
Abstract
Coiling of the artery is a rare morphologic entity most frequently described in the internal carotid artery. Herein we present two cases with symptomatic kinked internal carotid artery: one suffering from paresthesia of the right arm and speech disturbances and the other suffering from weakness of the left half of the body and speech disturbances. Both patients were treated surgically. None of the patients experienced any peri- or postoperative complications.
Coiling of the artery is a rare morphologic entity most frequently described in the internal carotid artery (ICA) as a cause of cerebrovascular insufficiency or in association with carotid atherosclerosis. 1 In other arteries, coiling is rarely reported because it remains asymptomatic and has no clinical relevance. 2 Herein we present two cases with symptomatic kinked ICA that we operated on in our clinic.
Case Report
Two patients underwent surgery in our department for symptomatic ICA kinking. These two patients were admitted to the Department of Neurology. One of these patients was a 46-year-old male suffering from paresthesia of the right arm and speech disturbances. His past medical history revealed dizziness when hyperextending the neck. Doppler ultrasound examination showed elongation of the left ICA with normal flow characteristics, confirmed as kinking by magnetic resonance angiography (Figure 1).

Angiographic view of kinking of the internal carotid artery (the first patient).
The other patient was a 53-year-old female suffering from weakness of the left half of the body and speech disturbances. Her physical examination was significant for dizziness and nausea when turning her head from side to side, which were relieved by resuming the neutral position. Doppler ultrasound examination showed suspected angulation of the right ICA, which was confirmed by conventional selective carotid arteriography (Figure 2).
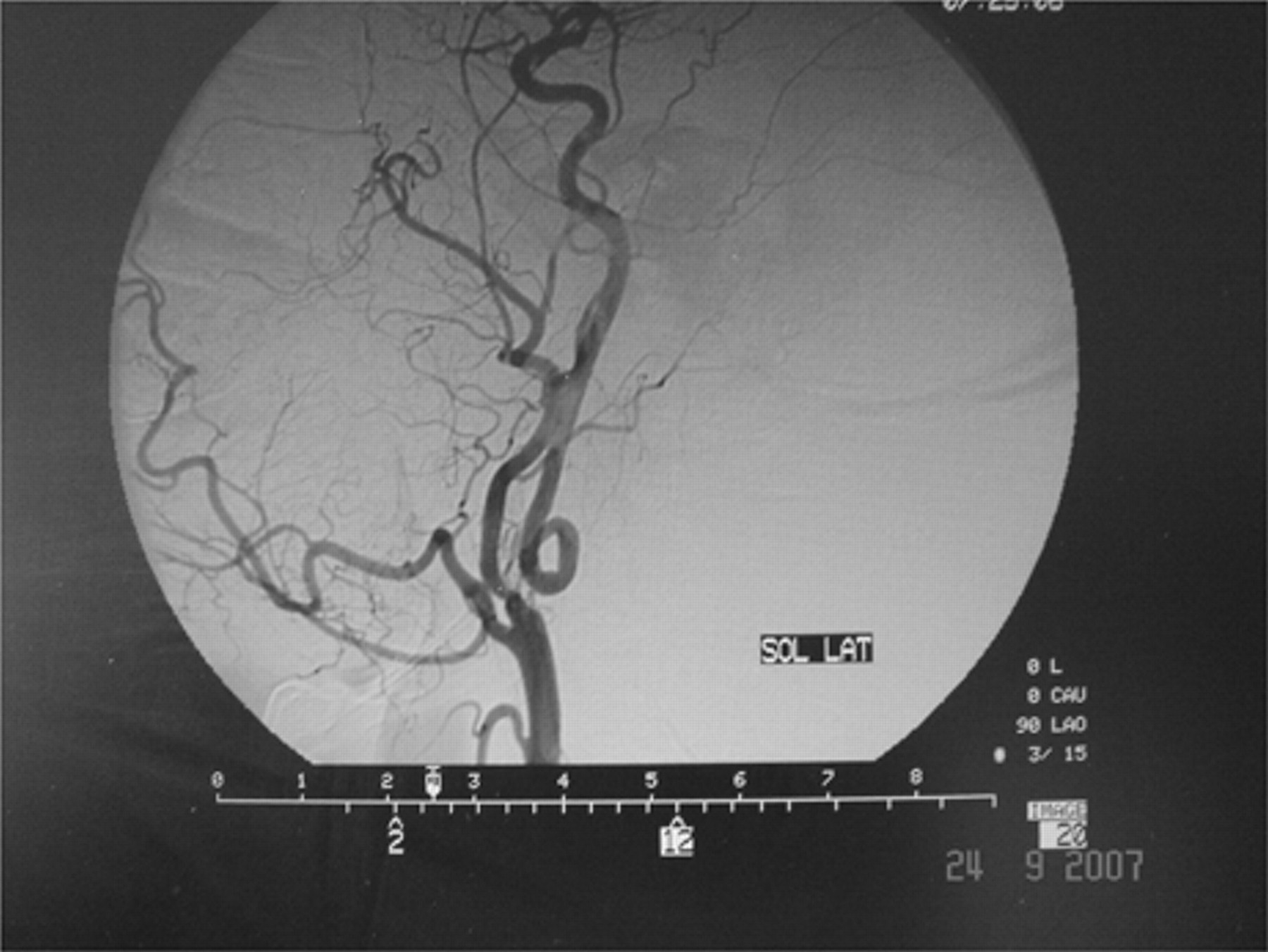
Angiographic view of kinking of the internal carotid artery (the second patient).
Both patients were operated on under general anesthesia with endotracheal intubation. The kinked segment of the carotid artery was resected. The first patient underwent end-to-end anastomosis of the ICA. The other patient underwent end-to-side anastomosis of the ICA to the common carotid artery (CCA) below the level of bifurcation (Figure 3 and Figure 4). None of the patients experienced any peri- or postoperative complications. One patient was discharged on the fourth postoperative day, whereas the other was discharged on the fifth day.

Operative view of kinking of the internal carotid artery (the first patient).
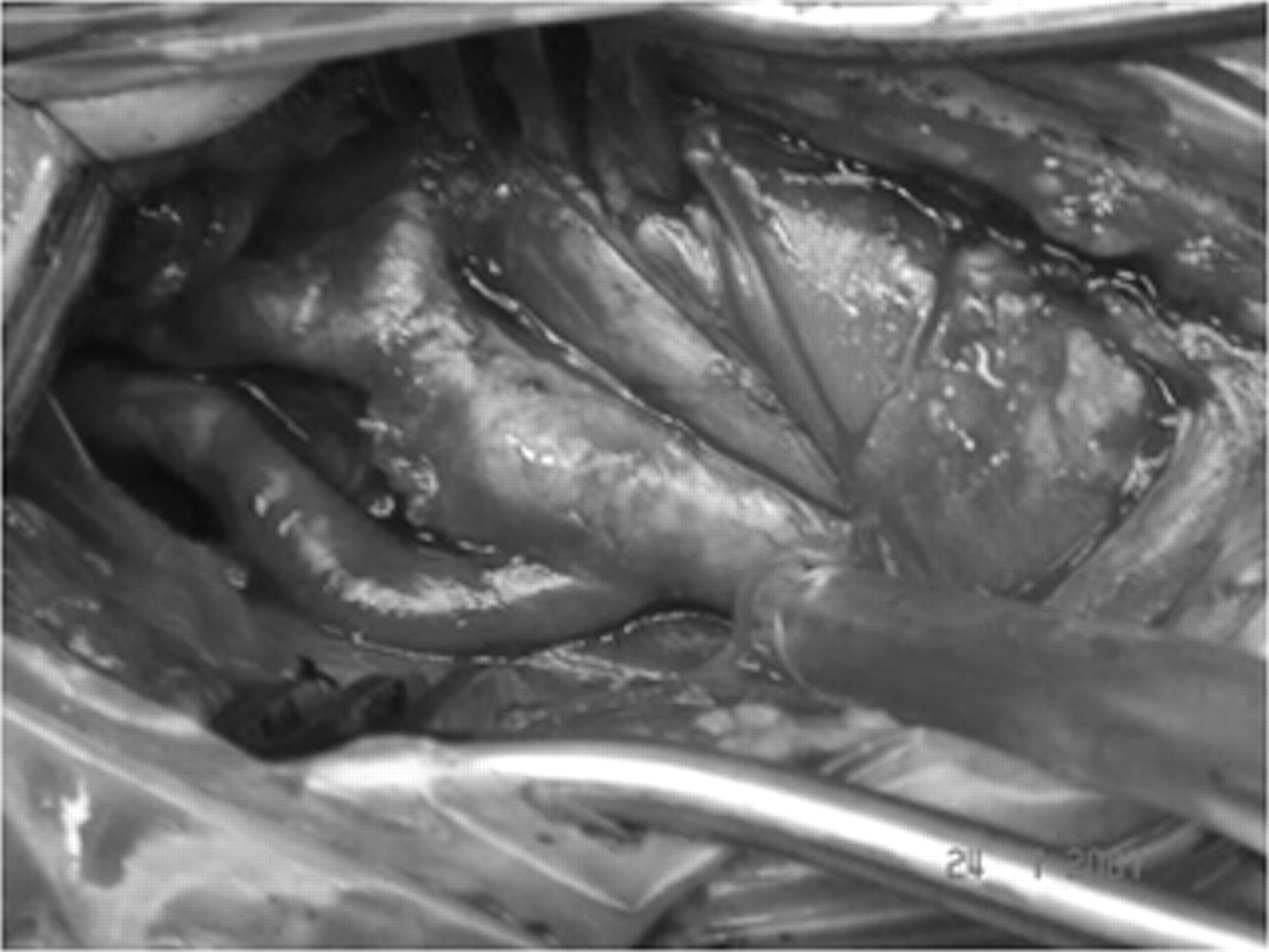
Operative view; kinked internal carotid artery resected and anastomosed to the common carotid artery (the first patient).
Comment
Whether surgically correcting symptomatic carotid elongation with coiling or kinking in the absence of an atherosclerotic lesion of the carotid bifurcation is effective in preventing stroke remains a controversial issue. Although there are numerous studies in the literature on carotid elongation with coiling or kinking in the absence of atherosclerotic lesion of the carotid bulb (isolated elongation), many doubts remain as to its etiology, clinical role, and best management. 3 The only aspect fully clarified concerns the terminology, introduced by Metz and colleagues 4 and Wiebel and Fields 5 in the 1960s: coiling is an elongation of the ICA in a restricted space, causing tortuosity and resulting in a C- or S-shape curvature or a circular configuration, and kinking is a variant of coiling, that is, an angulation of one or more segments of the ICA. The etiology of these peculiar arterial modifications seems to be related to a congenital basis, which may become exaggerated with aging of the artery. 6
Coiling of the
The aim of this study was to analyze our experience in the surgical treatment of symptomatic ICA coiling or kinking. In follow-up, we did not observe any vascular complications and recurrent symptoms. Our results indicate that surgical correction of symptomatic ICA coiling or kinking can be performed with excellent postoperative relief of signs and symptoms.
Footnotes
Acknowledgment
Financial disclosure of authors and reviewers: None reported.