
Abstract
Open surgery remains the gold standard by which endovascular treatment of superficial chronic venous insufficiency is measured. This meta-analysis of randomized controlled trials reviews the current evidence base, comparing open and endovascular treatment of varicose veins. Systematic review of studies reporting duplex scan follow-up after open surgical, laser (endovenous laser therapy [EVLT]), or radiofrequency (VNUS Closure device, VNUS Medical Technologies, San Jose, CA) treatment of refluxing great saphenous veins was completed. Primary outcome measures were occlusion and complication rates and time taken to resume work. No significant difference in recurrence rates at 3 months between open surgery and EVLT (RR 2.19, 95% CI 0.99–4.85, p = .05) or VNUS device (RR 7.57; 95% CI 0.42–136.02) were found. Return to work is significantly faster following VNUS (by 8.24 days; 95% CI 10.50–5.97) or EVLT (by 5.02 days; 95% CI 6.52–3.52). Endovascular treatment of varicose veins is safe and effective and offers the significant advantage of rapid recovery.
Varicose veins (VVs) significantly reduce quality of life, whereas their operative treatment demonstrably improves quality of life. 1,2 This, in conjunction with their prevalence, accounts for the fact that 90,000 VV operations are performed annually in the United Kingdom, making them the most commonly performed day-surgical procedure. 3
Open surgical saphenofemoral junction (SFJ) ligation combined with stripping of the great saphenous vein (GSV) above the knee and phlebectomy of incompetent tributaries remains the highest volume “gold standard” procedure. 4–7 Endovascular techniques are now well established; they have considerable advantages in recovery rate, operative time, postoperative pain, and bruising and offer the possibility of avoiding general anesthesia. 8,9 High patient satisfaction fuels demand and is giving rise to an increasing volume of endovenous practice. 10–12
Both endovenous laser therapy (EVLT) and radiofrequency ablation (RFA) thermally ablate the target vein, obviating the need for groin dissection, with its associated morbidity. The additional cost of endovascular catheters and equipment per treated leg remains in the region of £300 for both techniques. Duplex ultrasound availability and training are also required; however, overall economic costs are offset by a rapid return to work, and the cost per limb is reduced when patients have multiple vessel reflux. 13–15
Recurrence of VVs postoperatively remains a significant problem of the open technique. Recently, a published long-term follow-up from the above-cited trial found that of 133 operated legs, 83 had developed clinically recurrent VVs by 11 years (a recurrence rate of 62%). 16 Much of this recurrence has been attributed to neovascularization at the SFJ, a phenomenon rarely encountered with endovascular ablation. 9,17,18
To justify their increasing use, endovascular techniques must prove their clinical noninferiority and cost-effectiveness. 8 Here we collate and present the published data from randomized controlled trials (RCTs) and case series comparing the efficacy of open operation with laser and RFA for the treatment of primary superficial venous reflux of the GSV.
Methods
Search Strategy
Three principal electronic databases were searched, in addition to bibliographies of well-known vascular publications. The Cochrane clinical trial database was interrogated using the search term “varicose vein*,” yielding 520 RCTs, which were reviewed manually (Figure 1). Medline (1950–April 2009) and Embase (1980–April 2009) searches were performed using the terms “exp Saphenous Vein or exp Varicose Veins” and “clinical trial.mp. or clinical trial.pt. or random.mp. or tu.xs. or (randomized controlled trial or randomized or placebo or randomised controlled trial or randomized).mp,” yielding 5,388 and 2,960 results, respectively.

QUORUM diagram (occlusion data). EVLT = endovenous laser therapy; RCT = randomized controlled trial; RFA = radiofrequency ablation.
Inclusion Criteria
The title and abstract of all identified articles were screened for inclusion criteria by a single reviewer. RCTs directly comparing open and endovascular treatment of GSV VVs were selected for meta-analysis. Studies without duplex follow-up or adequate technical information were excluded, as were non–English-language publications and those not relating to GSV ablation. In addition, all treatment series of open or endovascular series reporting duplex scan occlusion data, complication rates, and time taken to return to work were selected for pooled analysis.
Statistical Analysis
A meta-analysis of RCTs comparing open and endovascular treatment of GSV VVs was completed using RevMan statistical software (The Cochrane Centre, Copenhagen, Denmark), generating an aggregate relative risk (RR) with 95% confidence intervals (CIs) for the stated primary end points. Further statistical comparisons of pooled data (occlusion and complication rates from treatment series) were performed using SPSS (SPSS Inc, Chicago, IL).
Data for common and potential serious complications were pooled, and rates were calculated. Statistical significance was evaluated using a 3 × 2 Fisher exact test for all three groups, and where justified, complication rates of EVLT and RFA were compared using a two-tailed chi-square test with Yates correction.
Results
Studies Identified
Nine RCTs were included in the meta-analysis of occlusion rates (see Figure 1). Of these, six compared EVLT and three compared a VNUS Closure device (VNUS Medical Technologies, San Jose, CA) with open surgery. In addition, duplex scan follow-up data and complication rates from 87 studies (20,278 legs), in which GSV VVs were treated by open surgery, EVLT, or RFA, were pooled and analyzed (Appendix 1, Appendix 2, and Appendix 3).
Twenty-four studies (3,000 legs) with duplex ultrasound follow-up following open surgical treatment of GSV VVs were identified. Data from small RCTs have the briefest follow-up time (up to 3 years) but are useful for direct and contemporaneous comparison with endovascular treatment modalities. 8,19 Longer cohort studies follow the course of this operation over 10- (prospective) and 30- (retrospective) year periods, finding recurrence rates of 62% and 60%, respectively, much of this owing to SFJ neovascularization (type 1c recurrence). 16,20
Twenty-nine studies (4,064 legs) reported duplex ultrasound data following GSV RFA. One RCT relates to the restore catheter, which aimed to restore competence rather than ablate the vein. Given its 40% failure rate, it was soon discontinued in favor of the Closure device. The data from the restore arm of the trial are indicated as a discarded outlier on the pooled RFA results at 1 week. The Closure catheter has since been superseded by the ClosureFAST; however, this is not substantially reflected in the literature, and only two articles relate to this latest catheter.
Fifty-five studies (13,214 legs) report duplex ultrasound data following GSV EVLT. The majority of studies used 810 and 980 nm lasers, with one using 1,064 nm (252 legs) and three small series (123 legs) using 1,320 nm lasers. A number of large 810 nm series, with 1 to 3 years of follow-up, have been published recently, notably by the Italian Endovenous-Laser Working Group, Fernandez and colleagues, and Lu and colleagues, demonstrating occlusion rates of 98.6% and 91.2% at 1 year and 97% at 3 years, respectively. 21–23 Desmyttere and colleagues and Myers and Jolley have published large series with 4-year follow-up data. 24,25
Efficacy
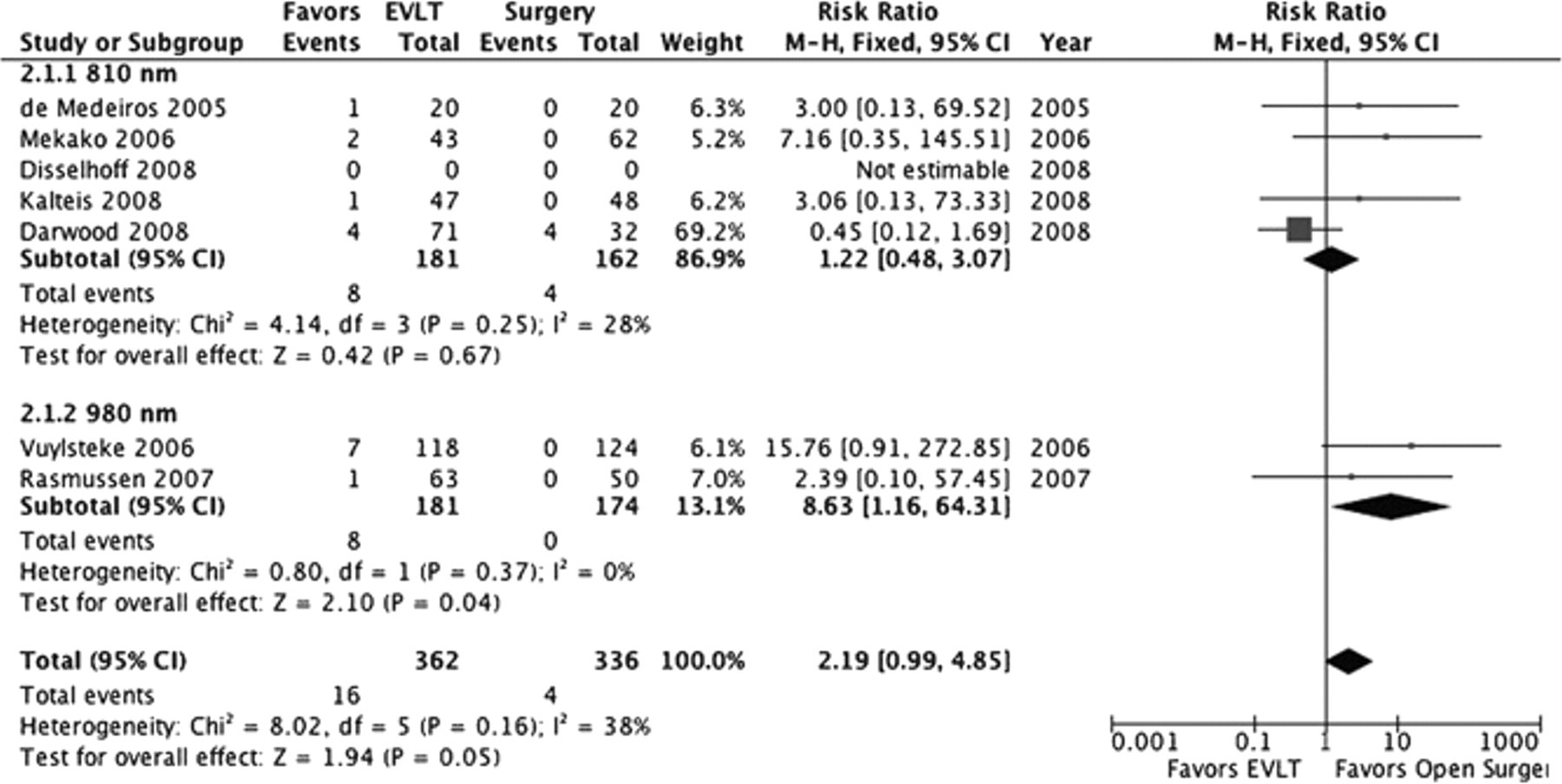
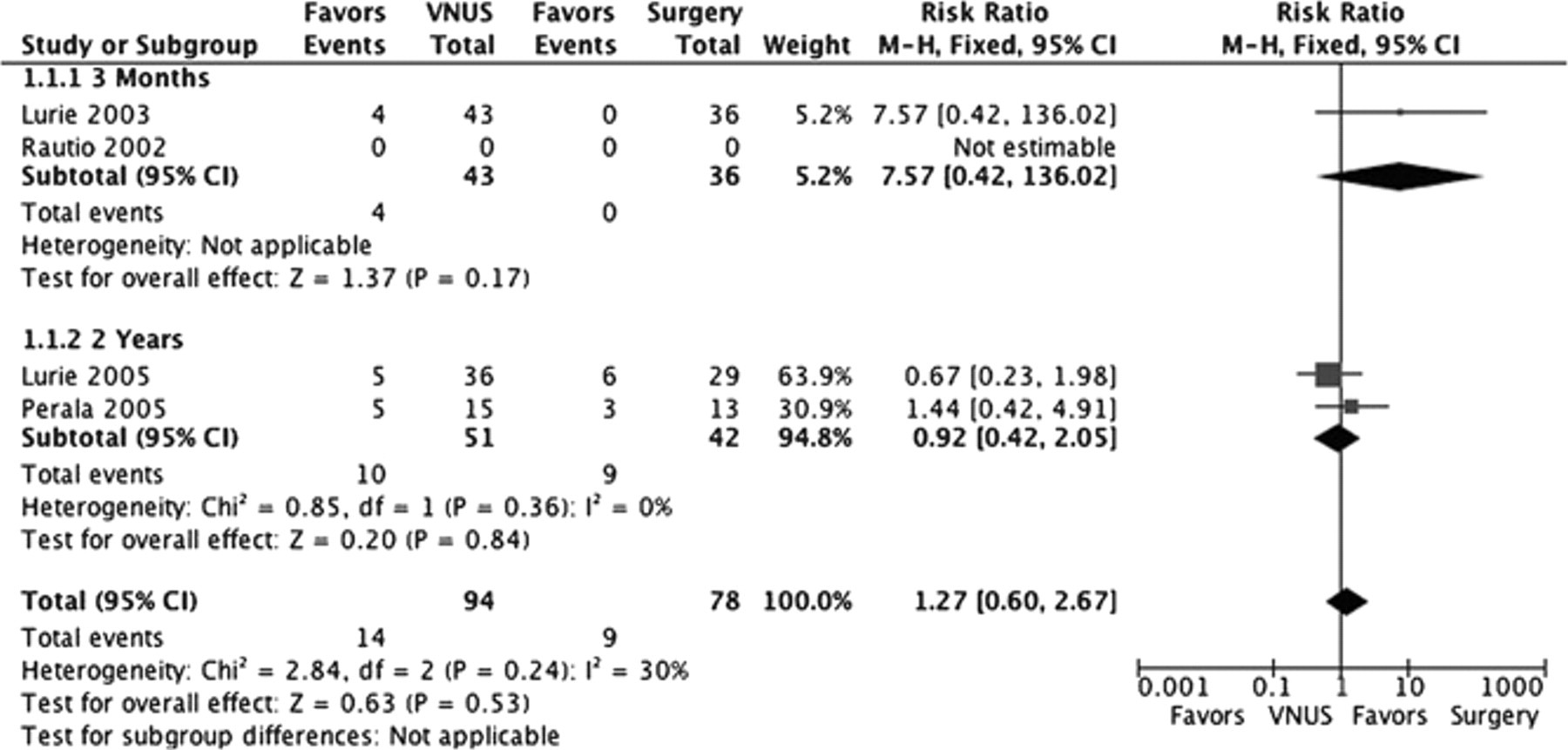
The meta-analysis found no significant difference in recurrence rates at 3 months between open surgery and EVLT (RR 2.19, 95% CI 0.99–4.85) or VNUS Closure (RR 7.57, 95% CI 0.42–136.02). There was no difference in recurrence rate between VNUS Closure and open surgery at 2 years (RR 0.92, 95% CI 0.42–2.05) (Figure 2 and Figure 3).
Pooled Gsv Occlusion Data from Published Series
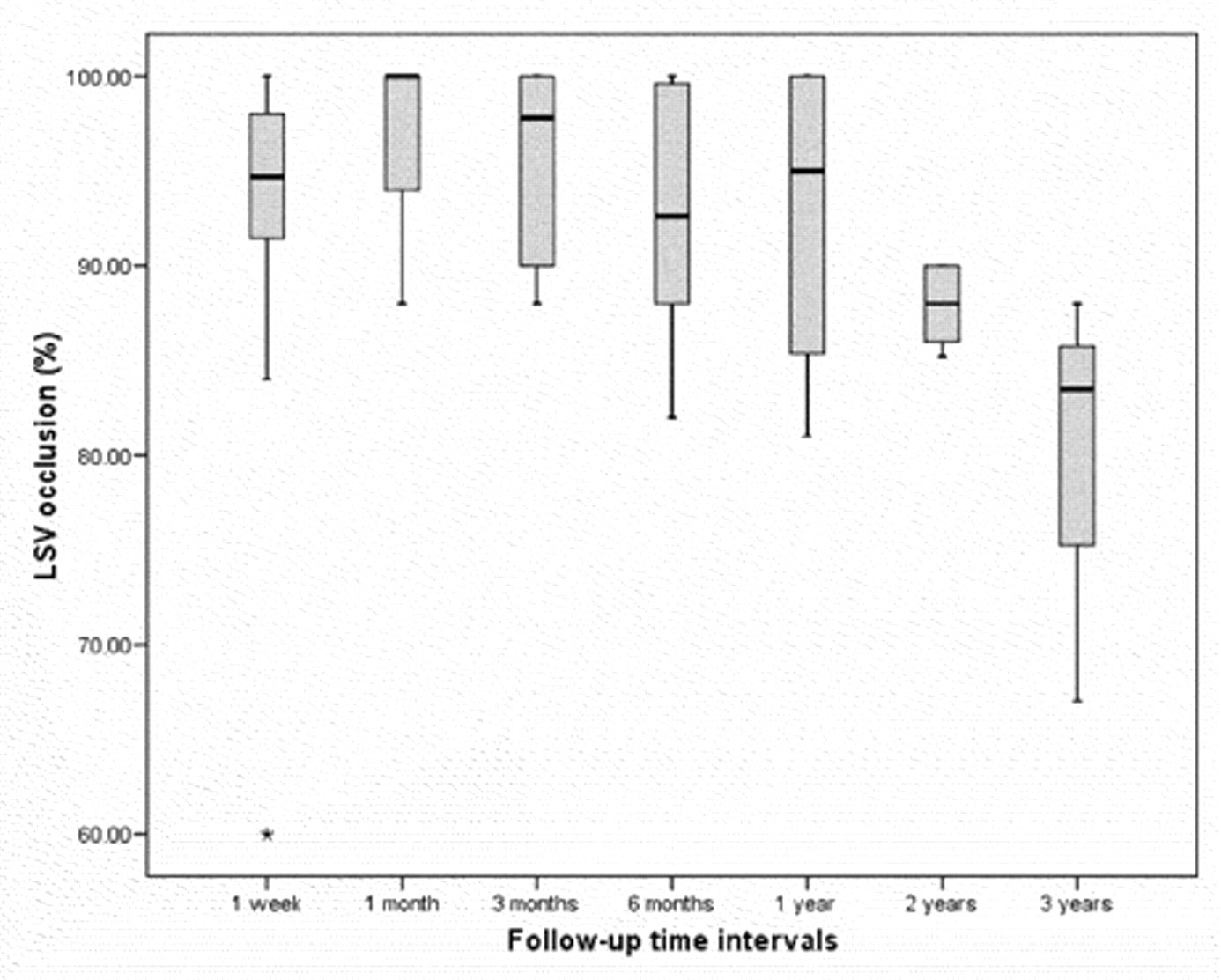
Figure 4, Figure 5, and Figure 6 depict pooled recurrence rate data for GSVs treated by open surgery, RFA, and EVLT. At 2 years, the occlusion rate for the VNUS device is comparable to that of open surgery at 87.9 (95% CI 85.8–90.0%), whereas that of EVLT (all frequencies and energies) remains 91.5% (95% CI 85.9–97%). EVLT maintains durability better in comparison to RFA. Although open surgical recurrence rates are extremely high at 10 years and beyond, there are no sufficient data to confirm the long-term durability of endovascular techniques.
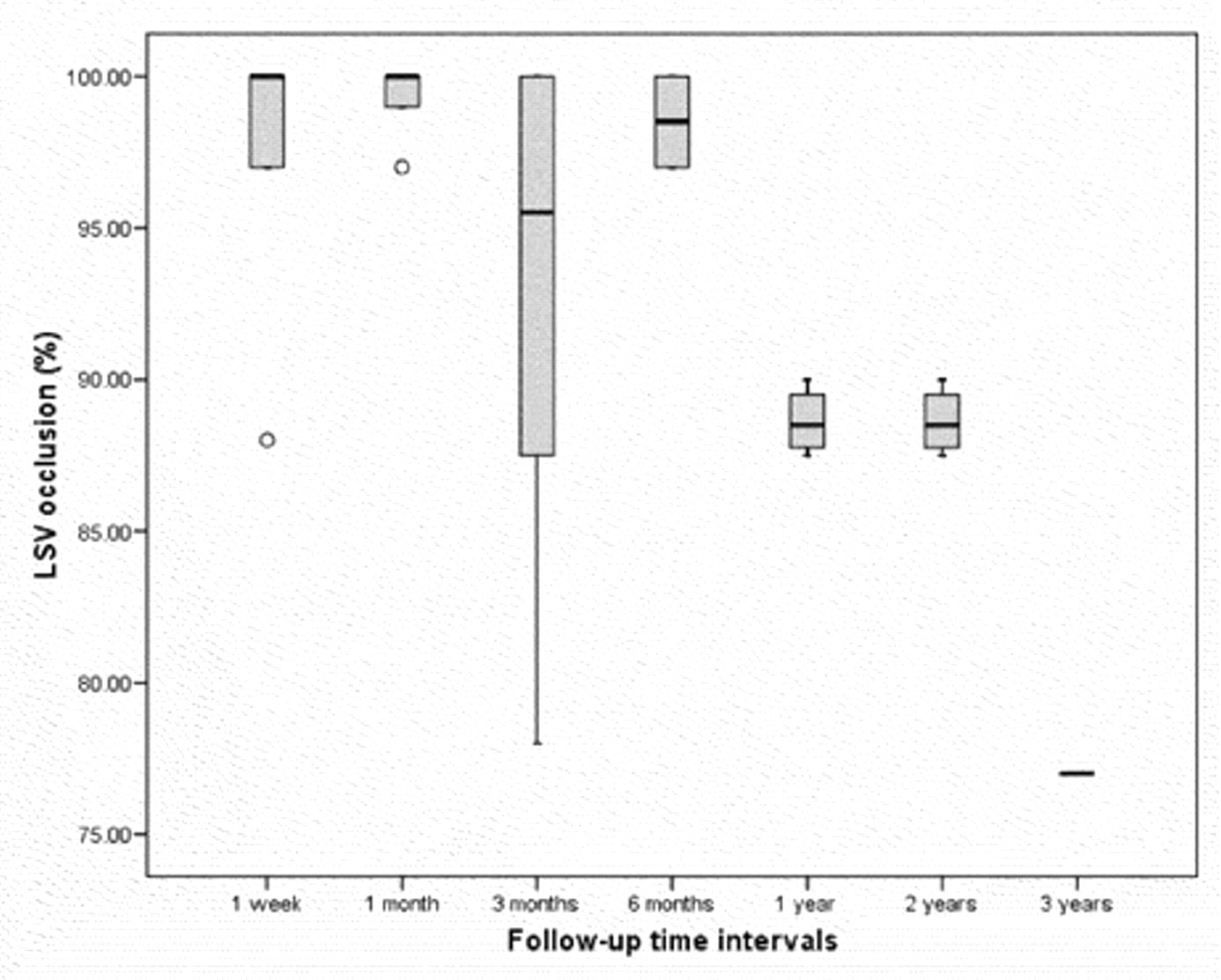
Open surgery: combined long (great) saphenous vein (LSV) occlusion rates.
Radiofrequency ablation: combined long (great) saphenous vein (LSV) occlusion rates.
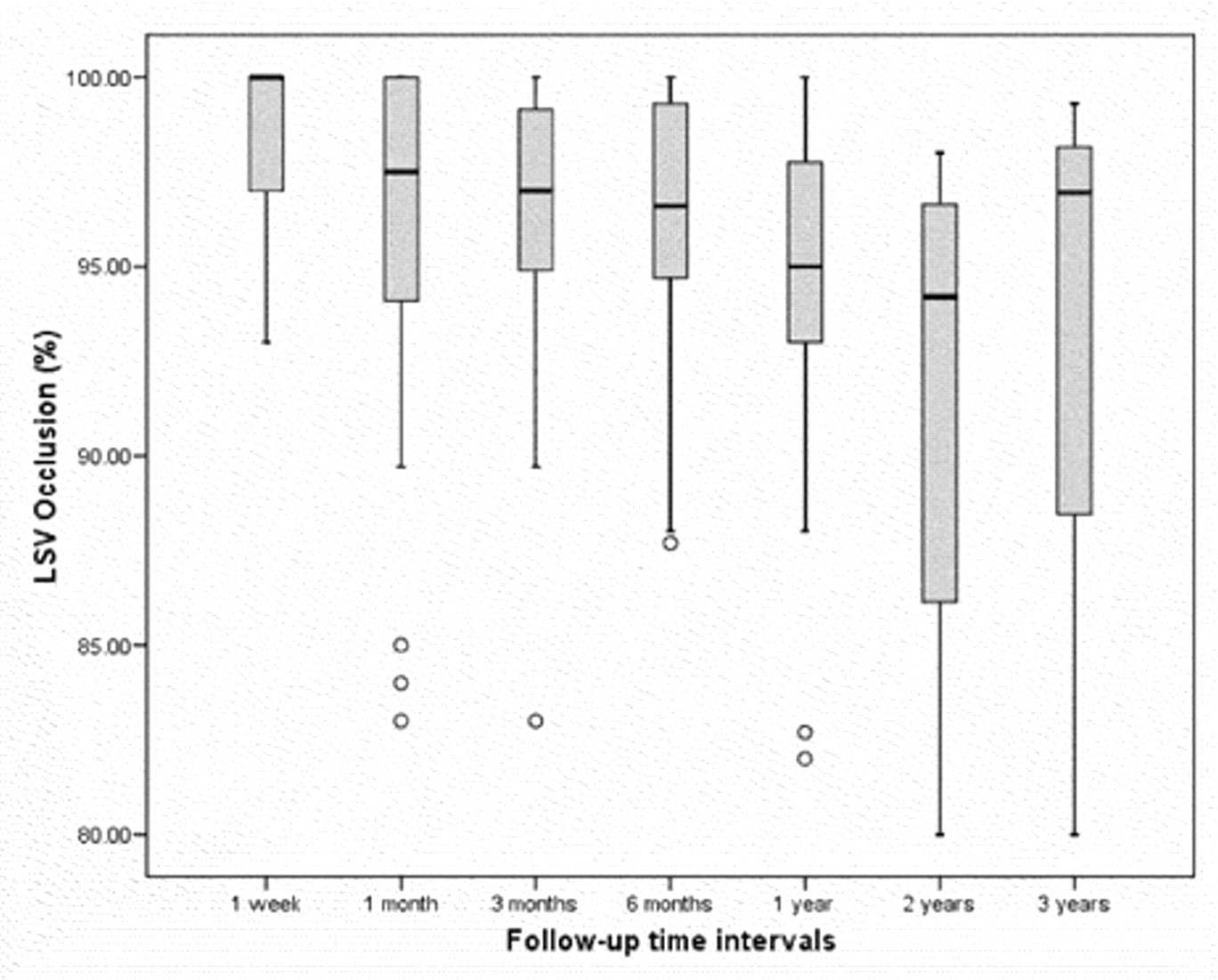
Endovenous laser therapy: combined long (great) saphenous vein (LSV) occlusion rates.
Subgroup Analysis: Linear Endovenous Energy Density
One-year recurrence data from published RCTs and series using an EVLT protocol delivering more than 60 J/cm were compared to those delivering a lower energy. In the former group (linear endovenous energy density [LEED] > 60 J/cm), 46 GSVs recanalized of 2,405 legs at risk (98.1% occlusion rate). In the latter, 74 GSVs recanalized by 1 year of 1,542 legs at risk (95.2% occlusion rate). This gives a small but significantly increased risk of recanalization with low energy dosage (RR 1.03, 95% CI 1.017–1.043, p < .0001).
Return to Work
When compared to open surgical treatment, return to work is significantly faster following the VNUS Closure device (−8.24 days, 95% CI −10.50 to −5.97) and EVLT (−5.02 days, 95% CI −6.52 to −3.52). Of the four RCTs reporting time taken to return to work, only Rasmussen and colleagues reported no significant advantage from endovascular treatment (Figure 7). 14

Safety: Complication Data
Pooling the published data suggests a significantly lower incidence of thromboembolism among patients treated endovascularly, but patients treated with RFA experience significantly greater incidence of deep venous thrombosis (DVT) (1.3 vs 0.2%, p = .0001), paresthesia (10.5 vs 4%, p = .0001), and skin burns (1.1 vs 0.5%, p = .0043) than those treated with EVLT.
The incidence of wound infection is significantly (p < .0001) higher with open surgery (0.1%; 6 of 1,186) compared to endovascular ablation (0.04% overall; 4 of 11,272), whereas skin burns are an issue only with endovascular treatment (0% of the open group reported skin burns compared to 1.1% of the RFA group and 0.5% of the EVLT group). Rates of wound infection, thrombophlebitis, and hematoma do not differ significantly between patients treated with EVLT and RFA.
Discussion
Endovascular techniques are demonstrably safe. Occlusion rates following endovascular GSV ablation are high, with early results being comparable (at 3 months EVLT and VNUS studies demonstrate 96% occlusion and open studies 93%) and midterm results being superior to open surgery (EVLT attaining 93% but open surgery achieving just 77% GSV occlusion at 3 years). The heterogeneity of the data remains a problem in establishing definitive recurrence and complication rates for all treatment modalities.
Studies vary in their follow-up protocols, and most report significant loss to follow-up, such that the pooled population studied at each of the time periods diminishes sharply. The studied RFA population consisted of 2,540 legs at 1 week, diminishing to 1,116, 673, 316, 119, and 117 patients at 1 to 5 years, respectively. Likewise, the pooled EVLT population was 5,568 legs at 1 week, decreasing to 3,947, 690, and 1,554 at 1 to 3 years, and just 45 legs from two studies were scanned at 4 years.
The great majority of GSV recanalization following endovenous treatment occurs within a year postprocedurally. 26,27 This probably represents delayed technical failure, namely, inadequate energy transferred to the venous endothelium to cause the usually observed progressive venous atrophy. 27,28 Appropriate energy dosing and scrupulous operative technique, ensuring adequate contact between the catheter tip and the vein wall, have improved results, and occlusion rates approaching 100% are reported in recent studies. 24,29–31
Endovenous Laser Therapy
The success of EVLT has been shown to be energy dependent. Primary nonocclusion and early reopening of the GSV are seen more frequently when the LEED is less than 70 to 80 J/cm or, factoring vein diameter into the equation, when the endovenous fluence equivalent (EFE) is less than 20 J/cm 2 . 22,32–37 This fits with our understanding that 810 to 940 nm laser energy is transferred to the venous endothelium indirectly by means of steam bubbles whose volume, and therefore the surface area of vein treated, is directly proportional to the energy delivered. 38
Disselhoff and colleagues found, in a series of 93 EVLT patients followed up over a 2-year period, that all technical failures and three-quarters of treatment failures occurred in the first half of the cohort, indicating a learning curve (p < .015), and that operative time also diminishes with experience. 34
Placing the patient in the Trendelenburg position during the procedure empties the GSV and facilitates energy transmission to the vein wall rather than absorption by blood. When the latter occurs, early occlusion with thrombus may resolve and recanalize, leading to technical failure, as well as excessive pain and thrombophlebitis. 23,32 Failure to wear prescribed compression stockings for a minimum of 2 weeks after surgery has also been associated with an increased recurrence rate. 39
RCTs comparing continuous and stepwise withdrawal favor the former (Darwood and colleagues, 810 nm, 8 and Disselhoff and colleagues, 810 nm 40 ), although Proebstle and colleagues failed to reproduce this finding in a very small group of 25 stepwise versus 15 continuous cases using a 940 nm laser. 41 Kabnick found 810 and 980 nm devices to be essentially equivalent in outcome. 42
Fernandez and colleagues, analyzing their registry of almost 2,000 EVLT procedures, found body mass index > 30 kg/m 2 and a vein diameter > 8.5 mm to be the only factors predictive of recanalization, given equivalent energy dosing. 22,37 The latter result was reproduced independently by Desmyttere and colleagues and Gonzalez-Zeh and colleagues, who found that increasing GSV diameter was associated with failure of both foam sclerotherapy (odds ratio 1.68, 95% CI 1.24–2.27, p < .0008) and EVLT (odds ratio 1.91, 95% CI 1.02–3.59, p = .0428). 24,43 Gonzalez-Zeh and colleagues reported 90% treatment success using foam sclerotherapy for veins < 6.5 mm and laser for veins < 12 mm. 43
Radiofrequency Ablation
The majority of published articles describing RFA relate to the VNUS Closure device. The radiofrequency generator for this device (regulated by a feedback loop to keep a constant temperature of 85°C at the catheter tip) did not allow in vivo measurement of energy delivery. The new VNUS ClosureFAST catheter, which uses a 7 cm catheter tip to deliver radiofrequency energy, does allow accurate energy measurement and reduces operative time.
In 2008, Proebstle and colleagues reported their use of VNUS ClosureFAST in a series of 252 legs. 29 Treatment temperature was raised to 120°C, delivering an average LEED of 116.2 J/cm along the proximal 7 cm vein segment, 2 cm distal to the SFJ (which was treated twice), and 68.2 J/cm along the remainder of the vein. The EFE calculated from the same data set at 3 cm distal to the SFJ was as high as 82 ± 25 J/cm 2 . Occlusion rates over 6 months using this protocol were 99.6%.
The EVOLVeS study (using the VNUS Closure device) demonstrated significant clinical improvement and significantly reduced postprocedural pain (compared to open surgery) at all follow-up points to 2 years. 44 Its recurrence rate was marginally lower than that of open surgery (14 vs 20% at 2 years), with significantly reduced neovascularization (type 1c recurrence) in the endovascular arm.
Logistic regression analysis finds catheter pullback speed (p < .0001) and body mass index (p < .0333) to be risk factors for anatomic failure. 45 The VNUS pullback speed is inversely proportional to and essentially an indirect measurement of LEED. In contrast to EVLT, however, vein diameter does not affect clinical or ultrasound-assessed outcome, as shown by Nicolini's series of 330 GSVs treated by the VNUS Closure, with a mean preoperative vein diameter of 7.7 mm (3–17.4 mm). 46
Is Adjunctive SFJ Ligation Necessary?
SFJ ligation has been described as an adjunctive procedure for both EVLT and VNUS Closure device. 47,48 It was considered desirable both to increase GSV occlusion rates and prevent thrombus extension into the deep femoral vein with the associated risk of pulmonary embolism. 49
The absolute risk of DVT and pulmonary embolism is small, however, and not significantly altered by performing adjunctive SFJ ligation-nor is thromboembolic risk related to proximal GSV diameter. 50
Avoiding groin dissection (with its consequent inflammatory reaction, promoting neovascularization) and leaving the SFJ intact allow anatomic drainage of proximal GSV tributaries and reduce recurrence rates. 51,52 The majority of vascular specialists have now discarded the practice of adjunctive SFJ ligation in favor of a purely endovascular technique of GSV ablation, commencing just distal to the epigastric vein to avoid proximal thrombus extension. 53,54
Extent of Ablation, Avulsions, and Anesthetic
Readily available duplex imaging has enabled selective treatment of refluxing veins while leaving functioning veins intact. Phlebectomy may not be routinely indicated. Once axial reflux is treated and venous hypertension abolished, varices diminish in size and clinical significance. 46 Morphologic studies have shown that in two-thirds of patients with GSV reflux, disease is limited to the thigh and just below the knee, but reflux extending beyond this should be treated. 55
Most study protocols ablate the GSV above the knee, with few routinely treating the GSV below the knee. When patients have reflux throughout the whole length of the GSV, extending EVLT from the groin to the midcalf (rather than limiting it to above the knee) is effective in reducing the need for concomitant ambulatory phlebectomy or sclerotherapy for residual veins to as little as 17%, without increasing the risk of saphenous nerve injury. 31
Complications
The most serious complications associated with VV surgery, other than bleeding, are thromboembolic. The incidence of DVT after traditional open VV surgery is quoted in the literature to be as high as 5%. Principal risk factors are family history, age, and severity of venous disease (greatest with CEAP class 5 and 6, ie, ulcer patients, probably owing to their poor mobility and increased inflammatory state). Low-molecular-weight heparin thromboprophylaxis does not significantly alter the incidence. 56
Our analysis (Table 1) shows both EVLT and the VNUS Closure device to be safe, with a comparable and extremely low risk of pulmonary embolism and significantly lower risk of DVT than open surgery (0.3% for EVLT and 1.2% for the VNUS device compared to 1.8% open surgery; p = .0001).
Complication Rates (%)
DVT = deep venous thrombosis; EVLT = endovenous laser therapy; PE = pulmonary embolism; RFA = radiofrequency ablation.
Overall comparison of three groups (A, B, and C) using a 3 × 2 Fisher exact test; analyses of RFA versus EVLT (groups B and C) using a chi-square test with Yates correction.
Pain and bruising are diminished by endovascular treatment, reflected in a rapid return to normal activity and work. Anecdotally, RFA is considered less painful than EVLT. This may be explained by the focused nature of the laser, which produces local temperatures in excess of 1,000°C, causing histologically detectable vein perforations. 28,38,57,58
VNUS Medical Technologies has sponsored the only published RCT comparing EVLT and RFA (VNUS ClosureFAST). 30 This study reported significantly less pain and bruising during the first 2 postprocedural weeks among the VNUS cohort, with no difference in pain at a month. Improvement in global quality of life was also significantly improved with the VNUS device at 1 and 2 weeks but was similar at 1 month. Return to work or normal activity was not reported. Eighty-seven patients were enrolled in the trial and followed for 1 month. The study was thus not designed or powered to find differences in safety and efficacy but was tailored to look at those aspects of the VNUS device that are thought to be marginally superior.
The Endovascular Varicose Vein VNUS versus EVLT RCT (or EVVERT study, ISRCTN 63135694) is a single-center study under way at St George's Vascular Institute (London, UK). It is independent of corporate sponsorship and seeks to enroll 200 patients with primary GSV VVs and randomize them to receive EVLT (810 nm, Varilase Bright-tip, Vascular Solutions Inc., Minneapolis, MN) or RFA (VNUS ClosureFAST). The study is powered to detect differences in occlusion rate under carefully standardized conditions and as such should provide valuable information regarding the relative efficacy of these two techniques.
The incidence of phlebitis increases with venous diameter and may occur more often with the 810 nm than with the 980 nm laser. 42 However, Lu and colleagues reported a total absence of thrombophlebitis in their series of over 1,100 patients treated by 810 nm laser. 23 They stressed the importance of using intraoperative limb elevation and stocking compression to limit this complication.
Return to Work
The meta-analysis of RCTs confirmed significantly faster recovery rates of endovascular ablation compared to conventional VV surgery by 8.24 days following the VNUS device (95% CI 10.50–5.97) and 5.02 days after EVLT (95% CI 6.52–3.52). 14 Shorter recovery rates are decisive in significantly decreasing overall economic cost; however, patients' subjective interpretations of pain and of readiness to return to work are multifactorial and remain difficult to evaluate objectively. 13
Conclusion
Endovascular treatment of VVs is safe, and short- to medium-term efficacy is at least equivalent to that of open surgery. Pooled data demonstrate that the 2-year occlusion rate for the VNUS device is comparable to that of open surgery at 87.9% (95% CI 85.8–90.0), whereas it is 91.5% (95% CI 85.9–97) for EVLT (pooling all frequencies and energies). The latest catheters and protocols offer substantial improvements over these results.
RFA has marginally higher recanalization rates than EVLT, but the heterogeneity of reported data and the fact that few studies relate to the new VNUS ClosureFAST RFA catheter render this finding open to question.
The heterogeneous nature of published data shows the need for well-designed RCTs in this field of surgery to accurately evaluate differences in recanalization and complication rates between the latest EVLT and VNUS catheters, under rigorously standardized conditions. Accurate information regarding postoperative pain and bruising and the time taken to return to work by patients undergoing these two increasingly used endovascular treatment modalities would be of benefit to the vascular specialist and inform patient choice.
Acknowledgment
R. Brar was awarded a research fellowship by the Royal College of Surgeons of England.
Financial disclosure of reviewers: None reported.
Footnotes
Open Surgery EVLT = endovenous laser therapy; GSV = great saphenous vein; no=no duplex; NRCT = non randomized controlled trial; RCT = randomized controlled trial; RFA = radiofrequency ablation. *Complication data. Radiofrequency Ablation GSV = great saphenous vein; NRCT = non randomized controlled trial; RCT = randomized controlled trial. *Complication data. Endovenous Laser Therapy GSV = great saphenous vein; IEWG = Italian Endovenous-Laser Working Group; NRCT = non randomized controlled trial; RCT = randomized controlled trial; RFA = radiofrequency ablation. *Complication data.
†High-energy protocol.
Lead Author
Year
Study Design
Center
Legs (GSV)
Longest Duplex Follow-Up (mo)
Allegra
65
2007
Series
Single
862
60
Belcaro
66
2000
RCT vs foam
Multi
42
120
Bountouroglou*
67
2006
RCT vs foam
Single
30
3
Darwood
8
2008
RCT vs EVLT
Single
32
3
De Maeseneer
68
2005
Series
Single
100
12
De Medeiros*
59
2005
RCT vs EVLT
Single
20
1
Disselhoff*
9
2008
RCT vs EVLT
Single
60
0
Dwerryhouse
6
1999
RCT (strip/ligate)
Single
52
60
Fischer
20
2001
Series
Single
125
408
Frings*
69
2004
Series
Single
500
24
Hinchliffe*
19
2006
RCT vs RFA
Single
16
12
Kalteis*
61
2008
RCT vs EVLT
Single
48
3
Kianifard*
18
2006
NRCT vs RFA
Single
55
12
Lurie*
63
2003
RCT vs RFA
Multi
36
3
Lurie
44
2005
RCT vs RFA
Multi
36
24
Mekako
60
2006
NRCT vs EVLT
Single
62
3
Perala*
64
2005
RCT vs RFA
Single
13
36
Rasmussen*
14
2007
RCT vs EVLT
Single
68
6
Rautio*
13
2002
RCT vs RFA
Multi
13
0
Sarin
7
1994
RCT (strip/ligate)
Single
43
24
Smith
70
2002
RCT (duplex/no)
Single
189
12
Van Rij*
56
2004
Series
Single
377
0
Vuylsteke*
71
2006
RCT vs EVLT
Single
124
6
Winterborn
16
2004
RCT (strip/ligate)
Single
133
120
Lead Author
Year
Study Design
Center
Legs (GSV)
Duplex Follow-Up (mo)
Device
Almedia*
30
2009
RCT
Multi
46
1
ClosureFAST
Almedia
72
2006
Series
Single
128
-
Closure
Boros*
52
2008
Series
Single
77
0.25
Closure
Boros*
52
2009
Series
Single
142
0.25
Closure
Chandler*
47
2000
Series
Multi
301
3
Closure
Fassiadis*
73
2002
Series
Single
18
12
Closure
Fassiadis
51
2002
Series
Single
127
12
Closure
Goldman*
19,74
2000
Series
Single
12
0
Closure
Hinchliffe*
19
2006
RCT
Single
16
12
Closure
Hingorani*
53
2004
Series
Single
73
0.25
Closure
Kianifard
18
2006
NRCT
Single
55
12
Closure
Labropolous*
75
2006
Prospective series
Single
46
0.25
Closure
Lurie*
63
2003
RCT
Multi
44
3
Closure
Lurie
44
2005
RCT
Multi
44
24
Closure
Manfrini*
76
2000
RCT
Multi
152
6
Closure
Manfrini
2000
RCT
Multi
68
0.25
Restore
Marston
77
2006
NRCT
Single
58
1
Closure
Merchant*
78
2002
Series
Multi
319
24
Closure
Merchant*
45,79
2005
Series
Multi
1,154
60
Closure
Nicolini*
46
2005
Series
Multi
330
36
Closure
Ogawa*
80
2005
Series
Single
25
1
Closure
Perala*
64
2005
RCT
Single
15
36
Closure
Pichot
17
2003
Series
Multi
63
24
Closure
Proebstle*
29
2008
Series
Multi
252
6
ClosureFAST
Puggioni*
81
2005
Series
Single
130
0.25
Closure
Rautio*
13
2002
RCT
Multi
15
0
Closure
Ravi
82
2006
Series
Single
159
0.25
Closure
Salles-Cunha
83
2004
Series
Single
106
6
Closure
Sybrandy*
84
2002
Series
Single
26
6
Closure
Weiss*
85
2002
Series
Single
140
24
Closure
Lead Author
Year
Study Design
Center
Legs (GSV)
Duplex Follow-Up (mo)
Wavelength (nm)
Agus (IEWG)*
21
2006
Series
Multi
1,076
36
810–980
Almedia†
72
2006
Series
Single
819
12
810–980
Almedia*†
30
2009
RCT (vs RFA)
Multi
41
1
980
Bush*
86
2005
Series
Single
620
6
940
Chang*
48
2002
Series
Multi
252
-
1,064
Corcos*
87
2008
Series
Single
44
24
808
Darwood†
8
2008
RCT
Single
71
3
810
De Medeiros*
59
2005
RCT
Single
20
1
810
Desmyttere*
24
2007
Prospective series
Multi
511
48
980
Disselhoff*
9
2008
RCT
Single
60
24
810
Disselhoff*
40
2008
RCT
Single
86
24
810
Disselhoff*
34
2005
Series
Single
93
24
810
Fernandez*†
22
2008
Series
Single
1,985
24
810
Gonzalez-Zeh*†
43
2008
RCT
Single
45
12
980
Hayes†
88
2008
RCT
Multi
19
1
1,320
Huang*
89
2005
Series
Single
230
12
810
Jung*†
90
2008
Prospective series
Single
135
3
810
Janne d'Othee
2008
RCT
Single
157
3
810
Kalteis*
61
2008
RCT
Single
47
3
810
Kabnick*
42
2006
RCT
Single
30
12
810
Kabnick*
2006
RCT
Single
30
12
980
Kavuturu*†
91
2006
Series
Single
66
3
940
Labropolous*
75
2006
Prospective series
Single
56
0.25
-
Lu*†
23
2008
Series
Single
1,186
12
810
Marston
77
2006
NRCT
Single
31
1
810
Mekako*†
92
2006
Series
Single
70
3
810
Mekako†
60
2006
RCT
Single
70
3
810
Min*
27
2003
Series
Multi
499
24
810
Min*
93
2001
Series
Single
90
12
810
Myers*
94
2006
Series
Multi
404
36
810
Myers
25
2009
Series
Single
509
48
810
Navarro*
95
2001
Series
Multi
40
6
810
Oh*
96
2003
Series
Single
15
3
980
Perkowski*
39
2004
Series
Single
203
12
940
Pleister
97
2008
Series
Single
50
-
980
Proebstle*
41
2003
Series
Single
41
12
940
Proebstle*
28
2003
Series
Single
109
12
940
Proebstle
32
2004
Series
Single
106
3
940
Proebstle*
38
2002
Series
Single
31
1
940
Proebstle*†
35
2006
NRCT
Single
249
3
940
Proebstle*†
98
2005
NRCT
Single
33
3
1,320
Puggioni*
81
2005
Series
Single
77
0.25
810
Rasmussen*†
14
2007
RCT
Single
69
6
980
Ravi
82
2006
Series
Single
990
0.25
810
Sadick*†
26
2007
Series
Single
94
48
810
Theivakumar†
31
2008
RCT
Single
68
3
810
Theivakumar*
36
2007
Series
Single
644
3
810
Theivakumar†
99
2008
NRCT
Single
84
12
810
Timperman*†
33
2004
Series
Multi
111
6
810 and 940
Timperman*†
37
2005
Prospective series
Multi
100
6
810 and 940
Van den Bremer
100
2008
Series
Single
403
1
980
Viarengo†
101
2007
RCT
Single
27
12
980
Vuylsteke*
71
2008
Prospective series
Single
129
6
980
Vuylsteke*
62
2006
RCT
Single
118
6
980
Yang
102
2006
Series
Single
71
12
1,320