
Abstract
One of the technical limitations of surgeon-modified fenestrated stent grafts is the lack of a diameter-reducing wire, which facilitates catheterization of target branches if there are errors of device design, alignment, or implantation. This article describes a technique of adding a diameter-reducing wire to the modified TX2 fenestrated stent graft for compassionate use in aortic emergencies or high-risk patients who do not have access to manufactured devices. The modified Cook TX2 stent graft was created using reinforced fenestrations with gold nitinol markers. After the TX2 stent was fully unsheathed, one of the nitinol wires located in the inner cannula was withdrawn and redirected externally through and through the fabric of the stent graft. Each Z stent was constrained using the nitinol wire for support and two nonlocking polypropylene loops. The use of a diameter-reducing wire facilitates side branch catheterization by allowing longitudinal and rotational movement to the modified fenestrated stent graft in patients where there is misalignment between the fenestration and the origin of the target vessel.
Fenestrated stent grafts allow incorporation of the supra-aortic and visceral arteries, expanding the indications of endovascular treatment of complex aortic aneurysms. 1–4 These devices require a period of 6 to 8 weeks for customization and are currently not commercially available in the United States, where their use is restricted to a few institutions for patients who are prospectively enrolled in physician-initiated Investigational Device Exemption (IDE) protocols. Although promising advances will soon allow the development of an off-the-shelf device, approximately 20 to 30% of patients will still require customization, and several centers may not have access to manufactured devices.
Modifications of commercially available aortic stent grafts with creation of fenestrations, scallops, and side branches have been described as an alternative for high-risk patients with complex aneurysms who otherwise would not have access to manufactured devices. 5,6 Uflacker and colleagues were granted the first clinical application of surgeon-modified fenestrated endografts. 5 The technique has several limitations, most notably the lack of quality control on device design. Errors of device design and implantation may result in stent graft misalignment between the fenestration and the origin of the target vessel. 5,6 The addition of a diameter-reducing wire, which constrains the stent graft into a smaller diameter, allows rotational and longitudinal movement of the device. In this article, a novel technique of adding a diameter-reducing wire into the modified TX2 fenestrated stent graft is described in a high-risk patient with a large type IV thoracoabdominal aortic aneurysm.
Technique
A 79-year-old high-risk male patient presented with an enlarging 7.5 cm type IV thoracoabdominal aortic aneurysm (Figure 1A). His medical history was notable for severe chronic obstructive pulmonary disease with forced expiratory volume of 1,200 mL, intermittent home oxygen therapy, congestive heart failure with ejection fraction of 35%, hypertension, hyperlipidemia, coronary artery disease, obesity, and diabetes. A physical examination was unremarkable.
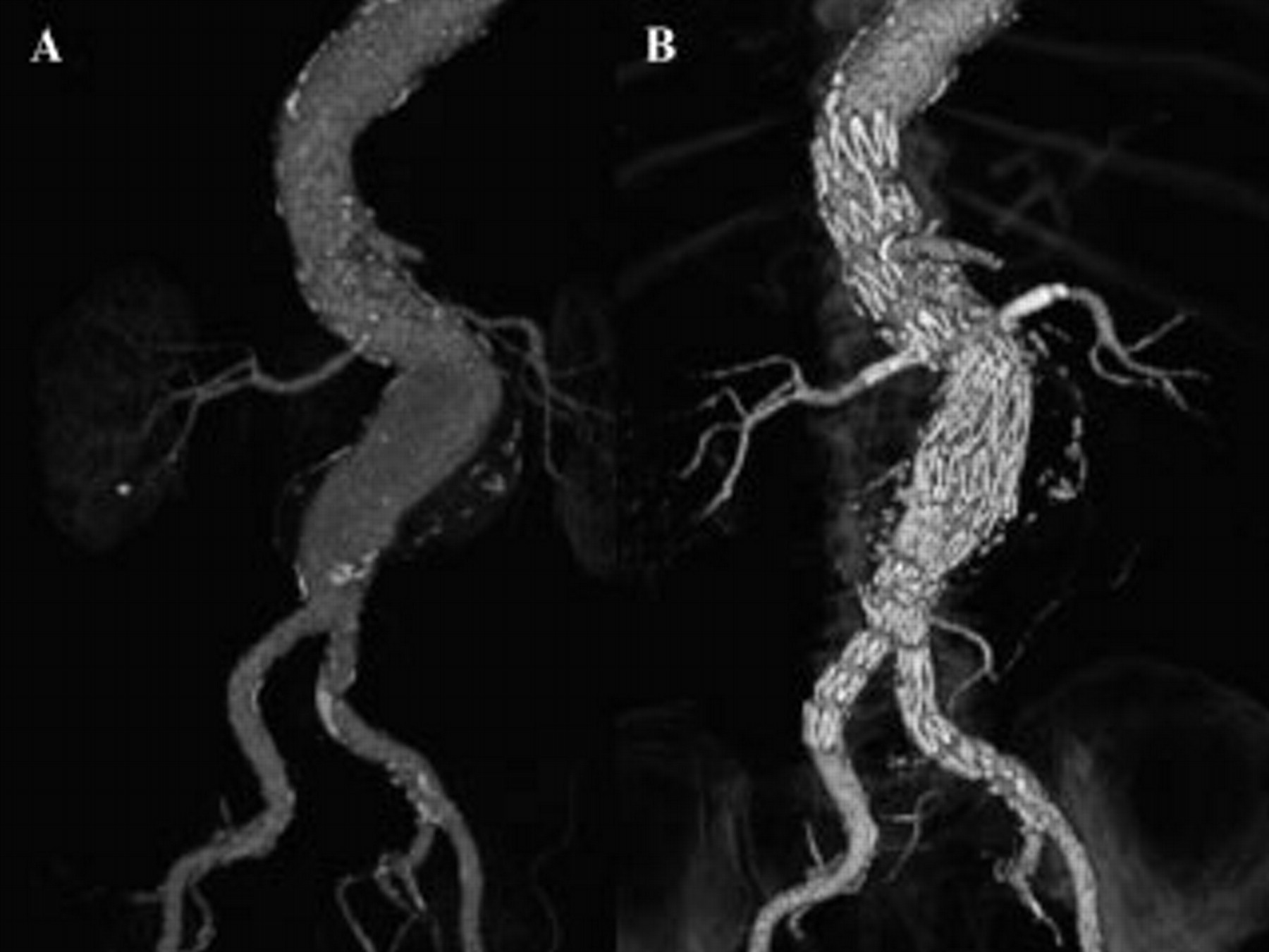
Computed tomographic angiography of the patient's type IV thoracoabdominal aortic aneurysm before (A) and after (B) endovascular treatment using a four-vessel modified fenestrated stent graft.
A surgeon-modified fenestrated stent graft was recommended because of the patient's prohibitively high surgical risk. The patient underwent preoperative cerebrospinal fluid drainage, followed by placement of a modified fenestrated TX2 stent graft (Cook Medical, Bloomington, IN) with four fenestrations to the celiac, superior mesenteric, and renal arteries and a distal modified Cook Zenith stent graft without the top uncovered stent. There were no complications, and the patient was dismissed home on postoperative day 6. Follow-up computed tomographic angiography at 6 months revealed no endoleak and 5 mm sac shrinkage (Figure 1B). The technique used for device modification is described below.
Modifications
The technique of stent graft modification and implantation has been described in detail. 6 A Cook TX2 Tapered 2PT 40 × 36 × 208 mm stent graft (Cook Medical) was modified on site using strict sterile technique. Four fenestrations were created using ophthalmologic cautery and gold nitinol markers (Figure 2A), which were anastomosed using a locking 5-0 Ethibond suture (Figure 2B). A longitudinal anterior marker was placed at 12 o'clock and a transverse posterior marker at 6 o'clock for orientation under fluoroscopy. After creation of the fenestrations and placement of the orientation markers, the diameter-reducing wire was added and routed posteriorly at the 6 o'clock position (Figure 2C). For the distal bifurcated component, a Cook Zenith TFFB 36 × 95 mm was modified by removing the top uncovered stent (Figure 2D).
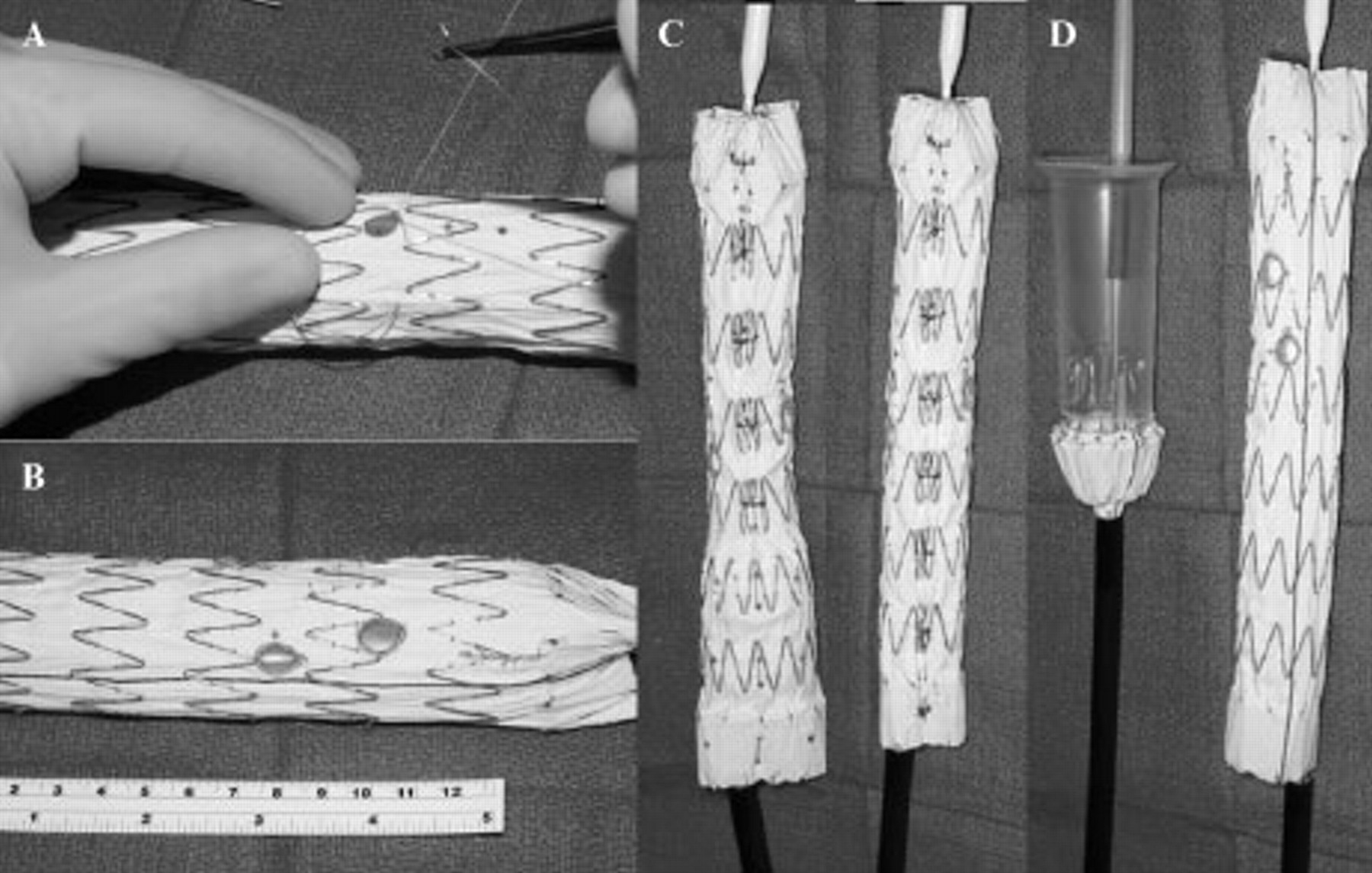
Modifications of the Cook Medical TX2 stent graft. Fenestrations are reinforced with gold nitinol wires using locking 5-0 Ethibond sutures for fluoroscopic guidance (A). The unconstrained stent graft after creation of four fenestrations for the celiac, superior mesenteric, and renal arteries (B). The diameter-reducing wire is added as described in detail in Figure 3, showing the diameter difference between the constrained and the unconstrained portion of the stent graft (C). A distal component is made using the Cook Zenith stent graft (Cook Medical) without the uncovered top stent (D).
The diameter-reducing wire was created using one of the three nitinol wires, which are located in the inner plastic cannula of the TX2 delivery system. To remove the nitinol wire, the TX2 was completely unsheathed (Figure 3A) and a small slit was created at the bottom of the plastic cannula using an 11-blade scalpel (see Figure 3A, inset). It is important to avoid grasping the nitinol wire with a hemostat or clamp because this will fracture the wire; instead, using a curved needle, the wire was pulled out from the inner cannula. After the wire was exteriorized, it was routed posteriorly at the 6 o'clock mark as demonstrated in Figure 2C and Figure 3B. A 22-gauge spinal needle was used to facilitate routing the nitinol wire through and through the fabric of the stent graft, noting that the wire was routed in the middle of the struts of the Z stent (see Figure 2C and Figure 3B). Once the wire was routed through and through the fabric of the stent graft, the spinal needle was removed (Figure 3C). Three Z stent peaks or six Z stent struts were constrained at a time to avoid infolding of the stent graft (Figure 3, D to F). Two nonlocking 3-0 polypropylene loops were used for each stent, as demonstrated in Figure 3F (inset). The first loop was placed around the nitinol wire (see Figure 3D), and the second loop was routed around the first polypropylene loop (see Figure 3E and inset), with careful attention not to place the suture through the first polypropylene loop (see Figure 3E, inset), which would permanently constrain the device. The nitinol wire was then repositioned into the inner cannula (see Figure 2C and Figure 3G) to prevent the “wind sock” effect during stent graft deployment. All the Z stents were constrained (see Figure 2C and Figure 3G), which allowed a 30% reduction in the diameter of the stent graft (see Figure 2, B and D). The modified stent graft was resheathed into its original sheath using 2-0 silk ties as previously described. 6

Technique of creation of a diameter-reducing wire in the TX2 stent graft. The inner cannula of the stent graft is opened with a scalpel (A, inset), and one of the nitinol wires is retrieved and rerouted posteriorly through and through the fabric of the stent graft using a long 22-gauge spinal needle (B). Once the wire is in place (C), the Z stents are constrained using loops of polypropylene. The first loop was placed around the stainless steel wire (D), and the second loop was routed around the first polypropylene loop (E), with careful attention not to place the suture through the first polypropylene loop (F, inset). The nitinol wire is then relocated into the cannula (G). Reprinted with permission of Mayo Foundation for Medical Education and Research. All rights reserved.
Device Implantation
The patient was admitted the day prior to the procedure for intravenous hydration, bowel preparation, and oral acetylcysteine. The procedure was performed using general endotracheal anesthesia in a hybrid endovascular suite with a fixed imaging unit. Diluted contrast agent (50:50 with normal saline) was used for selective angiography. An activated clotting time of > 300 seconds was maintained throughout the entire case.
Right femoral access was established using 0.035-inch Lunderquist wire (Cook Medical) and a 24F Check-Flo sheath (Cook Medical). The 24F sheath was accessed with three 7F Ansel II sheaths (Cook Medical) for selective side branch catheterization. The renal and superior mesenteric arteries were catheterized via the femoral approach and the celiac axis via the brachial approach (Figure 4A). The surgeon-modified fenestrated TX2 stent graft was oriented extracorporeally and introduced via the left femoral approach over a 0.035-inch Lunderquist wire. The device was deployed with perfect apposition between the fenestrations and the marker catheters (Figure 4B). The diameter-reducing wire allowed movement of the TX2 stent graft. With the stent graft constrained, the celiac fenestration was catheterized via the brachial approach and the renal and superior mesenteric arteries via the femoral approach. Hydrophilic 7F sheaths (Cook Medical) and a bridging iCAST stent graft (Atrium, Hudson, NH) were positioned within each of the four side branches (see Figure 4B). The diameter-reducing wire allowed the constrained modified stent graft to be moved in the axial and longitudinal planes during catheterization of the side branches. Once the side branch stent grafts were ready for deployment, the nitinol wires were removed, including the diameter-reducing wire. Once the stent graft was unconstrained, each of the balloon-expandable stent grafts was deployed and flared using a 10 mm × 2 cm balloon (Figure 4C). Selective branch angiography was performed to confirm patency (Figure 4D) followed by completion aortography, which showed no endoleak. The patient had an uncomplicated postoperative course and was dismissed on postoperative day 6.
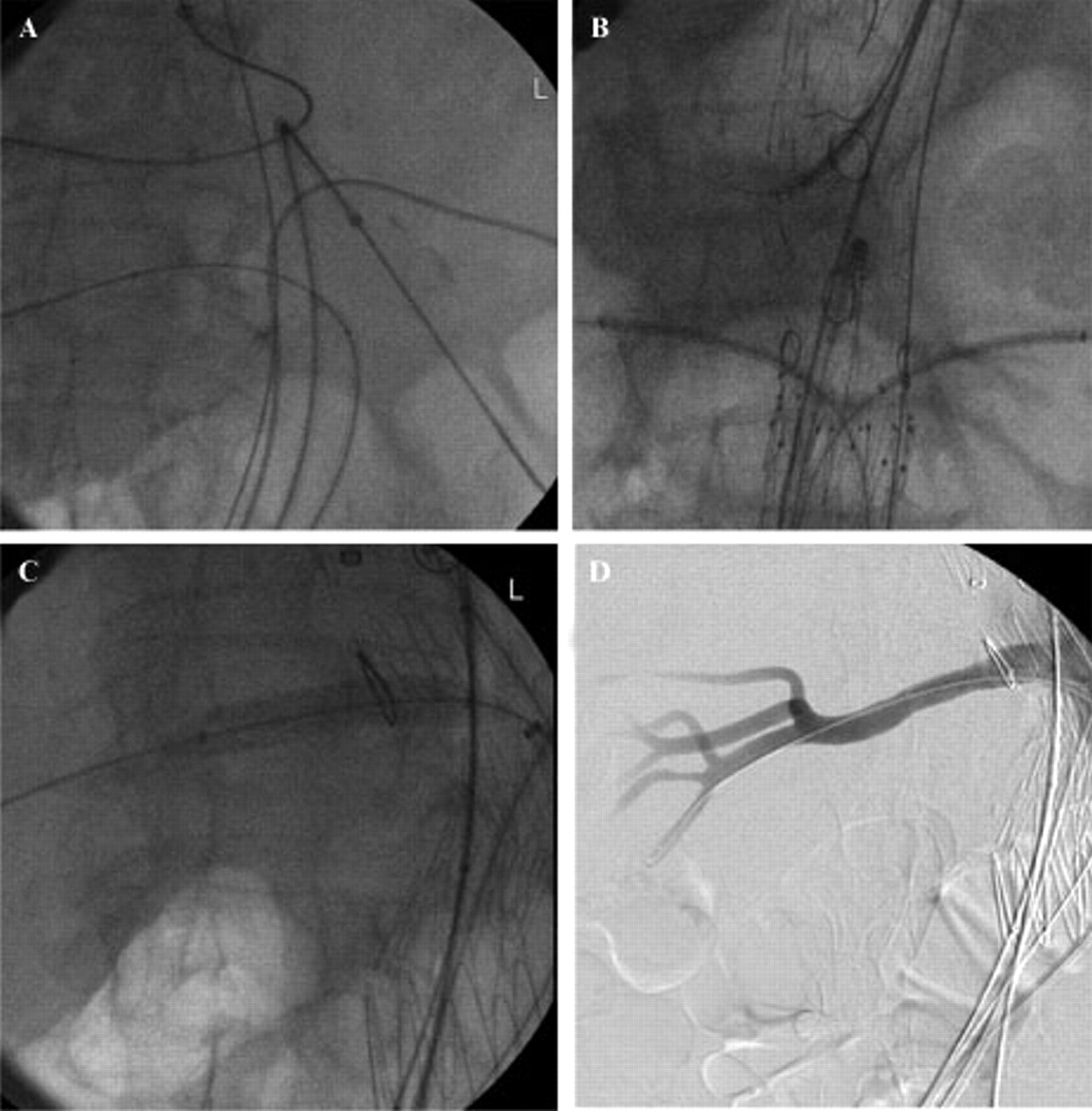
The four vessels are catheterized to facilitate orientation and minimize use of contrast agent(A). Once the vessels are located, the modified fenestrated stent graft is oriented and deployed (B). Each fenestration is catheterized, followed by placement of hydrophilic sheaths and balloon-expandable stent grafts (B). Once all four vessels are secured, the diameter-reducing wire is removed, and each side branch stent is deployed (C). Selective angiography confirms patency (D).
Discussion
One limitation of fenestrated stent grafts is the need for accurate design and device implantation. The addition of a diameter-reducing wire has greatly facilitated the precise implantation of industry-manufactured fenestrated stent grafts by allowing rotational and longitudinal movement of the stent graft. 1 This technique remediates problems related to misalignment of the main stent graft in relation to the target vessel, which could result in loss of a side branch. Several caveats to the technique of surgeon-modified fenestrated stent grafts with diameter-reducing wire deserve mention.
The same principles that are currently used for planning and implanting manufactured fenestrated devices are used for modified stent grafts. Anatomic limitations are excessive aortic tortuosity, the presence of multiple or small arteries, and chronic dissections with vessels arising from separate lumens. The proximal landing zone should not be compromised with modified stent grafts, and a length of at least 2 cm of “normal,” noncalcified, parallel aortic wall is recommended. The device is designed using length measurements and axial orientation obtained from computed tomographic angiography and centerline of flow analysis. A limitation of the modified technique is that there is no quality control in the planning process of the procedure; therefore, one relies on the experience a surgeon has in designing and implanting fenestrated stent grafts.
The diameter-reducing wire improves the ability to move the stent graft in the longitudinal or axial axis, which translates into the ability to compensate for errors of design and deployment. However, the ability to torque or rotate the TX2 device is limited in patients with excessive iliac tortuosity or in the aortic arch. One advantage of using a constrained stent graft is that the reduced diameter of the stent graft allows blood flow between the stent graft and the aortic wall, which may decrease renal and visceral ischemia and may allow catheter manipulations outside the stent graft in the event of device misalignment. Often a curved catheter such as the Simmons or Sos catheter may be formed via the fenestration and outside the stent graft, which allows catheterization of down-going vessels from a femoral approach. In the case of the TX2 device, one of the nitinol wires located in the inner cannula is used for the modification. It is imperative that the wire not be grasped with a forceps or hemostat as this results in fracture of the nitinol wire, similar to what would occur with a polypropylene suture. The nitinol wire has the advantage of being resistant to kinks, which facilitates withdrawal of the wire after deployment. Another caveat is the careful placement of the polypropylene ties to avoid permanently constraining the device. The average time for modification is 2 hours for a four-vessel stent graft with constraining wire.
The use of modified fenestrated devices is off label and is not recommended in centers that have access to a manufactured device or in patients who are candidates for open surgical repair. Several other limitations of this approach deserve to be mentioned. The manipulations of the stent graft could result in device contamination, although that is also true for fashioning a trifurcated graft in patients undergoing debranching procedures. There is no quality control in the design process, which is largely dependent on the surgeon's experience with fenestrated endografts and probably is the most critical aspect determining a successful repair. The durability of the fenestrations has not been tested, and the rates of endoleak may be higher than those reported for manufactured devices.
At our institution, modified stent grafts have been offered as an alternative to surgical debranching in patients with complex aneurysms who are considered unfit for conventional open repair because of severe cardiac, pulmonary, and/or renal dysfunction or hostile anatomy. The patients are not participants of a research protocol, which would require an IDE. We have presented our results comparing the use of modified fenestrated stent grafts with abdominal debranching in high-risk patients with complex aortic aneurysms. 7 In this study, the first 30 high-risk patients treated with modified fenestrated stent grafts were compared to 16 patients treated with debranching. These patients accounted for 23% of 198 patients who were treated for juxtarenal, suprarenal, or thoracoabdominal aneurysms during the study period.
The modified fenestrated devices were performed using one- to four-vessel fenestrations, as well as iliac side branch grafts to the internal iliac artery, most often without the diameter-reducing wire. Eighty-five fenestrations were created, including 50 renals, 33 mesenteric, and 2 hypogastric. The mean time for device modification was 45 ± 32 minutes. Patients in both groups had similar cardiovascular risk factors, with the exception of more patients with positive stress-induced cardiac ischemia and preoperative renal insufficiency in the fenestrated group. Conversely, there were more patients with renal involvement (56% versus 19%) and fewer patients with thoracoabdominal extension (47% versus 81%) in the fenestrated group. Importantly, the number of patients who had one and two vessels (48% versus 47%) or three and four vessels revascularized (52% versus 53%) was nearly identical between groups.
Technical success for branch artery stenting was 98%, with 83 of the 85 arteries successfully stented. The modified fenestrated technique was associated with substantially higher fluoroscopy time (mean 157 ± 59 minutes) and contrast use (241 ± 105 mL) but significantly less blood loss, fluid requirements, and total operative time, which averaged 5 hours. It is possible that the use of a constrained device would have decreased fluoroscopy times.
There were four 30-day deaths for the entire cohort, one after modified fenestrated (3.3%) and three after debranching (19%) procedures. All four deaths occurred among patients with thoracoabdominal aneurysms. The incidence of complications with fenestrated stent grafts was 37% compared to 73% for debranching. The median follow-up was 14 months. Primary branch or target vessel patency at 1 year was 97% for branched stent grafts and 98% for debranching procedures. Freedom from endoleak was 88% and 74% at the same interval, respectively. There were no patients with sac enlargement, rupture, or conversion in the fenestrated group. However, longer follow-up is needed to assess the durability of the modifications.
Conclusion
Modification of aortic stent grafts with fenestrations, scallops, and a diameter-reducing wire offers an alternative to surgical debranching in high-risk patients who are not candidates for open conventional repair and do not have access to a manufactured device. The constrained surgeon-modified stent graft has the advantages of rotational and longitudinal movement, which facilitates catheterization and stenting of side branches.
Footnotes
Acknowledgment
Dr. Oderich has a consultant agreement with Cook Medical.