
Abstract
The purpose of this study was to evaluate clinical outcomes of combined endovascular and open techniques to eradicate false lumen dilatation in the visceral aortic segment after type B aortic dissection associated with aortic aneurysm. We reviewed eight patients with distal thoracic and abdominal false lumen dilatation treated with a staged procedure. These included arch debranching as needed, proximal thoracic endovascular repair, and open surgical correction with abdominal aortic replacement of the visceral and infrarenal aorta. False lumen eradication was successful in all patients. There were no operative deaths, and paraplegia or paraparesis occurred in two patients. During a mean follow-up of 30 months, no complications or secondary interventions were necessary. The thoracic false lumen remained thrombosed in all patients, with no evidence of aortic dilatation or stent graft complications. Complete thrombosis and eradication of the false lumen can be achieved through a three-stage repair of chronic type B aortic dissection with aneurysmal dilatation. A prospective randomized trial is needed to establish the viability of this approach versus standard open repair of type II thoracoabdominal aortic aneurysms.
Aortic dissections of the thoracic aorta are common pathologies and continue to be lethal despite progress in medical and surgical therapy. 1 Incidence is estimated at 2 to 4 cases/100,000/year, and the prevalence at necropsy is approximately 1.1 to 1.5%. Furthermore, 21% of patients with acute aortic dissections die before reaching a hospital. 2 Until the last several years, the treatment for type B aortic dissections has been medically oriented, involving blood pressure control and stress reduction. 3–5 Early treatment with either surgical or endovascular methods is reserved for those patients who develop vascular complications such as persistent or recurrent pain, rapid aortic expansion, rupture, or malperfusion syndrome. However, this is not a benign approach as failures and complications do occur during the natural history of the disease despite appropriate medical management. It is estimated that 20 to 40% of the patients who survive the acute phase may develop significant aortic dilatation. 6
In patients with chronic dissections, the approach of excluding the proximal entry tear and additional significant distal thoracic communications is often an effective procedure with the predictable results of false lumen thrombosis, thoracic aneurysm shrinkage, and absence of abdominal aortic dilatation (Figure 1). However, the false lumen can often remain patent, resulting in possible dilatation. 7–9 Lastly, after years of medical therapy, some patients develop dilatation of the thoracoabdominal aorta. Although impressive results have been achieved in centers of excellence, graft replacement of such extensive disease still carries a high morbidity and mortality rate in other centers. 10,11 We have adopted a multistaged approach consisting of a planned three-step procedure combining extra-anatomic proximal reconstruction, endovascular grafting, and standard open surgical techniques.
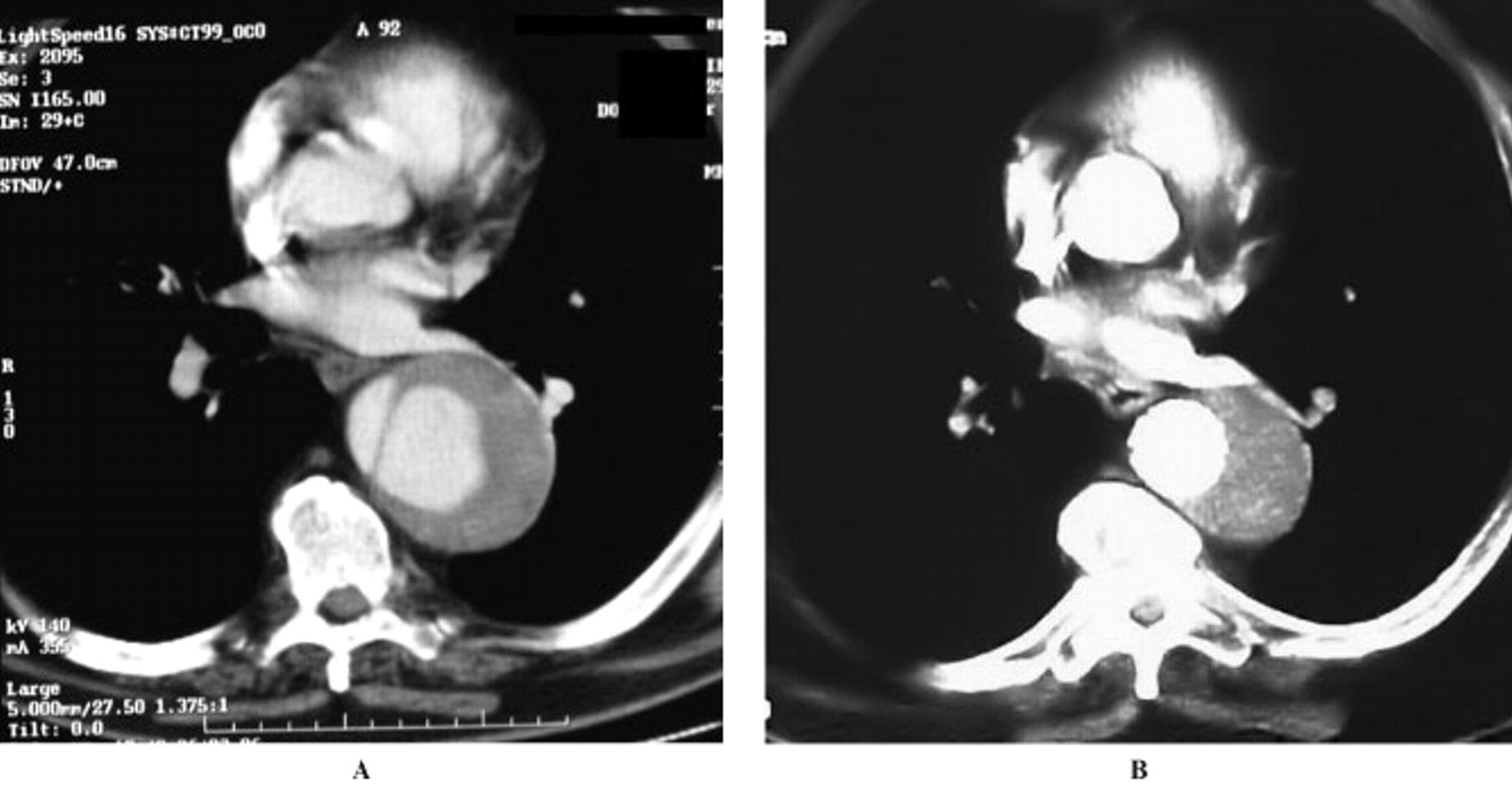
Chronic type B dissection: preoperative (A) and 4-year postoperative (B) computed tomographic scans.
Methods
From May 1998 to December 2008, the Vascular Surgery Unit at San Filippo Neri Hospital treated 152 patients with thoracic aortic pathologies. The pathologic entities treated included thoracic aortic aneurysms in 65 patients (42.7%), chronic aortic dissections in 47 (30.9%), acute type B dissections in 17 (11.1%), pseudoaneurysms in 13 (8.5%), penetrating aortic ulcer in 5 (3.3%), aortic coarctation in 3 (2.0%), and aortic graft infection in 2 (1.3%). Preoperative evaluation was done by thin-cut computed tomography (CT) and/or magnetic resonance angiography.
Among patients treated for chronic type B aortic dissection, despite entry tear coverage, we failed to achieve the expected results of false lumen thrombosis, true lumen dilatation, and aneurysmal sac shrinkage in three patients. In these patients, we observed a progressive increase in aortic diameter during follow-up. Aortic dilatation occurred at multiple levels in the aorta. Moreover, five patients were admitted for chronic type B aortic dissection with aneurysmal dilatation of the thoracic and the abdominal aorta. Two of these were followed at our institution and developed rapid enlargement of the aorta 3 and 4 years after the initial dissection episode.
The mean age of these eight patients was 57 ± 7.6 years (range 45–67 years), and the mean aortic diameter was 74.2 ± 18.3 mm (range 55–110 mm) (Table 1). Staged hybrid treatment was performed in all patients (Figure 2). The clinical presentation and details of surgery are summarized in Table 2.

Staged hybrid technique. A, Chronic dissection with aneurysmal dilatation of the thoracic and abdominal aorta. B, Left subclavian artery transposition and endovascular stent graft exclusion. C, Surgical open repair via a thoracophrenolaparotomy. The proximal anastomosis is end to end between the endograft and a standard Dacron graft.
Patient Demographics and Medical Characteristics
Clinical Presentation and Type of Surgery
TAA = thoracoabdominal aortic aneurysm.
First Stage
The first stage was the transposition of supra-aortic trunks to provide a suitable and secure proximal neck in seven patients, with either a carotid-subclavian transposition/bypass in four patients or retropharyngeal carotid-carotid/carotid-subclavian bypass in three patients to provide a neck length longer than 2 cm. Proximal debranching was unnecessary in one patient, who was previously treated for a type B aortic dissection with a short thoracic resection and graft interposition. In this patient, the proximal landing zone was the graft itself.
Patients who received a bypass were later submitted to percutaneous embolization of the origin of the left subclavian artery to avoid a reperfusion endoleak, according to a previously described technique. 12 Patients submitted to a carotid-carotid-subclavian bypass had their proximal left common carotid artery sectioned and sutured for the same reason. The distal end was then transposed on the graft.
Second Stage
The second stage involved endovascular exclusion of the thoracic dissection. The stent grafts used included the Gore Excluder and Gore TAG devices (W.L. Gore, Flagstaff, AZ) in six patients and the Bolton Relay endograft (Bolton Medical, Sunrise, FL) in two patients. The endovascular procedures were conducted under general anesthesia with a surgical femoral access in all but one case, where an abdominal access was performed.
Thoracic endografting was quite extensive in six patients, with the more distal endograft landing 5 to 10 cm above the celiac trunk. Laterolateral angiography was performed to determine the origin of the celiac trunk, and the last device was positioned with the distal end from 5 to 10 cm above the celiac trunk. A minimum of two devices were needed for each patient. During this step, spinal fluid drainage was not used.
In the remaining two patients, thoracic endografting was less extensive, covering approximately 20 cm of the thoracic aorta. In fact, in these two patients, the distal thoracic and visceral aorta was dissected but not aneurysmal, whereas the infrarenal aorta was dilated. These two patients had only the infrarenal aorta subsequently replaced.
Third Stage
Lastly, surgical repair of a type IV thoracoabdominal aortic aneurysm via a thoracophrenolaparotomy through the seventh or eighth intercostal space was conducted. The proximal clamp was always placed on the distal thoracic aorta, clamping together the aortic wall and the stent graft inside. During this last phase, the aorta at the diaphragm level was replaced by a standard Dacron graft, with a proximal end-to-end anastomosis with the stent graft. The anastomosis was reinforced by a triple-layer suture comprising the stent graft fabric, the aortic wall, and a Teflon felt.
Reimplantation of visceral arteries was accomplished with a visceral inclusion patch and reimplantation of the left renal artery via the Carrel technique. Spinal fluid drainage was routinely used, as well as femorofemoral bypass, allowing for lower limb and visceral artery perfusion during the proximal anastomosis (Figure 3). No hypothermic arrest was required for the repairs.

Intraoperative photograph showing the “hybrid” anastomosis.
This entire procedure, which we define as the standard approach, was applied in five patients. In three other cases, we were able to reduce the magnitude of the intervention.
In one case, all the visceral vessels originated from the true lumen and no viscerally located false communications could be detected. After left subclavian transposition and endovascular thoracic exclusion (Gore TAG), we performed a thoracophrenolaparotomy, opened the false channel, and confirmed that multiple reentries were located infrarenally. We were therefore able to move the clamp to the infrarenal aorta, which was replaced with a bifurcated Dacron graft.
The remaining two patients had a normal distal thoracic and visceral aorta diameter, even if dissected. As mentioned above, these two patients had an abdominal access only.
In the first case, the patient developed dilatation of her thoracic and infrarenal abdominal aorta and true lumen collapse 4 years after the initial symptoms. Furthermore, her anatomy was complicated by an extremely tortuous patent left iliac artery and a contralateral iliac occlusion. To obtain a suitable proximal neck, hemiarch transposition was performed via a retropharyngeal conduit and later open repair of the abdominal aortic aneurysm was performed to address the access issues. During the aneurysm repair, the septum was excised up to the infrarenal clamp and proximal anastomosis was carried out with Teflon felt–buttressed sutures. One limb of a bifurcated infrarenal Dacron graft was then used as a conduit for the thoracic stent graft (Bolton Relay).
In the second case, the patient developed an aneurysmal dilatation of the infrarenal abdominal aorta 6 years after a carotid-subclavian bypass and endovascular exclusion of a chronic type B aortic dissection. The thoracic false lumen was almost thrombosed at the thoracic level with a reduction in overall diameter, but the false lumen in the visceral and abdominal aorta remained patent. In this last case, the dilated infrarenal aorta was replaced with a bifurcated Dacron graft via a retroperitoneal approach. In the two patients who did not receive a complete aortic repair, the distal thoracic and visceral aorta, which is not dilated, is now under close surveillance.
Results
There were no operative deaths. Two patients developed paraplegia.
No significant morbidity occurred after supra-aortic trunk transposition. Immediate extubation and 1-day intensive care unit (ICU) stay were the standard postoperative care for the seven patients who needed lengthening of the proximal thoracic neck. Minor complications consisted of transient left diaphragm palsy (not symptomatic) in three cases and wound lymphorrhea in one case.
Similar benign outcomes were recorded in the eight patients after thoracic endografting, except for one patient who experienced lower extremity weakness on the second day after thoracic endograft exclusion. After aggressive spinal fluid drainage, the symptoms of spinal cord ischemia improved significantly, and he was able to walk without assistance 3 months later. The ICU stay was 5 days in this case. Following his recovery, he underwent the thoracoabdominal open procedure without recurrence of his symptoms.
The last step included six thoracoabdominal and two abdominal open procedures. One patient developed paraplegia on the second day after the thoracoabdominal intervention. Despite spinal fluid drainage, the patient did not recover from paraplegia. One patient required reintervention for abdominal hemorrhage 2 days after the thoracoabdominal procedure, without sequelae, and one patient required iliac stenting for a dissection.
The mean operative time was 283.3 ± 29.4 minutes. The extubation was possible on the first postoperative day in all but one patient (mean 19.7 ± 8.0 hours), and the ICU stay was 3.2 ± 1.2 days. All patients were available for clinical and imaging follow-up. Angiodynamic CT scan was also performed in cases of hybrid anastomosis to verify the integrity of the endograft during follow-up. All patients were alive without endovascular or open complications with a mean follow-up of 30 months (29.8 ± 19.3 months). Of note, imaging demonstrated complete exclusion of the thoracic aneurysm in all cases, and the diameter of the thoracic aorta remained stable or decreased in the residual thoracic segment.
Discussion
The long-term outcome of aortic dissections remains somewhat poorly defined. Unfortunately, surviving the initial onset of an aortic dissection does not guarantee freedom from subsequent aortic events, such as aortic aneurysm formation, rupture, and extension of dissection, that may lead to end-organ ischemia. 13 This risk of long-term complications involves both patients with medically treated uncomplicated type B aortic dissections and patients with type A aortic dissections who have undergone successful replacement of the ascending aorta but have persistent patency of the false channel at the descending thoracic and/or abdominal aortic level. 14–16 Even patients who successfully submit to open interposition aortic repair for complicated type B aortic dissections are not immune from possible long-term complications owing to persistent false lumen filling via distal communications.
Endovascular treatment is emerging as a viable alternative to conventional surgery for thoracic aortic pathologies because of its favorable risk profile and less invasive nature, 17–21 but it leaves the distal thoracic aorta untreated. Changes in hemodynamic forces usually protect the abdominal aorta from further dilatation, promoting an aortic remodeling (false lumen thrombosis, true lumen expansion, thoracic aneurysmal sac shrinkage). However, in some cases, this approach fails to induce thrombosis of the celiac and abdominal false lumen, which may dilate. 22,23 Recently, the implications of partial false lumen thrombosis have been published, estimating a relative risk of 2.7 compared to patients with a completely patent false lumen. 24
Proximal thoracic stent grafting fails to abolish the false lumen in about 15 to 25% of patients, suggesting that perhaps it may not be a definitive solution for all type B aortic dissections. 20,25,26 Eggebrecht and colleagues performed their meta-analysis on 609 patients submitted to endovascular stent grafting for aortic dissection. 27 False lumen thrombosis was reported in 75.5% of patients. In 2.5% of patients, late surgical conversion was required; in 4.6% of patients, secondary endovascular stent graft procedures were performed, for a total reintervention rate of 12% at a follow-up period of 20 months.
Recently published registry data from the International Registry of Acute Aortic Dissection (IRAD) show a mortality of 25% at 3 years in patients discharged alive from the hospital. 13 This high mortality at 3 years exceeds other disease mortality, such as coronary artery disease, chronic obstructive pulmonary disease, and stage II colon cancer. 16,28 Furthermore, this long-term mortality is mainly due to complications of the dissection, such as rupture, extension of the dissection, and perioperative mortality from subsequent aortic or vascular repairs. 29–31 Interestingly, there seems to be no significant difference in long-term mortality in the group of patients discharged alive, regardless of the in-hospital management modality: surgery or endovascular or medical procedures. Clinical and anatomic predictors of false lumen dilatation are also lacking, so, even in the presence of a thrombosed false lumen, the distal thoracic and abdominal aorta may grow in diameter during follow-up, accounting for the continued risk of aortic rupture (about 2%) and the need for lifelong clinical and imaging follow-up.
In spite of the impressive results in centers of excellence, graft replacement of such extensive disease across most hospitals carries a high mortality rate, thereby motivating the desire to develop other, less invasive methods. Some authors have devised ancillary minimally invasive techniques, such as the PETTICOAT and stable procedures, to deal with the problem of dissected false lumen after thoracic stent grafting in an attempt to completely repair the distal dissected segments without compromising important side branches. 32,33 But multiple communications between true and false lumen preclude complete false lumen exclusion.
Single centers have reported the combination of endovascular exclusion with visceral revascularization for treatment of extensive thoracoabdominal aortic aneurysms. This technique consists of a retrograde revascularization of the visceral and renal arteries via an abdominal approach, allowing for stent graft positioning and exclusion of thoracoabdominal aneurysm by extending into the visceral aorta. However, the rate of complications in this approach is not negligible, with a 13% mortality and a 58% morbidity rate reported by Black and colleagues. 34
To minimize surgical invasiveness, we adopted a multistaged approach consisting of a three-step planned combination of extra-anatomic proximal reconstruction, endovascular grafting, and classic open surgery procedure. These interventions carry quite a high risk of paraplegia; therefore, it is always necessary to preserve the flow in the left subclavian artery. Our technique provides a hybrid anastomosis at the lower third of the descending thoracic aorta, and in these cases, it is difficult to reimplant patent intercostal arteries. Therefore, left subclavian artery revascularization is mandatory.
This approach appears feasible and safe, although it remains a major operation. This approach results in a definitive repair with a much lower thoracotomy, leading to lesser pulmonary compromise and avoidance of barotrauma from left lung isolation. In some cases, it may even require only abdominal access.
One drawback may be the potential risk of paraplegia because it remains very difficult to reimplant patent critical intercostal arteries. In this subgroup of patients, we had two cases of paraplegia: one after endograft thoracic exclusion that completely regressed after 3 months and the second after the thoracoabdominal procedure with an incomplete recovery. In the last case, the etiology was probably multifactorial rather than linked solely to intercostal or lumbar artery occlusion. In fact, in this patient, clamp time lasted longer and intraoperative bleeding was more than expected. This corresponds to the theory that neurologic complications after thoracic open surgery are more closely related to the aortic cross-clamp time, concomitant mesenteric ischemia, and reduced spinal cord perfusion. 35
Another potential inconvenience may be the mismatch between the caliber of the endograft and that of the standard Dacron graft, which is usually smaller in size. This technical issue can be resolved using the triple-layer suture, which provides extra strength.
Lastly, the use of the femorofemoral bypass requires more heparin than the left heart bypass. In our opinion, femorofemoral bypass is easier, and in our experience, it can be performed by administering a low dose of heparin and maintaining an activated clotting time of 150 to 200 seconds so that this potential drawback can be minimized, and it is balanced by the great advantage of a less invasive lower thoracotomy.
This initial experience has been successful so far but is still evolving. In particular, the hybrid anastomosis between the endograft and the Dacron graft needs close observation (Figure 4). Although we have observed no device fatigue on follow-up imaging from our first case performed more than 5 years ago, a longer follow-up is still needed. Using the native aorta as buttressing tissue at the anastomosis may help mitigate this risk.

Computed tomographic scan reconstruction of the hybrid anastomosis. The arrow and the dashed line indicated the suture line.
We adopted two distinct types of repair in our patients. One approach was a hybrid repair of the entire descending thoracic and abdominal aorta, whereas in the second one, the visceral segment of the aorta was left untreated. This aortic segment also requires close monitoring.
Finally, we used this technique in dissecting patients only, where the endograft is well fixed along all of the narrow aortic true lumen. We cannot suggest it for atherosclerotic aneurysms because of the lack of a secure distal sealing zone.
Conclusion
Hybrid aortic replacement techniques demonstrate promising results in the treatment of chronic type B aortic dissections with complete thrombosis and eradication of the false lumen. Our technique takes advantage of thoracic aortic endografting to reduce the scope of the open distal aortic surgery. Although lifelong surveillance is still needed, this technique provides a less invasive alternative in this difficult patient population and may compare favorably to the standard thoracoabdominal aortic replacement results to be expected outside high-volume centers.
Footnotes
Acknowledgments
We thank Laura Torchiani for her drawings.
Financial disclosure of authors and reviewers: None reported.