the presence of multiple fragments by using a volume rendering technique and related slice and MIP. In the present cohort, CTA was performed in 166 patients (see Figure 2), of whom 24 patients (14.5%) were accurately diagnosed with a major vascular injury. In 141 patients, CTA was able to exclude a vascular injury, and our follow-up did not reveal any missed injury. In one additional case, CTA was nonconclusive, and the patient underwent angiography, which demonstrated an intact arterial tree. This was the only case in which angiography was used for diagnosis in the present study.

Computed tomographic angiography volume rendering reconstruction with related slice showing the injured left superficial femoral artery. Intact vascular tree of the right leg despite multiple shrapnel fragments.
Angiography, which is considered the gold standard for diagnosing vascular injuries, 7,8 is problematic, with multiple levels of extremity and fragmentation injuries. During wartime, the number of simultaneously admitted patients in need of vascular assessment is above and beyond the handling capability of invasive radiology teams and available angiography suites. Angiography is not feasible with mass casualties also because it is time consuming. During wartime, the number, arrival times, and severity of injuries of future patients are unknown; therefore, quick assessment should be performed to allow readiness for the next wave of patients. During the Lebanon war, there were 6 days with waves of 10 to 23 wounded patients waiting for imaging (see Figure 2). Finally, angiography demonstrates only the vessel lumen (actually luminography), whereas CTA depicts not only the lumen but also the vessel wall and surrounding tissues. A massive injury of the surrounding tissues may play a role in the management of vascular repair (ie, the need for an extra-anatomic bypass).
A missed vascular injury (when the outer damage is not severe or overt) will present itself later as an arteriovenous fistula or a pseudoaneurysm. 16 Figure 4 demonstrates a possible injury to be missed that was depicted by CTA, which was employed owing to the proximity of a major artery.
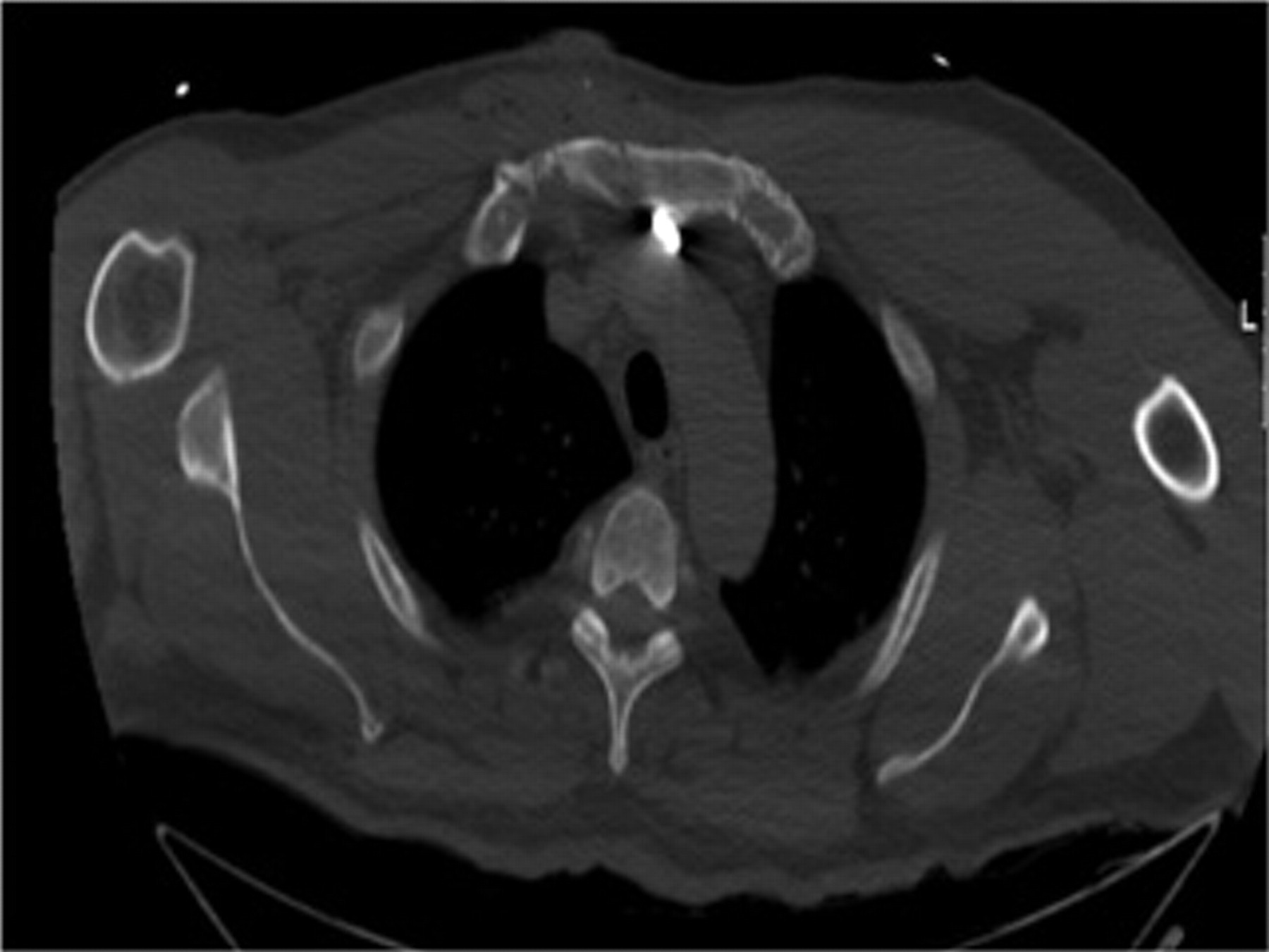
Injury of the innominate artery by a fragment that might have been missed without computed tomographic angiography.
Civilians are not equipped with body armor, and their vascular injuries were equally divided between the torso and the extremities. In soldiers wearing body armor, the vast majority of vascular injuries were in the extremities (83%), with 17% (5 of 30) torso injuries. Soldiers are therefore somewhat protected from severe and fatal torso injuries, a finding that was reported by Peck and colleagues. 17
Owing to body armor, the extremities are more vulnerable; therefore, vascular injuries of the extremities comprise approximately 60 to 90% of all injuries in other studies 1–3,5–8 and 72% in the present study. Exsanguination from extremity wounds is still the leading cause of preventable death in combat-sustained injuries. The reported perioperative mortality in vascular casualties during the war in Afghanistan and Iraq was 4.3%. 6 There were no perioperative mortalities in the present series, although severe injuries and hypovolemic shock as the presenting signs occurred in 43% of the patients. The anatomic distribution of vascular injuries of our patients (see Table 1) was similar to that of previously reported series.
During World War II, when there were long evacuation times and poor physiologic and equipment conditions prevented arterial reconstruction, ligation was the accepted treatment, 1 resulting in an approximately 60% amputation rate. This amputation rate was dramatically reduced with arterial reconstruction to 13% during the Korean War 2 and 12% in Vietnam. 3 The above-mentioned advancements in assessment and treatment were employed in recent wars. Thus, in recent reports from Afghanistan and Iraq, the early amputation rates were improved to 4.2 to 9%. 5,6,11
Eger and colleagues were among the first reports in the modern era to describe the use of temporary intravascular shunts for arterial vascular injuries. 18 A recent report had described a decade's experience with temporary shunts in 60 patients, with a 5% thrombosis rate. 19 In the present series, with quick and meticulous treatment, contemplated priorities and multidisciplinary approach temporary shunts were employed in 17% and fasciotomies were performed in 78% of the patients with extremity injuries. The indication for a temporary vascular shunt in our series was the need for the vascular team to await an orthopedic procedure, as in the case of an unstable fracture or a necessary shortening of long bones. Although our experience is a lot smaller, none of the shunts inserted were thrombosed or dislodged at the time of definitive repair (1–5 hours after insertion). The experience of the present study is that the use of temporary shunts is effective and decreases the ischemic time while the patient is treated for other, higher-priority injuries. A temporary shunt is especially prudent when treating patients with severe fractures (ie, Gustilo IIIc fractures) and when bone shortening is necessary.
The described management resulted in 0% mortality and a 0% amputation rate in the early postoperative period (only one amputation after 23 months). In the Lebanon war of 1982, with 87 patients over 3 months, we had 1% mortality and a 2% amputation rate. At that time, patients benefited from the very short evacuation periods and quick arrival at a vascular facility (90 minutes), similar to those reported from Iraq. In sharp contrast, during the Lebanon war of 2006, owing to urban combat settings that interfere with radio control and injured identification, treatment and evacuation times were extended to 7 hours. No temporary shunts were used in 1982.
Large extremity vein injuries usually accompany those of the adjacent arteries. Although their repair, especially when a complex venous reconstruction is needed, is controversial, mostly because there is no danger for life or limb loss, we believe that large injured veins should be repaired. Reconstructions of all large named veins were performed in the present cohort and have been reported on separately. 20
Seemingly, casualties are complex, with multiple fragmentations resulting in systemic effects; therefore, today we are treating patients who would never have made it to care previously. The approach should be multidisciplinary to set treatment priorities and the needed repeated procedures for débridement of devitalized tissues. Vascular repairs should never be left uncovered by a vital and healthy tissue even if a rotational flap is needed because of infection and rupture. Intensive care monitoring for at least 24 hours is prudent.
The described management observation that 13% of vascular injuries in this experience were treated with endovascular techniques is significant because although the vast majority of combat vascular injuries require open surgery, there seems to be a subset that should be treated with less invasive endovascular methods. This is specifically important with very high carotid, aortic arch, great vessel, and pelvic vascular injuries, as noted by others. 21
In conclusion, the triage team should have a high index of suspicion for a vascular injury. A liberal use of CTA should be practiced to allow for early and accurate diagnosis of a vascular injury, even in the presence of multiple pellets and/or fragments. CTA, not angiography, should be the first-line modality for the diagnosis of vascular injuries, especially when dealing with mass casualties. Angiography should be reserved for endovascular treatment, not for diagnosis alone.
When needed, endovascular techniques are effective for certain wartime vascular injuries in a subset of patients.
Temporary shunts are effective and should be inserted when the definitive vascular repair should be postponed.
Aggressive, fast (repeated if needed), and meticulous treatment by a multidisciplinary team leads to greater life and limb salvage.
Footnotes
Acknowledgment
Financial disclosure of authors and reviewers: None reported.
Presented at the 15th Annual Advanced Interventional Management Symposium, November 14–16, 2007, New York, NY.