
Abstract
Blood blister–like aneurysms (BBAs) are rare but challenging to treat owing to their fragile, thin walls and poorly defined necks. A right-sided aortic arch is an uncommon congenital cardiac anomaly with an estimated incidence of only 0.1% and presents a challenge to intubation at vessels above the aortic arch. This represents an extremely rare case of a BBA at the left internal carotid artery with a right-sided aortic arch treated with combined endovascular and vascular surgical therapy. We report the case and provide a short review of the relevant literature.
A blood blister–like aneurysm (BBA) refers to a small hemispherical bulge from the arterial wall. Although the lesion resembles a small berry aneurysm, it has different clinical features, such as thin walls and a poorly defined neck. Several reports have described BBAs as arising at nonbranching sites from the dorsomedial wall of the internal carotid artery (ICA), 1–4 and BBAs constitute up to 7% of ICA aneurysms. 2,5 However, we found no reports in the English-language literature of BBAs combined with a right-sided aortic arch. In this retrospective review, we present a rare case with a BBA at the left ICA combined with a right-sided aortic arch and discuss the therapeutic aspects of the case.
Case Report
A 44-year-old man presented to the emergency department with an acute headache lasting for 4 hours and conscious mental status. The headache was associated with nausea and projectile vomiting. The patient was also known to be hypertensive for 8 years.
His emergency computed tomographic (CT) scan revealed a subarachnoid hemorrhage (modified Fisher grade IV), with blood mainly in the basal cistern and both sylvian fissures, with the left side having slightly more blood than the right (Figure 1A). Magnetic resonance angiography (MRA) revealed an irregularity at the C7 segment of the left ICA, but no aneurysm was confirmed on the image (Figure 1B). This patient was admitted and commenced on nimodipine, mannitol, and p-aminomethylbenzoic acid intravenously to treat subarachnoid hemorrhage. Diagnostic angiography was done the day after admission and showed a right-sided aortic arch, and selective catheterization to the left common carotid artery failed (Figure 2A). Consequently, nonselective angiography of the left carotid artery at the aortic arch was performed and no aneurysm was revealed at the left ICA.
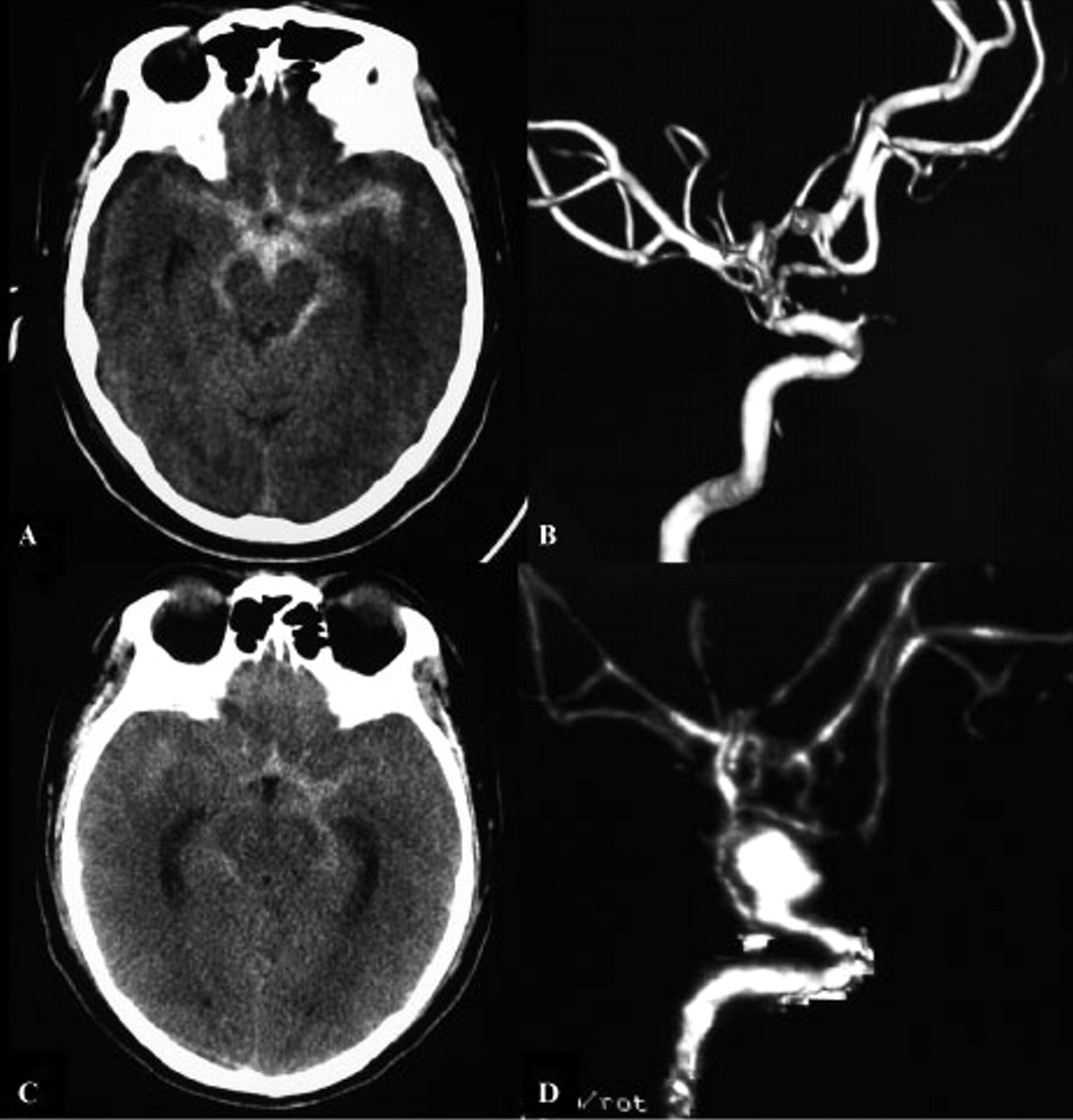
A, Axial unenhanced computed tomographic (CT) image showing a diffuse subarachnoid hemorrhage in the basal cistern and bilateral sylvian fissures. B, Left internal carotid artery (ICA) magnetic resonance angiogram at the time of presentation demonstrated no aneurysm. C, Unenhanced CT scan after 12 days' admission revealed a recurrent subarachnoid hemorrhage in the basal cistern and left sylvian fissures. D, A CT angiogram at the same time demonstrated a large aneurysm at the C7 segment of the anterior wall of the left ICA.

A, An emergence digital subtraction angiogram demonstrated a right-sided aortic arch variation at the right anterior oblique position. B, A lateral position angiogram after 12 days admission revealed a large aneurysm (5 × 6 mm) at the C7 segment of the left internal carotid artery. C and D, The lateral position plain film and subtracted angiogram demonstrated a nearly complete coil embolism, and the parent artery maintained good patency.
Twelve days after admission, this patient presented with acute unconscious mental status and shortness of breath. After first aid support, his vital signs were stable, and his condition changed to conscious mental status with a right hemiplegia. The patient received an acute brain CT scan, and computed tomographic angiography (CTA) was performed at the same time to exclude any further hemorrhage in the brain or any vascular abnormalities. The CT scan revealed a recurrent subarachnoid hemorrhage, and CTA demonstrated a large aneurysm located at the nonbranched anterior arterial wall of the C7 segment in the left ICA separated from the posterior communicating and choroidal arteries (Figure 1, C and D).
It was clear that this aneurysm was the cause of the rehemorrhage; thus, an aneurysm embolization was planned and performed. Considering that the right-sided aortic arch may have caused the failure of catheterization of the left ICA, exposure of the left CCA was performed with the help of two other vascular surgeons, and then a puncture was done followed by the placement of a 6F introducing sheath. A 6F guiding catheter (Envoy, Cordis Endovascular Systems, Warren, NJ) was placed at the distal cervical segment of the left ICA. Immediate angiography confirmed a large aneurysm (5 × 6 mm) at the C7 segment of the left ICA (Figure 2B). Next, the aneurysm was selected with a 0.014-inch microcatheter (Enchalon-10, eV3, Plymouth, MN) and a 0.010-inch microguidewire (Transend, Boston Scientific, Natick, MA). Altogether, seven detachable coils, measuring 6 mm × 20 cm in one, 3 mm × 10 cm in two, 2 mm × 8 cm in one, 2 mm × 6 cm in two, and 2 mm × 4 cm in one (Nexus, eV3), were inserted into the aneurysm sac. The postprocedural angiogram showed mostly occlusion of the aneurysm (Figure 2, C and D). Then the puncture site of the left ICA was sutured. Finally, the muscle and skin were layer-sutured. After the guiding catheter was introduced, a bolus of 4,000 U of heparin was injected intravenously and an additional 1,000 U was added every hour to maintain heparinization conditions during the procedure. Nimodipine (10 mg) diluted in 250 mL of saline was intravenously transfused during the procedure to prevent intracranial vasospasm. Nonenhanced brain CT was performed postprocedure to occlude any intracranial hemorrhage or ischemic event, and detailed neurologic examinations were conducted pre- and postprocedure.
This patient tolerated the procedure well, with no further deterioration in his symptoms. His right upper limb muscle strength recovered to grade 2, but the right lower limb muscle strength remained at grade 0 when he was discharged 2 weeks later. Follow-up angiography 3 months after the embolization showed no recurrence or recanalization of the aneurysm. The patient remains well after 6 months, with no recurrent symptoms at our clinical follow-up. His right upper limb muscle strength recovered to grade 4, and the right lower limb muscle strength became grade 1.
Discussion
BBAs are rare lesions characterized by a hemispherical shape and fragile walls. Blister-like aneurysms consist of focal wall defects covered with thin fibrous tissue, compared to berry aneurysms with a wall composed of thickened intima and adventitia. Other typical attributes of blister-like aneurysms are their documented growth or rupture in short intervals and their occurrence at nonbranching points of the supraclinoid ICA. 2,5 Other prominent traits of blister-like aneurysms mentioned in the literature have included the preponderance of arterial hypertension and atherosclerosis. Although most patients presented with massive hemorrhage, initial angiograms obtained soon after subarachnoid hemorrhage showed only a small bulge or even not identifiable, which progressed within a few weeks to a saccular appearance. 2,6
It has been reported repeatedly that direct clipping of a BBA often causes rupture of the lesion, resulting in an apparent wall defect of the feeding artery. Various neurosurgical and/or endovascular tactics have been proposed to treat a BBA. 3,4 Previous reports indicate that either complete wrapping or clipping of the lesion reinforced by wrapping was used most often to treat this kind of lesion but still ran a high risk of hemorrhage. 6 Pelz and colleagues reported two ICA BBAs in two patients treated with preliminary balloon occlusion of the ICA followed by safe surgical trapping of the ICA beyond the aneurysm. 3 Endovascular treatment, including balloon trapping and coil embolization with or without stent assistance, has emerged as a promising treatment for BBAs in recent years. 4,7 Mainly according to our experience and results from the literature, for BBAs with a small hemispherical bulge configuration, endovascular ICA trapping might be the safest technique if the balloon occlusion test of the ipsilateral ICA was negative. But once the BBA has grown into a berry aneurysm configuration within a few weeks, then endovascular coil embolization can be applied safely.
A right aortic arch is by itself a rare condition, comprising approximately 0.1% of cases seen in several studies. 8,9 Many articles have reported a right aortic arch accompanied by a development variation such as an aortic aneurysm, aortic coarctation, Kommerell diverticulum, and an aberrant left subclavian artery. 10–13 More importantly, the right aortic arch may make catheterization difficult because most of the catheters used presently were designed for a left aortic arch application.
We reported a patient harboring a BBA at the anterior wall of the nonbranched left ICA combined with a congenital right aortic arch, which is extremely rare and has not been reported in the English literature. Considering that surgical clipping of the BBA runs a high risk of aneurysm rupture, the endovascular option is the first-level treatment. But the congenital aortic arch malformation made the catheterization nearly impossible. After a discussion with both neurosurgeons and vascular surgeons, we decided to undertake homolateral common carotid artery exposure to create access to the ICA aneurysm. Despite the fact that aneurysm trapping with detachable balloons is believed to be an effective treatment for BBAs of the ICA, given that this patient presented with right hemiplegia and a brain infarction at the left brain hemisphere might have existed, the aneurysm trapping method was not considered and a subsequent balloon occlusion test was not done. After successful coil embolization treatment, nearly complete isolation of the aneurysm sac was achieved immediately, and the follow-up, including the 3-month angiogram and the 6-month clinical symptoms, revealed a good recovery.
Footnotes
Acknowledgment
Financial disclosure of authors and reviewers: None reported.