
Abstract
The objective was to study the intraoperative hemodynamic effects of closure of residual arteriovenous fistulae during in situ saphenous vein graft procedures. Data on 60 residual arteriovenous fistulae in nine patients (five men) with a median age of 74 years (range 64–83 years) with critical lower limb ischemia were obtained. Direct measurements of proximal and distal blood pressures in the graft were taken and simultaneous determinations of volume blood flow proximally and distally in the graft with ultrasound transit time technique before and after closure of residual fistulae were made. Closure of a fistula with blood flow around or below 100 mL/min did not increase distal outflow, whereas closure of fistulae with higher blood flow resulted in unpredictable changes in distal outflow. Only fistulae with a blood flow above approximately 100 mL/min may be of hemodynamic significance.
Keywords
The in situ techniques for making an arterial bypass with the great saphenous vein are standard open 1–3 or endovascularly assisted 4 procedures for revascularization of the leg in patients with critical ischemia. Several methods are available for intraoperative identification and closure of the arteriovenous fistulae (side branches from the saphenous vein), 5 but it is controversial 6 whether occlusion of fistulae influences outflow from the graft and distal blood pressure at the outlet of the graft. 7–9 The present intraoperative study was undertaken to determine the acute hemodynamic effects of arteriovenous fistulae closure in terms of proximal and distal graft blood flow rates and blood pressures.
Material and Methods
The study comprised nine patients (five men) with a median age of 74 years (range 64–83 years) with critical ischemia as defined in accordance with the Second European Consensus Document. 10 All patients were operated on electively with an open standard technique under epidural anesthesia. None of the patients required an inflow procedure. After transposition of the great saphenous vein to the common femoral artery, valves were cut by a valvulotome. After pulsating bleeding from the distal cut end of the graft was obtained, the distal end of the graft was anastomosed to the recipient crural artery.
Transit time ultrasound flow probes (diameter 3–5 mm, 2.5 MHz) and intravascular blood pressure lines (fluid-filled catheter, inner diameter 2 mm, Medex transducer Sunrise, FL) were placed proximally and distally on the graft as close to the anastomotic lines as possible (Figure 1). The four recording lines were connected to Cardiomed 4008 equipment (Medi-Stim A/S, Oslo, Norway) for simultaneous online visualization and digital storage for later analysis. By manual external compression, fistulae were located, clipped, and divided through short incisions as required. Volume blood flow rate in mL/min (Qf) through each fistula was derived by subtracting volume blood flow rate recorded at the distal position (Q2) from volume blood flow rate recorded at the proximal position (Q1) before and after closure of that fistula.
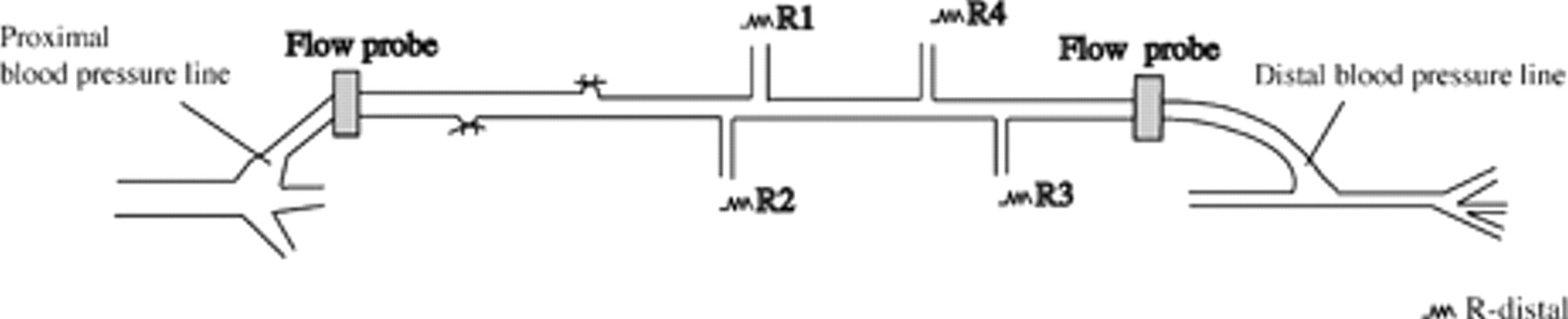
Diagram of the in situ saphenous vein graft with two lines for direct measurements of blood pressures at the proximal and distal anastomoses. The proximal and distal 2.5 MHz ultrasound transit time probes for determinations of volume blood flow rates were mounted on the graft. Blood pressures and flow rates were acquired by transit time ultrasound Cardiomed 4008 equipment with digital storage of data for postprocessing and analyses. R1 through R4 signify the resistance to blood flow in the open side branches (the arteriovenous fistulae) from the graft. Inflow to the left, distal runoff to the right.
Results
Sixty data sets (each of two blood flow rates and two blood pressures) were obtained.
The median in situ graft blood flow rate measured at the proximal location before fistula occlusion was 291 mL/min (range 211–664 mL/min). The median total fistula blood flow rate was 252 mL/min (range 82–648 mL/min). From one to seven residual fistulae were closed (median five). The median blood flow rate through a single fistula was 64 mL/min (range 3–262 mL/min). The median change in distal outflow rate from the graft after ligation of a fistula was 4 mL/min, with values ranging from −49 to 41 mL/min (Figure 2). The median drop in mean blood pressure from the proximal to the distal point of measurement was 9 mm Hg (range −3–23 mm Hg) after closure of all fistulae. Figure 3 and Figure 4 present the changes in proximal mean blood pressure (P1) and distal pressure (P2), respectively, as functions of the change in Qf.
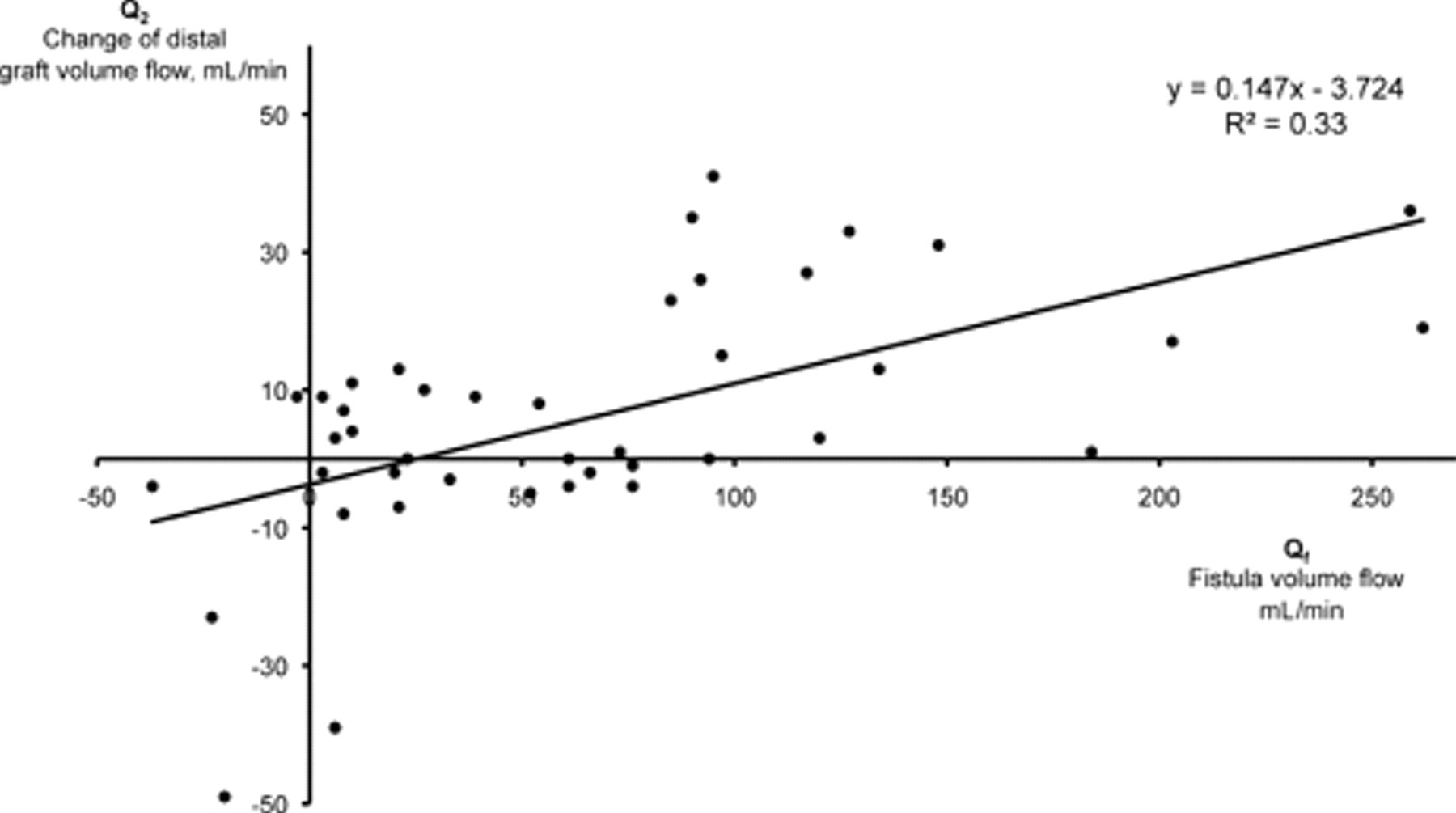
The change in distal graft volume outflow rate (Q2) induced by occlusion of a fistula is plotted in a linear diagram as a function of Qf (volume blood flow rate in that fistula measured immediately before occlusion). The solid line shows y = −3.724 + 0.147x as calculated by the least squares method (r, the correlation coefficient, was .57).
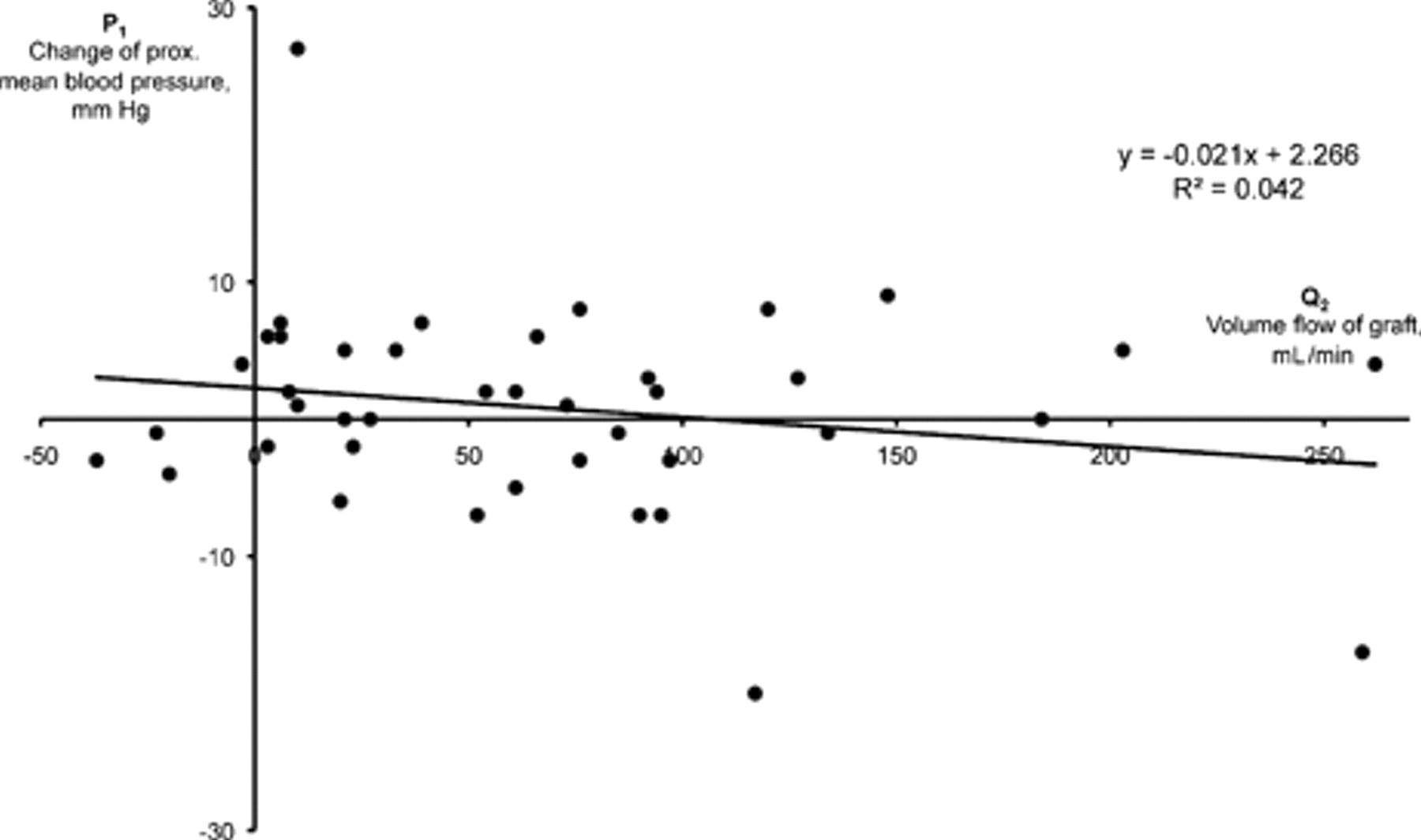
The change in the proximal mean blood pressure in the graft (P1) induced by closure of a fistula is plotted as a function of the volume blood flow rate through that fistula immediately before closure. The solid line shows y = 2.266 − 0.021x as calculated by the least squares method (r, the correlation coefficient, was .20).
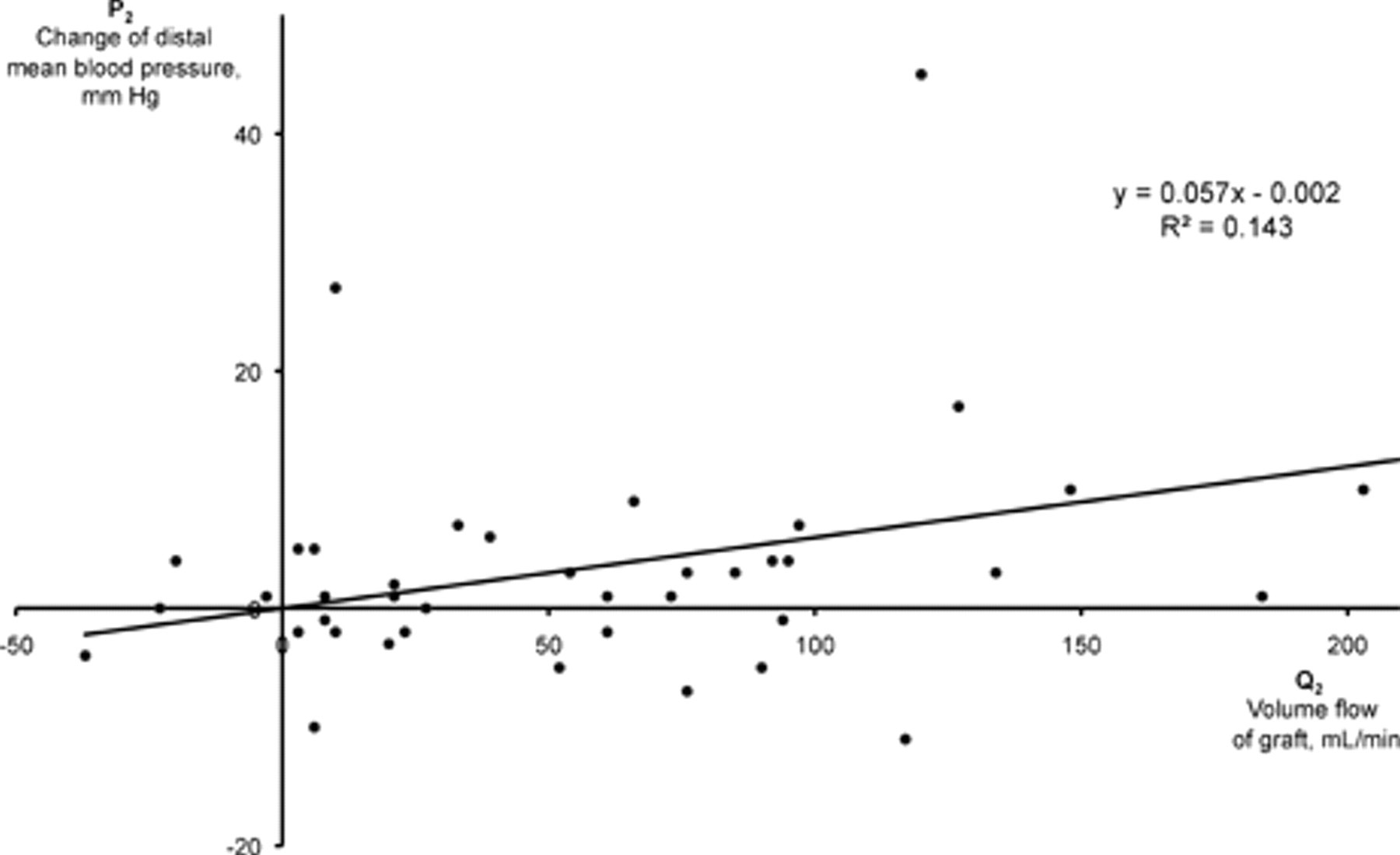
The change in the distal mean blood pressure in the graft (P2) induced by closure of a fistula is plotted as a function of the volume blood flow rate through that fistula immediately before closure. The solid line shows y = −0.002 + 0.057x as calculated by the least squares method (r, the correlation coefficient, was .38).
Discussion
The transit time ultrasound Cardiomed 4008 equipment used in the present study has previously, in a validation study, been found to measure volume blood flow rate through in situ saphenous venous grafts and through aortocoronary bypasses with high precision. 11 The technique is simple and provides real-time, online recordings of volume blood flow rate and blood pressures together with options for digital data storage for postprocessing and offline analyses.
The main finding of the present study was that the hemodynamic effect of closure of residual arteriovenous fistulae is arbitrary in the individual case. Closure of a fistula with blood flow below 100 mL/min did not increase distal outflow, and closure of a fistula with blood flow over 100 mL/min resulted in unpredictable changes in distal outflow. The bypasses transmitted high blood pressure to the receiving crural arteries regardless of whether arteriovenous fistulae were open.
It is probable that revascularization leads to normalization of the local mechanisms for regulation of peripheral blood flow 12 in the individual tissues in the longer term, so extrapolation of the present findings cannot be made as to the conditions in later postoperative periods. It is to be expected, however, that residual fistulae may continue to enlarge and thus divert more and more blood flow as the peripheral resistance increases owing to the progression of the atherosclerotic disease.
In a study using proximal and distal electromagnetic flowmeters on in situ saphenous grafts for critical ischemia, it was found that patent branches would cause decreased distal blood flow from the graft in some cases. 13 It was concluded that the hemodynamic significance of vein branches was determined by the resistance in their drainage bed and that this factor could not be reliably predicted from the size or the site of the fistula. These authors found a significant increase in distal graft blood pressure after closure of all fistulae, but the blood pressure in the graft was measured through a side branch toward the distal end of the graft (distance unspecified).
Earlier postoperative studies indicated an increased risk of graft failure with patent side branches, 3 but more recent series have not confirmed this. 7,14,15 A specific problem is whether duplex ultrasonography, most commonly used for estimations of graft and fistula blood flow, is suited to these types of investigations. 15
Generally, there seems to be a tendency of a more restrained policy toward closure of asymptomatic fistulae except in cases with concomitant proximal graft stenosis or small vein size. 7,15
Conclusion
This study showed, by direct intraoperative measurements, that occlusion of residual fistulae only minimally influenced graft runoff. Intraoperative closure of fistulae with a blood flow above approximately 100 mL/min gave hemodynamically unpredictable results.
Footnotes
Acknowledgment
Financial disclosure of authors: This study was supported by the Danish Heart Foundation and the John and Birthe Meyer Foundation.
Financial disclosure of reviewers: None reported.