
Abstract

In 2009, Professor Frans Moll and Professor Giorgio Biasi considered the opportunity to set up a survey on indications for the treatment of carotid bifurcation stenosis for the prevention of stroke. The idea derived from the consideration that what happens in the “real world” is totally different from the results of randomized controlled trials and well-designed and well-conducted observational studies. For example, the role of endovascular versus surgical treatment for carotid stenosis is still strongly debated, and the criteria for indications to stenting and endarterectomy are pretty subjective. In their capacity as presidents of, respectively, the European Society for Vascular Surgery (ESVS) and the International Society for Vascular Surgery (ISVS), Professors Moll and Biasi, with the collaboration of Dr. Alberto Froio from the University of Milano-Bicocca, Italy, and Dr. Gert Jan de Borst from the University of Utrecht, the Netherlands, prepared a questionnaire to be distributed to most of the vascular surgery community worldwide. This article describes the rationale for and design of the joint survey by the ISVS and the ESVS.
As a mechanism for obtaining information and opinion, questionnaires have a number of advantages compared to other evaluation tools: (1) nearly everyone has some experience completing questionnaires; (2) questionnaires are easy to analyze when properly designed; (3) they are very cost effective, especially for studies involving large sample sizes and large geographic areas; (4) bias is reduced by uniform question presentation; and (5) data collection is performed anonymously.
On the other hand, questionnaires have the disadvantage of being impersonal, and a bad design may lead to misinterpretation, rendering the answers useless. Open questions can take a lot of time to collect and analyze, and people are not always willing or able to respond because the survey is too complicated or asks for information unlikely to be available to the respondent. Whatever their form, to get useful responses, it is important to be clear about the aim of the questionnaire and how the response will help improve learning technology.
However, there are more than just advantages and disadvantages. Although we continue to discover new treatments, it is even more important to take what we already know and apply effective strategies to our practices (Figure 1). First, we perform clinical trials and use the outcomes of these trials to develop guidelines. Then, to be sure that what we are promoting is actually the “best option,” we must be able to measure what we are doing. Here there is an important opportunity for questionnaires, as a measurement instrument, to provide feedback to the practicing community. If we are successful in all of this, outcomes can be improved. So it seems that a questionnaire is a necessary and valuable tool in the cycle of clinical therapy in general and in the translation of clinical trials into practice in particular.
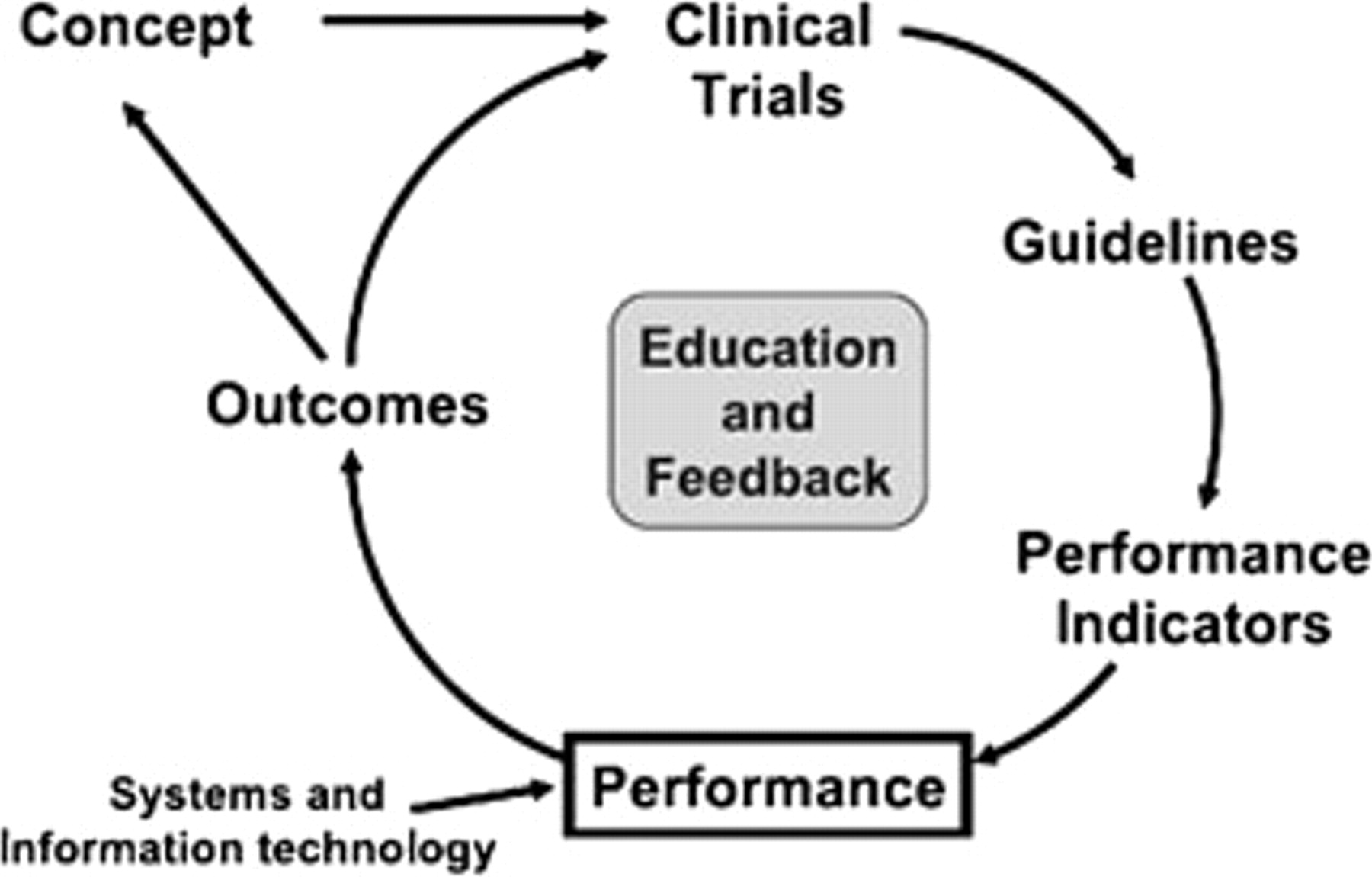
Reproduced with permission from Califf RM. Translating clinical trials into practice. Heart Inst J 2006;33:192–6. Copyright 2006, Texas Heart Institute, Houston. Reprinted with permission.
But unforeseen factors may influence the relationship between questionnaires and clinical practice. One of these unforeseen factors is the self-awareness of the responder. The purpose of an interesting and somewhat peculiar study in Houston, Texas, was to determine whether adolescent boys could make a correct self-report of their circumcision status. 1 During a physical examination, 1,508 adolescents were asked whether they were circumcised; of these, 49% had full, 1% had partial, and 50% had no circumcision. Of the 738 fully circumcised boys, only 512 (69%) considered themselves circumcised, and 24% did not have a clue. Conversely, of the uncircumcised youth, 4% reported being circumcised, and 31% did not know. In conclusion, there was a clear level of disagreement between the adolescents' opinions and the clinicians' observations. In this population, self-report of circumcision status did not result in accurate information, and disturbed self-awareness was a limiting factor.
Another unforeseen factor might be the influence of role models, who are also believed to influence the behavior of the general public, including health care decisions. In the United States, a gradual increase occurred in the mid-1980s in the use of breast-conserving surgery (BCS), supported by doctors' advice. However, when confronted with breast cancer suitable for BCS, Nancy Reagan chose to have a mastectomy. With the help of a questionnaire, Nattinger and colleagues determined the temporal association between the nationwide choice for BCS and Mrs. Reagan's mastectomy. 2 Compared to the third quarter (just before Mrs. Reagan's mastectomy), women were 25% less likely to undergo BCS in the fourth quarter. In subsequent quarters, the rate gradually returned to baseline. Clearly, role models can influence decisions about medical care, potentially disturbing guidelines for current medical practice by negative feedback.
On the other hand, when a survey is created, positive feedback on the initial list of questions may be obtained from a small but representative sample of potential responders. Positive reinforcement can also be obtained by choosing the right group of respondents. To direct the survey to people being trained and experienced in the procedure (carotid endarterectomy [CEA] or carotid artery stenting), and by their participation in this particular specialty society, it may be assumed that they have a special interest in the topic being surveyed. 3
In 2000, the Dutch Bypass Oral anticoagulants or Aspirin (BOA) trial provided level A evidence on antithrombotic treatment after peripheral bypass surgery.
4
Accordingly, in venous grafts, oral anticoagulants (OACs) are significantly better for bypass patency than aspirin. In nonvenous grafts, aspirin is significantly better than OAC. To analyze the behavior of prescription of antithrombotics in Europe, all ESVS members were sent an electronic invitation in 2007 to participate in a Web-based survey. Overall, independent of the type of bypass, aspirin was prescribed in 50% of procedures, especially for femoropopliteal bypasses, and OAC in 22%, especially for femorocrural bypasses. The type of bypass and material did not seem to influence the choice of antithrombotic type being prescribed. These (unpublished) data showed the following:
A highly heterogeneous antithrombotic preference was noted within Europe Clinicians in northern Europe prescribed the most aspirin, independent of the type of bypass Only in western and central Europe was OAC preferred for venous bypass A similar trend was found for nonvenous bypasses
This ESVS questionnaire clearly presented insight into the (1) low compliance with antithrombotic treatment and (2) large heterogeneity within Europe among vascular surgeons' preference for antithrombotic drug treatment for patients after infrainguinal bypass surgery.
Within the field of vascular surgery, questionnaires have also been effective in preparing candidates for vascular training programs 5 and in evaluating the influence of training paradigms after the introduction of independent certification in vascular surgery on the actual practice of endovascular therapy among European countries. 6 In another study, with the help of a questionnaire, Farber and colleagues showed a significant knowledge deficit among both the general population and medical students about the field of vascular surgery and, in particular, the daily work of a vascular surgeon. 7 All of these examples provide the necessary feedback for vascular surgical societies to create or adjust the course of their future strategies.
The Society for Vascular Surgery (SVS) and the ESVS have both recently published guidelines for the management of carotid artery atherosclerosis. 8,9 Although the documents differ slightly in the methods used and in the level of detail, they reveal trans-Atlantic consensus in most areas regarding the role of CEA in the management of both symptomatic and asymptomatic patients. 10 It is of the utmost importance to determine whether these published practice guidelines are being followed in patients undergoing carotid revascularization. This is of particular interest in this era, in which carotid surgery has repeatedly been challenged by endovascular alternatives. 11,12 Although some information about regional practice patterns regarding CEA has been reported, 13 no large-scale assessment of the practice patterns of vascular surgeons has been conducted. The present survey is directed at the practice patterns of specialists with regard to carotid revascularization, focusing on treatment indications. 13 It will be the most extensive assessment of this aspect of carotid revascularization, and it is unique in its specific focus on subspecialty–trained, clinically active vascular surgeons' preferences and current attitudes within the membership of the ISVS and the ESVS. By their participation in these particular specialty societies, it may be assumed that potential responders have a special interest in clinical vascular treatment. 14
The questionnaire was constructed using closed-ended questions (Supplementary Material), provided with electronic guidance so that none of the questions can be missed. The survey was placed on an independent study Web site (<http://www.vascularsurvey.com>), and the questions were piloted by a small group of colleagues. Nonresponders are sent a reminder every 2 weeks.
In this questionnaire, supported by the boards of both ESVS and ISVS, traditional practice is balanced against the published consensus statements on appropriate indications for carotid revascularization. The survey's principal purpose and the large size of the survey group should give a good overall assessment of the attitudes and practice patterns of experienced vascular surgeons. This type of information needs to be considered in the development of clinical pathways for practice in managed care environments. The aim is to present analysis of the survey data at the ISVS and ESVS meetings in 2011. To better establish current practice patterns and to characterize vascular specialists' opinions about the role of current guidelines on the management of carotid artery disease, the ESVS and ISVS membership is kindly invited to fill in this Web-based questionnaire (<http://www.vascularsurvey.com>).
Footnotes
Acknowledgments
Preparation of the ISVS/ESVS survey Web site was finalized under the endorsement of the Associazione per la Ricerca pre-clinica e clinica, la Prevenzione e il Trattamento delle Malattie Cardio-Vascolari.
This paper was submitted simultaneously to Vascular and the European Journal of Vascular and Endovascular Surgery.
Financial disclosure of authors: Preparation of the survey Web site was sponsored by Cook Medical.
Financial disclosure of reviewers: None reported.