
Abstract
Many hemodynamic factors have been shown to be associated with increased intimal hyperplasia at the distal anastomosis of arterial bypass graft. However, the relationship between the length of anastomosis and the development of such a complication has not been studied before. The aim of this study was to assess this relationship at the distal anastomosis with a Dacron graft. Iliofemoral bypass using 6 mm Dacron grafts was performed in 10 German shepherd dogs. In accordance with preoperative randomization to individual animal legs, distal anastomoses were reconstructed using four different groups (A, B, C, and D), depending on the length of the arteriotomy: 3.0, 3.5, 4.0, and 4.5 times the internal diameter of the artery, respectively. The vessels were harvested 6 months after the operation, and specimens were processed for histologic and transmission electron microscopic (TEM) studies. Quantitative analysis was performed to assess the extent of intimal hyperplasia at three zones (heel, toe, and midzone of the arterial bed) of the distal anastomosis. Sixteen arterial bypasses were included in this study. Both light and TEM studies revealed evidence of intimal hyperplasia in the four groups. Quantitative analysis showed a significant decrease in intimal hyperplasia with increasing the length of the anastomosis at the heel, toe, or midzone of the arterial bed. Mean (μm ± SD) intimal hyperplasia of the three zones together was significantly higher in group A than group B (585 ± 106 vs 423 ± 8.6, p < .001) and in group B than group C (423 ± 8.6 vs 202 ± 15, p < .001). However, the difference between group C and group D (202 ± 15 vs 162 ± 8.6; p = .13) was statistically insignificant. The present study showed that the length of the anastomosis is one of the hemodynamic factors involved in the development of intimal hyperplasia. Anastomotic techniques that resulted in the least intimal hyperplasia were end to side, with length 4 or 4.5 times the internal diameter of the artery.
Prosthetic grafts are commonly used for lower-extremity arterial bypass grafting when no suitable autologous material is available. However, they accelerate the development of intimal hyperplasia, which remains the major cause of graft failure, especially in distal anastomosis. 1–3 Compliance mismatch between the native vessel and the graft is considered to be one of the most important factors implicated in the development of intimal hyperplasia. 4 This factor can lead to adverse local hemodynamic effects at the anastomosis with consequent greater intimal thickening and eventual graft failure. 5–7
Many hemodynamic factors 4,8 have been shown to improve the compliance mismatch and hence to be associated with decreased intimal hyperplasia at the distal anastomosis of the arterial bypass graft. However, the relationship between the length of the arteriotomy and the development of such a complication has not been studied before. The aim of this study was to assess this relationship at the distal anastomosis using a Dacron graft with different arteriotomy lengths.
Material and Methods
Ten apparently healthy adult German shepherd dogs (3–5 years old) of both genders were used in this study. The study was carried out at the departments of Surgery and Histology, Faculty of Medicine, and the Department of Surgery, Faculty of Veterinary Medicine, Suez Canal University, Egypt. The animals' weights ranged between 25 and 20 kg. The experimental study was performed in accordance with national laws on animal experiments, with the permission of the local university ethics committee.
About 10 to 15 minutes prior to the induction of general anesthesia, each dog was premedicated with an intramuscular injection of chloropromazine hydrochloride, 1 mg/kg body weight (Neurazine, Misr Co. Pharm. Ind., Cairo, Egypt). 9 General anesthesia was then conducted by intravenous injection of thiopental sodium 2.5% (maximum dose is 20 mg/kg body weight; Egyptian International Pharmaceutical Industries Co., Egypt). 10
Under sterile conditions, bilateral inguinal incisions were made. The terminal parts of the external iliac artery and femoral arteries, on both sides, were dissected free. A segment approximately 3 to 4 cm in length was cut out from the femoral arteries after accomplishing proximal and distal control of the vessel. The segment (control) was divided in the midsagittal plane. One half was prepared for light microscopic study and the other for transmission electron microscopy (TEM). Iliofemoral bypass using 6 mm diameter, 10 cm long knitted Dacron grafts (InterGard Silver UltraThin, InterVascular, France) were performed. In accordance with preoperative randomization to individual animal legs, distal anastomoses were reconstructed using four different groups (A, B, C, and D) depending on the length of the arteriotomy: 3.0, 3.5, 4.0, and 4.5 times the diameter of the artery, respectively. The internal diameters of the femoral artery of all dogs were about 2.5 mm. Standard end-to-side anastomoses were constructed. All anastomoses were constructed with continuous 6-0 polypropylene (Ethicon, Somerville, NJ) with the aid of surgical magnifying loups. Prophylactic antibiotic (three doses of cefotaxime 500 mg) were administered intravenously twice on the day of surgery and once on the following day. After surgery, the animals were kept under natural housing conditions under the care of a veterinarian without any medication for 6 months. During the study period, follow-up of the graft flow was checked with an ultrasound (Advanced Bi-Directional Doppler, Huntleigh, UK) 1 week postoperatively and then every month.
After 6 months, the dogs were brought back to the operating room for harvesting of the anastomosed vessels. Incisions were made on both legs under general anesthesia. On-table angiography was performed to confirm the patency of the distal anastomosis (Figure 1). The distal anastomotic regions were clamped and excised. The animals were euthanized by intravenous administration of potassium solution (4.48 g potassium in 60 mL water). The excised segments were divided in the midsagittal plane. One half was prepared for light microscopy and the other for TEM study.

On-table angiogram showing a patent graft (arrow) and a tiny filling defect at the distal anastomosis (curved arrow).
Light Microscopy
Specimens for light microscopy were fixed in 10% neutral buffered formalin solution. They were then processed to prepare 5 μm thick paraffin sections for histologic stains (hematoxylin-eosin and elastic–Verhoeff-van Gieson stain). The specimens were cut transversely at three different locations: the anastomotic heel, the midsection at the floor of the artery, and the anastomotic toe. Qualitative analysis of both control and distal anastomosis specimens was carried out. Quantitative assessments of intimal hyperplasia (distance; μm ± SD, from lumen to internal elastic lamina) were measured in the different groups using an image analyzer (Super eye-Heidi software, Heidi Software Company, Cairo, Egypt).
Statistical Analysis
The results were summarized using descriptive statistics. These are presented as mean ± SD and compared using Student t-test or analysis of variance as appropriate. Significance was set at p < .05 for all comparisons. All statistical analyses were performed with the aid of SPSS 15 (SPSS Inc, Chicago, IL) software.
Electron Microscopy
Specimens for electron microscopy were immediately immersed in 2.5% glutaraldehyde solution. Each specimen was trimmed, immediately fixed in glutaraldehyde solution in 0.1 M sodium cacodylate buffer, pH 7.2, and kept at 4°C for 2 hours. They were postfixed in 1% osmium tetroxide in sodium cacodylate buffer and then dehydrated in an ascending series of ethyl alcohol and embedded in Spurr resin. Semithin sections (1 mm) stained with toluidine blue were obtained for observation. Ultrathin sections stained with uranyl acetate and lead citrate were examined at 80 kV under a transmission electron microscope (Jeol, JEM 1010, Japan).
Results
Two dogs developed small hematomas in the groin, which were treated conservatively. One groin was complicated with superficial inflammation, which diminished with antibiotics. One dog died without apparent reason, 4 months after the operation. Two grafts failed during the follow-up period, one from group A and the other from group B. They were excluded from statistical analysis. Thus, 16 arterial bypasses were included in this study. Each group comprised four bypass grafts. At 6 months, the distal anastomotic sites were patent in the 16 grafts. However, there was weak flow (nonpulsatile) in all grafts of group A and two grafts in group B (50%). During the study period, there were no other morbidities.
Light microscopy revealed development of intimal thickening at the distal anastomosis of all grafts compared to normal artery (Figure 2). The intimal thickening was composed of a monolayer of endothelial cells (sometimes lost), proliferated smooth muscle cells, and intercellular connective tissue formed mainly of collagen and some elastic fibers. TEM confirmed the above findings (Figure 3).

A, Section in normal artery showing that the wall is formed of thin intima and thick media and adventitia (hematoxylin-eosin stain ×250 original magnification). B, Wall of normal artery showing black-colored elastic fibers forming internal elastic lamina between the intima and media (elastic–Verhoeff-van Gieson stain; ×250 original magnification). C and D, Sections at the distal anastomosis showing intimal thickening (arrows) composed of a monolayer of endothelial cells, smooth muscle cells, and collagen fibers (C, hematoxylin-eosin stain; ×250 original magnification; D, elastic–Verhoeff-van Gieson stain; ×250 original magnification).

Electron micrograph. A, Section of normal artery showing part of the intima. It is formed of apparently normal endothelial cells facing the lumen, with subendothelial connective tissue formed of collagen and elastic fibers (×10,000 original magnification). B and C, The artery at the distal anastomosis showing that the arterial lumen is not lined by endothelium. The intimal hyperplasia is formed of collagen fibers, some elastic fibers, and smooth muscle cells (×8,000 original magnification). D, The artery at the distal anastomosis showing smooth muscle cells and collagen fibers (×10,000). C = collagen fibers; E = elastic fibers; EC = endothelial cells; L = lumen; SMC = smooth muscle cells.
Quantitative analysis showed a significant decrease in intimal hyperplasia at the heel with increasing the length of the arteriotomy (595 ± 109 vs 443 ± 129 vs 185 ± 81 vs 168 ± 94, p < .001, for group A, B, C, and D, respectively) (Figure 4). The same observation was found at the midzone of the arterial bed (566 ± 155 vs 432 ± 87 vs 192 ± 88 vs 156 ± 46, p < .001, for group A, B, C, and D, respectively) (Figure 5) and at the toe (581 ± 131 vs 394 ± 35 vs 266 ± 162 vs 176 ± 73, p < .001, for group A, B, C, and D, respectively) (Figure 6).

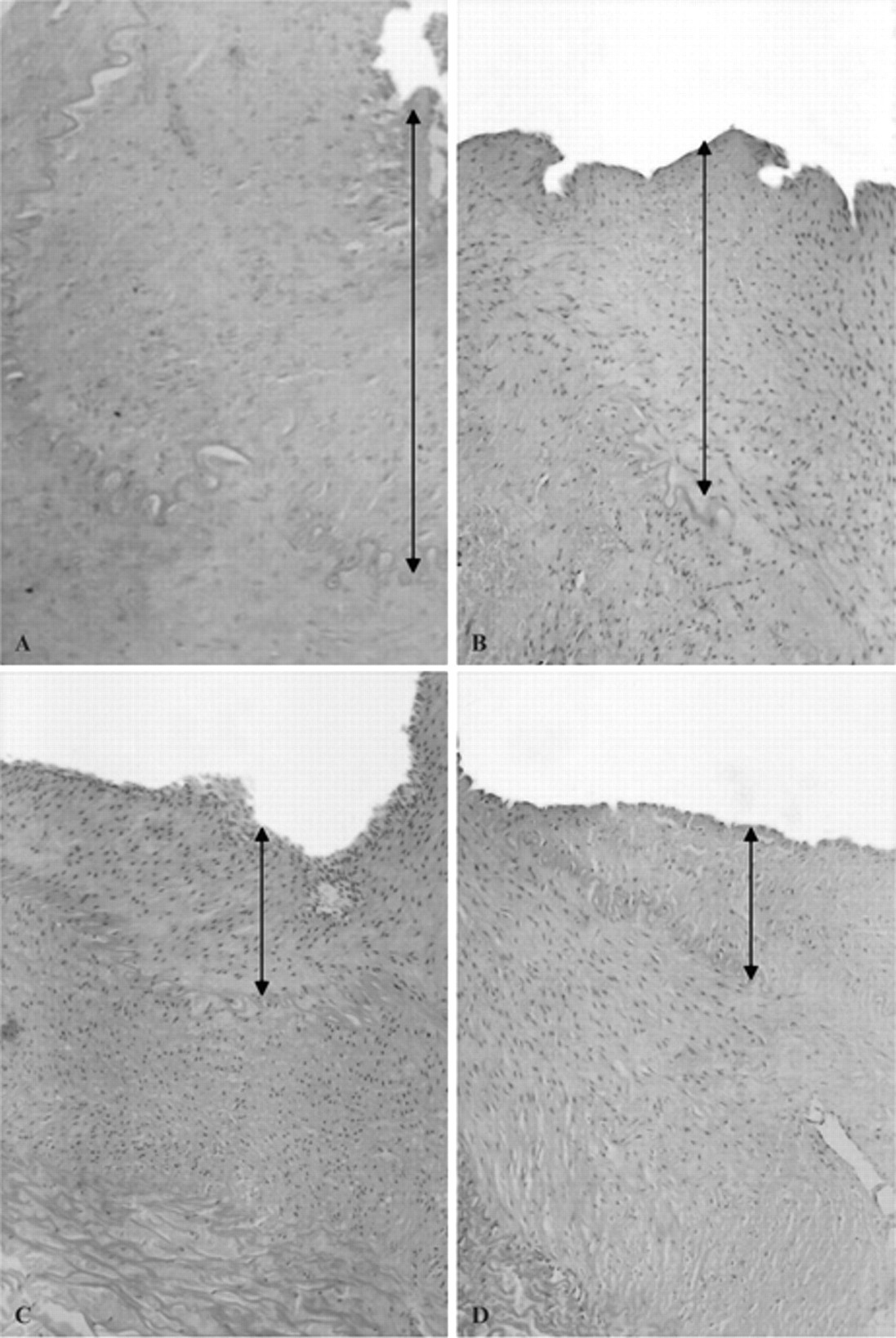
Sections at the heel of the distal anastomosis showing intimal hyperplasia (arrows) in the different groups (A, B, C, and D). Note the decrease in intimal hyperplasia with increasing the length of the arteriotomy (hematoxylin-eosin stain; ×100 original magnification).

Sections at the midzone of the arterial bed of the distal anastomosis showing intimal hyperplasia (arrows) in the different groups (A, B, C, and D). Note that intimal hyperplasia decreased with increasing the length of the arteriotomy (hematoxylin-eosin stain; ×100 original magnifcation).
Sections at the toe of the distal anastomosis showing intimal hyperplasia (arrows) in the different groups (A, B, C, and D). Note also the decrease in intimal hyperplasia with increasing the length of the arteriotomy (hematoxylin-eosin stain; ×100 original magnification).
The mean intimal hyperplasia of the three zones together was significantly higher in group A than in group B (585 ± 106 vs 423 ± 8.6, p < .001) and in group B than in group C (423 ± 8.6 vs 202 ± 15, p < .001). However, the difference between group C and group D (202 ± 15 vs 162 ± 8.6, p = .13) was statistically insignificant.
Discussion
Although intimal hyperplasia was reported a long time ago, 11 its role as the main cause of thrombotic complications occurring between 2 and 24 months after a vascular intervention has not been recognized until recently. 1 Extensive studies have been performed to know more about the pathogenesis of this complication to reduce its development. Although some solutions have had promising results with respect to improved patency of peripheral bypass grafts, the impact of intimal hyperplasia on the field of vascular intervention remains high. 12 More studies are required to find pharmacologic and hemodynamic interventions that can diminish the formation of intimal hyperplasia. The present study was made to assess the effect of one of these hemodynamic factors.
Intimal hyperplasia is commonly found at the toe, heel, and arterial floor near the distal anastomosis of the arterial bypass graft. 13 At the floor of the arterial wall and at the heel of the anastomosis, where the blood flow divides proximally and distally, the wall shear stress will be low. This affects expression of some vasoactive molecules, which are involved in the formation of intimal hyperplasia. In addition, the change in the direction of shear force that occurs during the systolic phase of the flow cycle, defined as the oscillatory shear index, is high at the anastomotic heel and the arterial floor. 5 This high oscillatory shear index may provide a stimulus for development of intimal hyperplasia. 14 At the toe of the anastomosis, the wall shear stress gradient is high, 15,16 which may be responsible for development of intimal hyperplasia at this site. 17 For the above reasons, the toe, the heel, and the arterial floor near the distal anastomosis of the arterial bypass graft were chosen for the measurement of intimal hyperplasia in the present study.
Many factors have been shown to be implicated in the development of intimal hyperplasia, such as suture materials, surgical techniques, 4,8 and pharmacologic intervention. 12 In the present study, there was no difference between groups with regard to the above-mentioned factors. All bypasses were also performed with the same material (Dacron), diameter, and length. Although there were slight variations between groups (eg, angle of anastomosis), the previous measures minimized the differences between all operations.
The present study is the first, to our knowledge, to assess the effect of the length of the arteriotomy on the degree of intimal hyperplasia at the distal anastomosis. The study showed that increasing the arteriotomy length up to four times the internal diameter of the artery minimized the development of intimal hyperplasia. This may be explained by Poiseuille's law, which says that the pressure of flow for blood through a conduit is inversely proportional to the fourth power of its radius. This also explains how reduced flow velocity at the anastomotic floor of the Venaflo (Bard-IMPRA, Tempe, AZ) cuffed polytetrafluoroethylene (PTFE) anastomosis prevents excessive shear stress, translating to reduced intimal hyperplasia. 18 A vein cuff or the Distaflo (Bard-IMPRA) PTFE graft widens the distal anastomosis, and both are used clinically with better patency than PTFE alone. 19,20 Conversely, a grossly oversized distal conduit results in a sudden decrease in flow rate with relative stasis and flow separation. The resultant low shear rate is associated with intimal hyperplasia, as discussed earlier. Hence, the ideal diameter difference between graft and artery at the distal anastomosis is a balance to maintain the ideal flow velocity and resist turbulent flow. 21 This may suggest that an arteriotomy 4.5 times the internal diameter of the artery is not better than 4 times the diameter with regard to the formation of intimal hyperplasia in the present study. It will be expected that intimal hyperplasia may increase if the arteriotomy length is more than 4.5 times the internal diameter of the artery.
Intimal hyperplasia occurs as a result of abnormal proliferation and migration of cells to the tunica intima of a vessel wall. 1 It is composed of about 20% of vascular smooth muscle cells that have migrated from the media to the intima and have proliferated and deposited extracellular matrix, which comprises most of the intimal area. Other components of the intimal hyperplasia are macrophages and lymphocytes. The surface may or may not be endothelialized, depending on the extent of and time passed since the intimal damage. 22 The same findings were found in the present study, as revealed by both light and TEM studies. Proliferation of smooth muscle cells results from endothelial cell damage as the normal endothelium produces factors that inhibit vascular smooth muscle proliferation. 22 This endothelial damage might result from surgical exposure and dissection damage to the vasa vasorum and autonomic nerves. 12 The proliferated smooth muscle cells resemble the fetal type and can produce four to five times more extracellular matrix than the differentiated ones. 22
The present study has few limitations. It assessed the development of intimal hyperplasia in only medium-sized vessels. It also investigated this complication using a synthetic graft. Moreover, it was an experimental study, and some experimental studies, which showed a favorable outcome using a certain technique, failed to prove this advantage in multicenter clinical trials. 23
In summary, the present study showed that the length of anastomosis is one of the hemodynamic factors involved in the development of intimal hyperplasia. Anastomotic techniques that resulted in the least intimal hyperplasia were end to side with a length 4 or 4.5 times the internal diameter of the artery. However, more extensive experimental and clinical studies on arteries of different sizes are required.
Footnotes
Acknowledgment
Financial disclosure of authors and reviewers: None reported.