
Abstract
This study analyzed the clinical outcome in endovascular aneurysm repair (EVAR) patients with an angulated aortic neck. Two hundred thirty-eight EVAR patients underwent postoperative duplex ultrasonography and/or computed tomographic angiography, which was repeated every 6 to 12 months. Aortic neck angle was classified into < 45° (A1, n= 129), ≥ 45 to < 60° (A2, n = 43), and ≥ 60° (A3, n = 42). The perioperative complication rates for groups A1, A2, and A3 were 13%, 5%, and 29%, respectively (p = .006). Proximal type I early endoleaks occurred in 9%, 33%, and 38% in groups A1, A2, and A3, respectively (p < .0001). Intraoperative proximal aortic cuffs were needed in 7%, 28%, and 33% in groups A1, A2, and A3, respectively (p < .0001). However, the rate of late reintervention was comparable in all groups. Postoperatively, the size of abdominal aortic aneurysm decreased or remained unchanged in 97%, 95%, and 84% in A1, A2, and A3, respectively (p = .0147). The rates of freedom from late type I endoleak at 1, 2, and 3 years were 90%, 85%, and 85% for A1; 74%, 74%, and 68% for A2; and 64%, 64%, and 53% for A3 (p = .0013). EVAR can be used for patients with an angulated aortic neck but was associated with a higher rate of early and late type I endoleaks and early interventions.
The suitability for endovascular aneurysm repair (EVAR), based on the instructions for use (IFU), requires a specific infrarenal aortic angulation. The recommended infrarenal neck angulation is < 45° for Talent stent grafts and < 60° for all other EVAR stent grafts. Although adherence to the IFU specific for each stent graft results in low complication rates, deviation from the recommended IFU may lead to higher mortality and morbidity. 1 Recently, the envelope to treat abdominal aortic aneurysms (AAAs) using EVAR has been pushed beyond the IFU; hence, in the United States, a significant number of patients with AAAs are being treated by EVAR.
Our present study analyzed the clinical outcome of EVAR in patients with an angulated aortic neck.
Patient Population and Methods
This study, which was approved by our Institutional Review Board, analyzed only 238 (of 523) patients that were operated on by two of our full-time academic faculty (A.F.A. and P.A.S.) between 2000 and 2008. Patients that were operated on by nonacademic physicians were excluded because we had no control over their follow-up. Patients who lacked preoperative infrarenal aortic neck measurements (because of the lack of good-quality computed tomography [CT]) were also excluded.
Prospectively collected data were supplemented with a retrospective review of medical records and radiologic images. The preoperative workup of these patients included color duplex ultrasonography, computed tomographic angiography (CTA), and arteriography, and these were used to select patients for endovascular therapy. Preoperative cardiac evaluations were done only in patients with a history of significant coronary artery disease and/or congestive heart failure. Preoperative arteriograms were obtained in all patients using a marked pigtail catheter. The demographic and clinical characteristic profiles, aortic neck anatomic characteristics, operative details, and events were recorded.
The Food and Drug Administration–approved device selection was based on physician preference. All procedures were performed under either epidural or general anesthesia, based on the physician's choice, using conventional fluoroscopy (General Electric Medical, Milwaukee, WI) originally. All devices were inserted, and patients were followed according to the manufacturers' recommendations. Every effort was made to deploy the endovascular device flush with the level of the lowest renal artery. However, over the last few years, we became more liberal in using EVAR beyond the IFU in patients with angulated or short aortic necks.
All patients were encouraged to participate in our postoperative surveillance protocol, which included CTA and/or color duplex ultrasonography and plain abdominal radiography at 1, 6, and 12 months and then every 12 months thereafter.
Standard CT follow-up protocol with and without intravenous contrast material was used, which required CT section thickness of 3 mm. The proximal aortic neck diameter was recorded in the minor access from adventitia to adventitia, just below the lowest renal artery. Another measurement was also made 15 mm below the lowest renal artery, or at the distal end of the aortic neck, in patients with a short neck (< 15 mm). The aortic neck angle was calculated. This angle was measured between the aortic neck and the longitudinal axis of the aneurysm, as seen on CT scanning or using preoperative arteriography, if the preoperative CT scan was not helpful. The infrarenal aortic neck length was measured on CTA as the distance between the lowest renal artery and the point of the initial aneurysm dilatation or where the infrarenal aortic diameter increased to greater than 3 mm of the proximal neck diameter. The aneurysmal sac size was defined as the maximum transverse diameter and was also measured from adventitia to adventitia. Details of these measurements, specifically the neck anatomy, were reviewed separately without the knowledge of the early and late clinical outcomes of these patients.
Comparison of Preoperative AAA Largest Minor Access Diameter to the Postoperative Diameter at the Last Follow-Up
Pretreatment images were used to measure AAA stability or shrinkage, as recommended by the Ad Hoc Committee for the Standardized Reporting Practice in Vascular Surgery. 2,3 Significant AAA diameter change was defined as ≥ 5 mm, and shrinkage was defined as ≤ 5 mm. Migration of the endograft was determined by measuring the distance from the lowest renal artery and the most cephalad portion of the stent graft, as seen on CTA images. Significant migration was defined as displacement of ≥ 10 mm from the predischarge study, or any displacement requiring secondary intervention.
An angulated neck was defined as a ≥ 45° angle. For clinical applications and statistical analysis, the aortic neck angle in our study was classified into < 45° (A1), ≥ 45° to < 60° (A2), and ≥ 60° (A3) angles.
Endoleak was determined using CT, based on extravasation of contrast between the prosthesis and the aneurysm wall, and/or by color duplex ultrasonography where the flow and spectral signals were outside the prosthesis. If the CT and duplex ultrasonography results differed, contrast arteriography was done to confirm the endoleak. Primary or early endoleak was defined as a leak detected within 30 days of the procedure, and a secondary or late endoleak was defined as a leak observed after 30 days postoperatively.
The primary end points for analysis for this study included early (30 days postoperative) outcome, specifically the incidence of early proximal aortic endoleak (type I), use of proximal aortic neck extension or cuff, other secondary interventions, technical success, and surgical conversion. Technical success was defined from the periprocedural period through the first 24-hour postoperative period. Secondary early outcome included operative blood loss, transfusion requirement, volume of contrast used during implantation, stent graft patency, other endoleaks (distal types I, II, III, and IV), and other perioperative morbidity and/or mortality. Late clinical outcomes included type I endoleak, other types of endoleak, stent graft patency, aortic sac expansion, conversion to open repair, stent graft migration, aneurysm rupture, secondary interventions, and aneurysm-related mortality.
Statistical Methods
Comparisons between the groups were performed using contingency table analysis with a chi-square or Fisher exact test (categorical variables) and t-tests (continuous variables) to determine statistically significant differences. Logistic regression was used to predict which risk factors were associated with early/late intervention and early/late endoleak. The Kaplan-Meier method was used to estimate survival distributions (survival, freedom from late endoleak, freedom from late intervention, and EVAR patency) for the groups. The test statistic for comparison between these two survival distributions was based on the log-rank test. An alpha level of ≤ .05 was used to determine statistical significance.
Results
Two hundred thirty-eight patients who underwent EVAR were analyzed, including 49 patients with Ancure (Guidant Corp, Indianapolis, IN), 47 patients with AneuRx (Medtronic, Santa Rosa, CA), 104 patients with Excluder (W. L. Gore & Assoc., Flagstaff, AZ), and 38 patients with Zenith devices (Cook Corp., Indianapolis, IN). The mean follow-up was 25 months (range 1–87 months). The overall initial technical success rate was 99%. All AneuRx, Excluder, and Zenith devices were successfully deployed, but two patients with the Ancure device failed, one secondary to failure of introduction for the original model of the Ancure device, which was converted to an AneuRx device in the same procedure, and the other one owing to iliac artery obstruction/rupture; the patient underwent an open repair.
The demographic and clinical characteristics according to neck angle are summarized in Table 1. As noted, these characteristics were somewhat similar, except for male gender and mean age.
Demographics and Clinical Characteristics by Neck Angle
NS = not significant.
Table 2 summarizes aortic neck angle and AAA characteristics. As noted, patients with an angle of ≥ 60° had statistically significantly larger AAAs, both preoperatively and postoperatively. Postoperatively, the size of the AAA decreased or remained unchanged in 97%, 95%, and 84% in A1, A2, and A3 patients, respectively (p = .0147).
Abdominal Aortic Aneurysm Characteristics by Neck Angle
AAA = abdominal aortic aneurysm; NS = not significant.
Table 3 summarizes the correlation of aortic neck angle and intraoperative/hospital variables. As noted, the mean fluoroscopy time, mean amount of contrast, and mean transfusion were statistically significantly greater in patients with an angle > 60° (p < .0001).
Intraoperative and Hospital Variables by Neck Angle
NS = not significant.
The overall perioperative complications are summarized in Table 4. Graft limb thrombosis/acute limb ischemia (14%) and hematoma/bleeding (10%) were higher in patients with an angle of > 60° (p = .0071 and < .0001, respectively). The overall complication rate was also statistically significantly higher in these patients (29%; p = .0061; see Table 4).
Perioperative Complications by Neck Angle
NS = not significant.
There were no significant differences in overall perioperative complications in patients with angulated necks (> 60°) between various devices (18% for Excluder, 33% for AneuRx, 33% for Ancure, and 45% for Cook; p = .3089).
Inpatient mortality was statistically higher in patients with a neck angle > 60° (10%; p = .0001). There were four perioperative deaths, three secondary to myocardial infarction and one secondary to multisystem failure.
Table 5 summarizes the correlation of neck angle and the incidence of endoleak and intervention.
Endoleak and Intervention by Neck Angle
NS = not significant.
*These early type I endoleaks were noted prior to completion of the procedure, and most were treated with proximal aortic cuffs (see Results).
Early type I endoleaks (38%; p < .001) and all early endoleaks (48%; p = .0019) were statistically significantly higher in patients with an angle > 60°. These early type I endoleaks were noted in the circulatory dynamics laboratory prior to completion of the procedure, and most were treated with proximal aortic cuffs. Aortic cuff extensions were also used more often to seal early type I endoleaks in patients with an angle > 60° (33%; p < .0001). Late type I endoleaks and all late endoleaks were also statistically significantly higher in patients with an angle > 60°.
Neck Angle and Fate of Early Endoleak and Type of Early Intervention
As noted in Table 5, the endoleaks of 14 of 16 patients with A3 neck anatomy (with early type I endoleak) sealed by inserting a proximal aortic cuff extension, except in 4 patients who needed Palmaz stents. In the remaining two patients, the type I endoleak decreased with no significant change in the aortic sac size. There were also 14 patients with an A2 neck who had type I early endoleak on completion angiogram. Eleven of these patients were treated with proximal aortic cuff extensions and the endoleak sealed immediately, and one was treated with aortic cuff extensions, which decreased the endoleak, and it sealed 6 months later. Thirteen patients with A1 neck anatomy had type I early endoleaks. Eleven of these patients were treated with proximal aortic cuff extensions and all endoleaks sealed immediately. Of the remaining two patients, the endoleak sealed in one at 3 months and in one at 12 months with no significant change in the AAA sac size.
Fifteen patients with A1 neck anatomy had type II endoleaks, 10 of which sealed spontaneously within 30 days; 1 sealed at 3 months, 1 at 16 months, and 1 at 46 months postoperatively. The two remaining patients had persistent type II endoleaks, one at 12 months and one at 36 months, with no significant change in the AAA sac size. One patient with A2 neck anatomy had an early type II endoleak, which sealed 6 months later.
Overall, there were 18 A3 patients, 12 A2 patients, and 17 A1 patients with early 30-day perioperative intervention. Thirty-seven of these were proximal aortic extensions to seal type I proximal endoleaks. The remaining early interventions included two groin explorations for bleeding, two lysis/percutaneous transluminal angioplasty (PTA) procedures, four thrombectomies, and two stent grafts for treatment of iliac rupture in patients with Ancure devices.
Neck Angle/Late Midterm Clinical Outcome: Late Endoleak, Intervention, Survival, and EVAR Patency
Neck Angle/Late Endoleak
The rates of freedom from late endoleaks at 1, 2, and 3 years were 90%, 85%, and 85% for A1 patients; 74%, 74%, and 68% for A2 patients; and 64%, 64%, and 53% for A3 patients, respectively (p = .013; Figure 1).
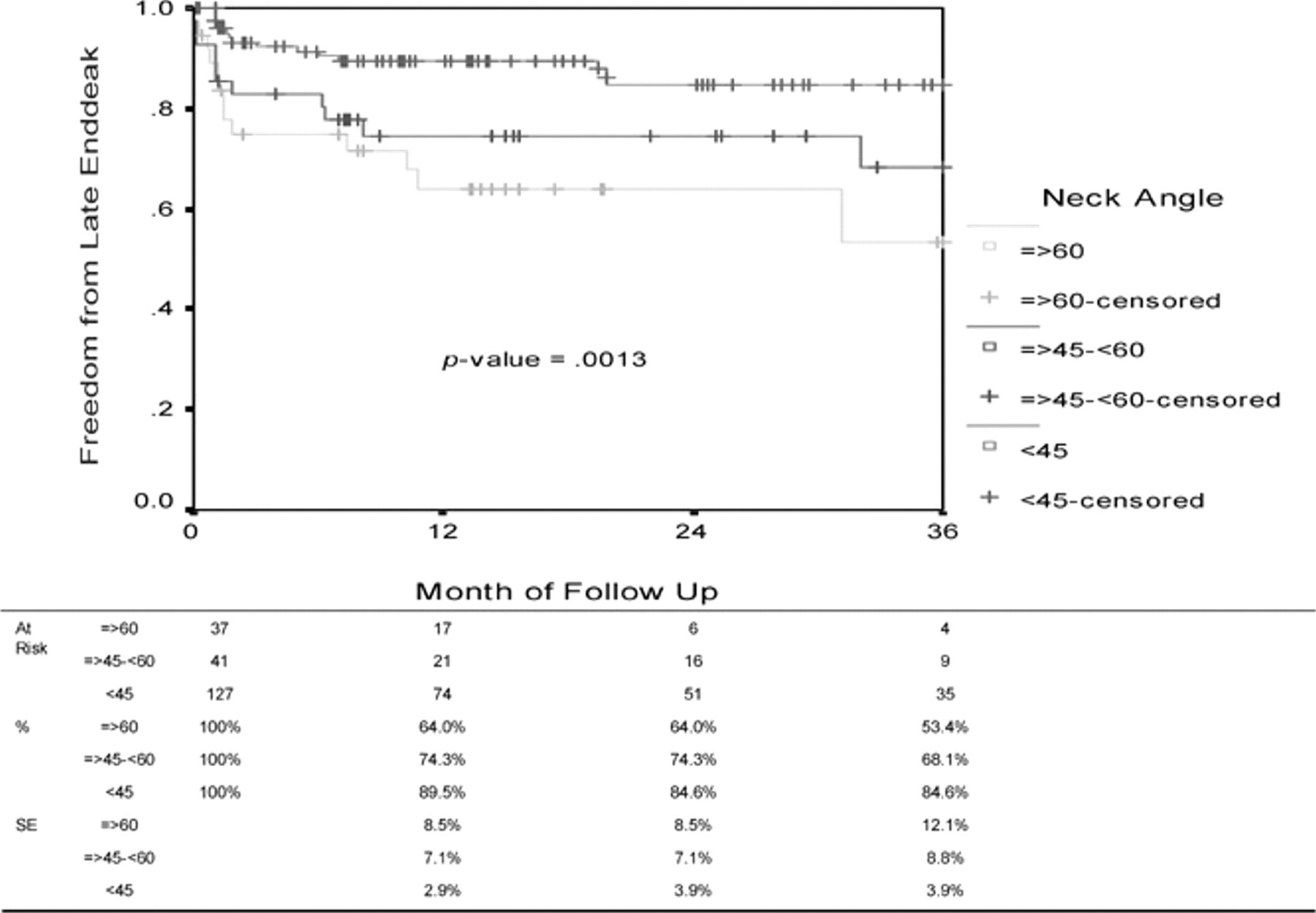
Freedom from late endoleaks according to neck angle at 1, 2, and 3 years.
Neck Angle/Late Intervention
The rates of freedom from late intervention at 1, 2, and 3 years were 96%, 93%, and 93% for A1 patients; 93%, 88%, and 88% for A2 patients; and 97%, 97%, and 86% for A3 patients, respectively (p = .9271; Figure 2).

Late intervention according to neck angle at 1, 2, and 3 years.
Neck Angle/Survival Rates
The survival rates at 1, 2, and 3 years were 93%, 90%, and 88% for A1 patients; 81%, 70%, and 60% for A2 patients; and 76%, 62%, and 55% for A3 patients, respectively (p = .0012; Figure 3). Only one of the late deaths was related to AAA rupture.

Survival rates according to neck angle at 1, 2, and 3 years.
Neck Angle/EVAR Patency
EVAR patency rates for A1, A2, and A3 patients at 1, 2, and 3 years were 98%, 94%, and 93%; 94%, 94%, and 94%; and 91%, 91%, and 91%, respectively (p = .6420; Figure 4).

EVAR patency according to neck angle at 1, 2, and 3 years.
Overall, 13 EVAR procedures failed, 8 of them perioperatively and 5 at a later date. Five were Zenith, four were Ancure, three were Excluder, and one was an AneuRx device. Patients with perioperative graft thrombosis were successfully treated with thrombectomy and/or lysis with PTA/stenting, except for three patients, for whom femorofemoral bypass grafting was needed. In the remaining five grafts, one Ancure graft failed at 1 month and was successfully treated with PTA/stenting and lysis; one Zenith graft failed at 12 months owing to an infected graft, which was removed, and the patient expired 1 month later from multiple system failure. Another Zenith graft failed 7 months later, and the patient was treated with a femorofemoral bypass graft. Two other Zenith grafts failed at 8 and 12 months later, with no further treatment (the patients were asymptomatic).
Discussion
It is generally recommended that an infrarenal neck angle < 45° be used to secure proximal graft fixation for EVAR. In severely angulated aortic necks, the endograft is curved, which results in a larger force exerted at the outer wall; thus, the blood flow will produce a larger displacement force. The endograft is usually held in its proximal position by friction dependent on the radial force of the graft against the aneurysmal wall and the contact surface between the graft and the aortic wall. 4 The length of the proximal attachment in patients with short angulated necks will decrease, leading to a smaller contact surface and lower friction forces. Therefore, stent graft migration may occur if displacement forces exceed the friction forces. 4
Our study demonstrated an increased fluoroscopic time, mean amount of contrast used during the procedure, and mean amount of transfusion required in patients with increased neck angulation. Fairman and colleagues also evaluated if complicated neck anatomy (short [< 15 mm], very short [< 10 mm], dilated [> 28 mm], angulated [≥ 45°], calcified, and thrombus lined) impacted blood loss, transfusion requirements, and volume of contrast required for EVAR. 5 They reported no significant difference in the procedural variables of transfusion required or the volume of contrast used; however, an important difference between the two studies is that they combined six distinct neck features to describe a complicated neck.
Our study also demonstrated a significantly increased incidence of graft limb thrombosis/acute limb ischemia and hematoma/bleeding perioperative complications with increasing neck angulation, especially when > 60°. As the procedure complexity increases, and if more devices have to be advanced through the common femoral and iliac systems, there is an increased risk of damage to the access arteries, which can lead to thrombosis. Perioperative death was also significantly increased with increasing neck angulation in our study. However, other studies have not shown an increased risk of perioperative mortality with hostile neck anatomy. 5,6 The difference in outcomes could be secondary to the fact that these studies included other anatomic criteria for the classification of a “hostile neck,” whereas our study focused only on neck angulation. One landmark study reported the outcomes of EVAR with neck angulation from the EUROSTAR registry. 4 Hobo and colleagues found an increased risk of perioperative mortality in the presence of an angulated neck (> 60°); however, it did not reach statistical significance (4% vs 2.9%). 4
The most clear difference with increasing neck angulation, when compared to favorable neck angle in our series, was the incidence of type I early endoleaks. Thirty-eight percent of patients with neck angulation > 60° had type I early endoleaks. Most of these required intraoperative placement of aortic cuffs; however, a few patients also required proximal aortic Palmaz stents to seal proximal type I early endoleaks. Others treated patients with hostile neck anatomy using adjunctive balloon-expandable stents. 7 Cox and colleagues treated 19 patients, in whom proximal balloon-expandable stents (17 were Cordis/Palmaz stents) were used in patients with hostile neck anatomy, including an angulated neck ≥ 60°. 7
Increased neck angulation was also associated with significantly increased rates of late type I endoleaks, although this did not correlate with a significant increase in late reintervention. Sternbergh and colleagues, using the AneuRx device, concluded that patients with an increasing degree of neck angulation had a higher incidence of adverse outcomes, including endoleak, migration, conversion to open repair, and death. 8 Fulton and colleagues, also using the AneuRx endograft, concluded that patients with unfavorable neck anatomy had a significantly higher rate of migration, device-related complications, and secondary intervention rates. 9 Hobo and colleagues also found that severe neck angulation (> 60°) predicted early and late type I endoleaks. 4 Secondary interventions, associated with repair of proximal endoleaks, were more frequently performed in patients with severe aortic neck angulation. Although proximal endoleak was strongly associated with rupture of AAA, the incidence of rupture was too low to reveal any significant association with severe aortic neck angulation in the entire study group. 10
Other studies have not found a significant difference in patients treated with EVAR with hostile neck anatomy versus “good” neck anatomy in regard to early and late type I endoleaks. 6,11 Robbins and colleagues, using the Talent device with suprarenal fixation, concluded that increased aortic neck angulation was not associated with the selected adverse outcome within 1 year following EVAR. 12 Again, it is likely that the differences in these study results, when compared to ours, were that multiple anatomic factors were included to define a hostile neck.
There was no correlation between EVAR patency and neck angulation in our series. Similar results were also noted by Fairman and colleagues, who concluded that the primary graft limb patency was 100%, regardless of the neck anatomy. 5
Recently, some manufacturers have adapted their products so that angulated necks can be better used, that is, by designing specific stent grafts with larger areas of fabric without stent frames.
Our present study has several limitations, including the heterogeneity of devices used for EVAR; for example, the Ancure device is no longer available on the market and was not a modular device. We also included devices with and without suprarenal fixation in our study, which may affect the outcome with hostile neck anatomy. 12 Another limitation was that device selection for each case was not randomized and that there was likely preference for certain devices with hostile neck anatomy and preference for other devices with good neck anatomy. The number of patients with angulated necks was also relatively small. Other aortic neck features were not analyzed in this study.
In conclusion, although there was an increase in both early and late type I endoleaks in patients with highly angulated necks, there was no increased need for late intervention-only an increased need for early placement of aortic cuffs or early intervention. However, there was an increased rate of perioperative complications/mortality with angulated neck anatomy, which has to be weighed when making the decision to undergo open repair versus endovascular repair.
Footnotes
Acknowledgment
Financial disclosure of authors and reviewers: None reported.